





Abstract
Symptoms of hypersensitivity pneumonitis and massive pulmonary haemorrhage occurred in a 24-yr-old male shortly after occupational exposure to naphthylene-1,5-diisocyanate (NDI).
The present examination was performed ∼1-yr after the initial life-threatening haemoptysis and following an uneventful recovery after resection of the middle lobe, which had been identified bronchoscopically as the bleeding source. Histological re-examination of the lung was compatible with hypersensitivity pneumonitis.
After a chamber challenge with NDI (5 parts per billion (ppb) for 10 min, 10 ppb for 110 min), rales were heard in both lungs, and a fall in vital capacity and partial pressure of arterial oxygen as well as a rise in body temperature were documented. Isocyanate-specific immunoglobulin-G antibodies could not be detected in the patient's serum, possibly due to the long period without exposure to isocyanates.
The authors conclude that naphthylene-1,5-diisocyanate may cause immunological pulmonary haemorrhage. The underlying disease is consistent with hypersensitivity pneumonitis and may be triggered by low concentrations of the diisocyanate.
- hypersensitivity
- immunologic haemorrhagic pneumonia
- isocyanates
- naphthylene-1,5-diisocyanate
- pneumonitis
Approximately two decades ago, trimellitic anhydride (TMA) pulmonary disease anaemia syndrome was described in workers occupationally exposed to TMA 1. TMA-induced pulmonary haemosiderosis is the most firmly established occupationally-related diffuse pulmonary haemorrhage syndrome, which has been reported in both humans and experimental animals 2. An immunological basis for the disease was assumed because immunoglobulin (Ig)-A, IgE and IgG antibodies to trimellityl proteins were detected in human 3, and a correlation between haemorrhagic lung foci and serum antibodies to radiolabelled TMA rat serum albumin was demonstrated in rats after inhalation of TMA 4. To the best of the authors' knowledge, only one case report has been published describing “immunological haemorrhagic pneumonia” in a spray painter with probable high exposure to isocyanates (a polyurethane enamel with aliphatic polyisocyanate and hexamethylene diisocyanate (HDI)) 5. The causal link between exposure to isocyanates and the disease was established by the demonstration of IgE and IgG antibodies to HDI and toluene diisocyanate (TDI) in the patient's serum. Here, the authors report another case of haemoptysis due to isocyanate exposure.
Case report
History
A never-smoking 24-yr-old male developed work-related runny nose, severe cough, malaise, flu-like symptoms (the latter mostly in the afternoon and evening) and shortness of breath on exertion. These symptoms first appeared in July 1998, a few days after the production of polyurethane foam parts for various industries by an injection moulding operation using diphenylmethane-4,4′-diisocyanate (MDI) and naphthylene-1,5-diisocyanate (NDI). Symptoms improved markedly during weekends. Spirometry performed a few weeks prior to isocyanate exposure was normal, but 3 weeks after the beginning of isocyanate exposure the vital capacity was 79% of predicted, and “pathological lung sounds” were documented by the factory physician. After 7 weeks of exposure, the subject had lost 10 kg of body weight. On a Friday evening, he experienced massive haemoptysis and was admitted to a local hospital. Radiography showed diffuse patchy infiltrates in both lungs. Mechanical ventilation was initiated due to profound hypoxaemia. Haemoptysis resolved spontaneously but reappeared after 3 days. Although a diffuse lung disease was suspected, on bronchoscopy bleeding was limited to the middle lobe, and lobectomy was performed on the same day. The remainder of the clinical course was uneventful; the patient became symptom-free without medication (systemic high dose steroids had been given initially). Serological tests did not indicate any connective tissue disease. Bronchoalveolar lavage (BAL) performed 3 weeks later showed 42% lymphocytes with a CD4/CD8 ratio of 0.05.
Clinical and immunological evaluation
The patient was examined at the Research Institute for Occupational Medicine (Bochum, Germany) for the purposes of an expert medical opinion ∼1-yr later in October 1999. He had developed an insulin-dependent diabetes mellitus in December 1998. At the time of examination, he had not returned to work and was free of symptoms. Auscultation of the lungs was normal. Both total lung capacity and forced expiratory volume in one second, were 92% pred 6. Single- breath carbon monoxide diffusing capacity as well as arterial blood gases at rest and after 6 min of treadmill exercise with 125 watts were normal. There was no bronchial hyperresponsiveness 7. Blood glucose was elevated. The patient was not anaemic and there were no signs of an inflammatory disease. Total IgE was 7 kU·L−1 and skin-prick tests with environmental allergens were completely negative. No specific IgE or IgG antibodies to human serum albumin conjugates of HDI, MDI, TDI and NDI (Desmodur 15, Bayer, Leverkusen, Germany) or a panel of acid anhydrides including phthalic and trimellitic anhydride were found in the patient's serum 8. Radiography of the chest did not show interstitial lung disease. The patient gave informed consent for exposure tests which were considered necessary to establish a causal relationship between the disease and the former workplace for medico-legal purposes. The concentrations of the MDI and NDI vapour in the test chamber were measured continuously with a calibrated tape monitor system (Continuous Toxic Gas Monitor Series 7100, MDA Scientific Inc., Lincolnshire, USA). Exposure to MDI (3 ppb for 10 min, 5 ppb for 110 min) in a chamber resulted in a fall of oxygen tension in arterial blood (Pa,O2) from 81 to 73 mmHg at both 2 and 4 h after exposure termination without any other pathological signs or symptoms. On the following day a challenge with NDI (5 ppb for 10 min, 10 ppb for 110 min) was performed (fig. 1⇓). The patient reported itching of the throat, headache, runny nose, burning lips and chills, which started about 2 h after leaving the chamber, and peaked in the night. A rise in body temperature from 36.3 to 38.6°C was documented 12 h afterwards. Vital capacity fell from 3720 (70%) to 3210 mL (60%) and Pa,O2 from 81 to 71 mmHg after 4 h, and to 65 mmHg after 24 h. On the next day, auscultation revealed rales in both lung bases. Fibreoptic bronchoscopy was performed 24 h after the second (NDI) challenge. Diffuse redness of the trachea and both mainstem bronchi was seen. The percent recovery of bronchoalveolar lavage fluid (BALF) was 88% with a total cell count of 1.8×107 and 61% neutrophils, 30% macrophages, 5% eosinophils and 4% lymphocytes. A total 73% of the lymphocytes were CD3+ cells (T-cells), 13% natural killer cells and the CD4/CD8 ratio was 0.23. Intracellular cytokine staining 9 of BALF CD3+ cells yielded 34% (85%) interferon-γ+, 16% (18%) interleukin (IL)-2+, 4% (1%) IL-4+ and about 1% IL-5+ (not done) and IL-13+ cells (1%) (numbers in parentheses represent the respective percentages of CD3+ BAL cells of a patient with known hypersensitivity pneumonitis).
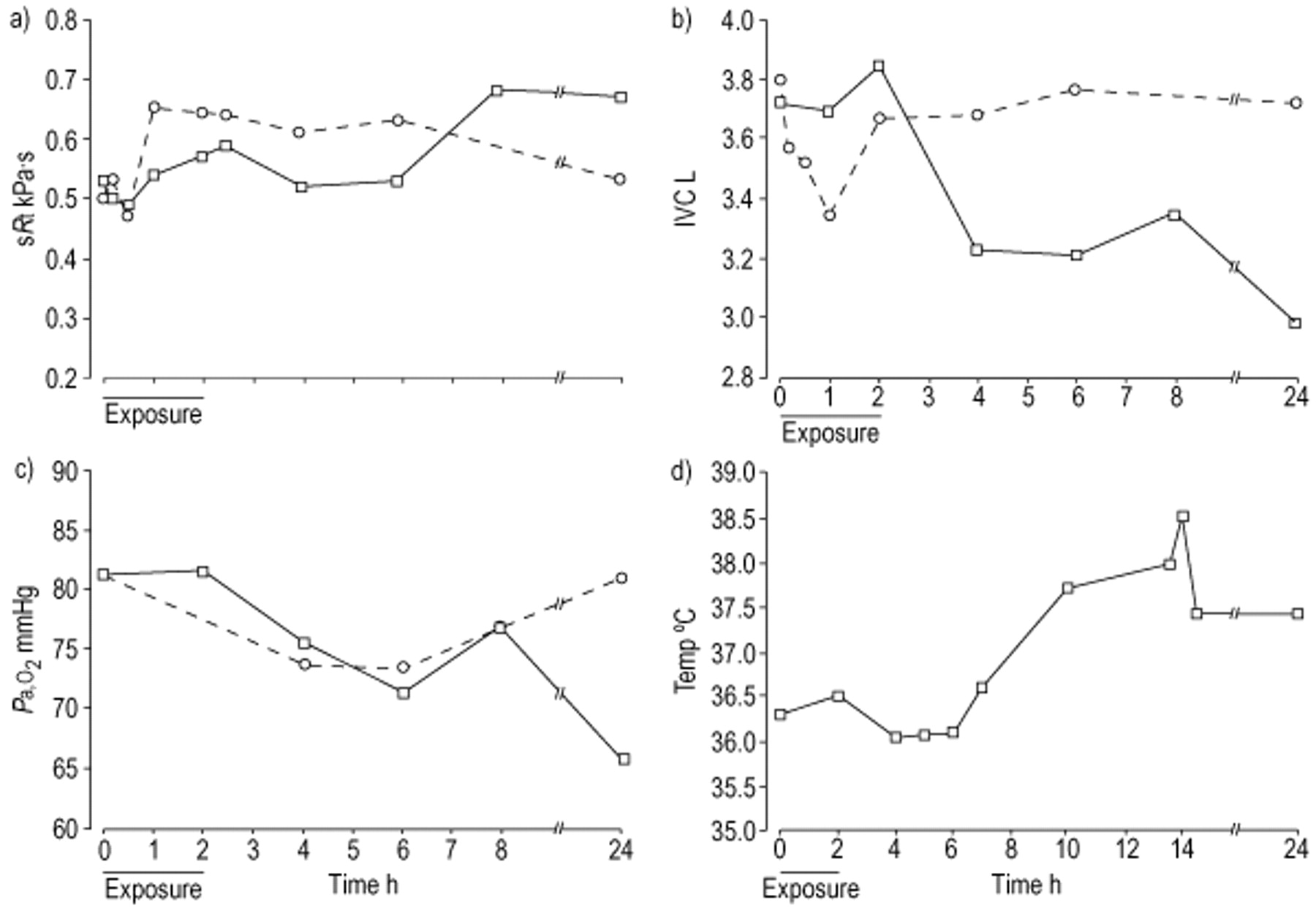
Results of the chamber challenge with naphthylene-1,5-di-isocyanate (NDI) (solid lines) and diphenylmethane-4,4′-di-isocyanate (MDI) (dotted lines). a) Specific airway resistance (sRt); b) inspiratory vital capacity (IVC); c) partial pressure of oxygen in arterial blood (Pa,O2); and d) body temperature (Temp) were measured.
The patient was discharged on a 1-week course of 25 mg oral prednisolone·day−1. The patient was contacted by telephone 1-month later and reported gradual but complete cessation of the symptoms which had occurred as a consequence of the chamber exposures.
Evaluation of the patient's workplace exposure
The patient handled isocyanates in 20-kg portions about 10–12 day−1. After heating to about 80–100°C, the isocyanates (about 95% was NDI), were filled manually in an open container and transported to the injection machine. The isocyanates were poured into the machine manually and the moulding process was automated. Personal protective equipment including protective clothing and gloves was available, but was not used by the worker. The work area contained stationary ventilation devices. Area sampling measurements of the patient's workplace obtained by the plant's technical service revealed NDI concentrations of 2.2 and 1.6 ppb in 1995, and 1.2 and 0.7 ppb in 1998 (the German threshold limit value of NDI is 10 ppb). MDI was measured below the detection limit of 0.02 ppb in 1998 (threshold limit 5 ppb). The patient reported that the ventilation system had broken down twice for several hours, which was followed by an increase in his symptoms.
Histological examination
The middle lobe, which had been resected 1-yr previously, was re-examined. The predominant finding was a diffuse alveolar haemorrhage mainly in the smaller bronchi with a variable amount of alveolar macrophages and leukocytes (fig. 2⇓). There was patchy to diffuse massive interstitial infiltration by small CD3 positive lymphocytes (fig. 3⇓), only a few plasma cells and a varying number of neutrophils were present, depending on the amount of alveolar damage and necrosis. CD20 positive B-cells were found focally in bronchial walls (data not shown). In smaller and middle-sized bronchi and bronchioli, focal and segmental ulcerations with granulation and focal bronchiolitis obliterans were seen (fig. 2⇓). Immunohistochemical staining showed IgG and to a lesser extent C1q in capillaries and alveolar membranes (fig. 3⇓). Staining for IgA, IgE and IgM was negative. Intra-alveolar macrophages contained mainly C1. Giant cells, histiocytic granulomas, foreign bodies or crystalline materials, fibrosis, microthrombi, vasculitis or immune complexes in larger vessels, or haemosiderin deposits were not found.
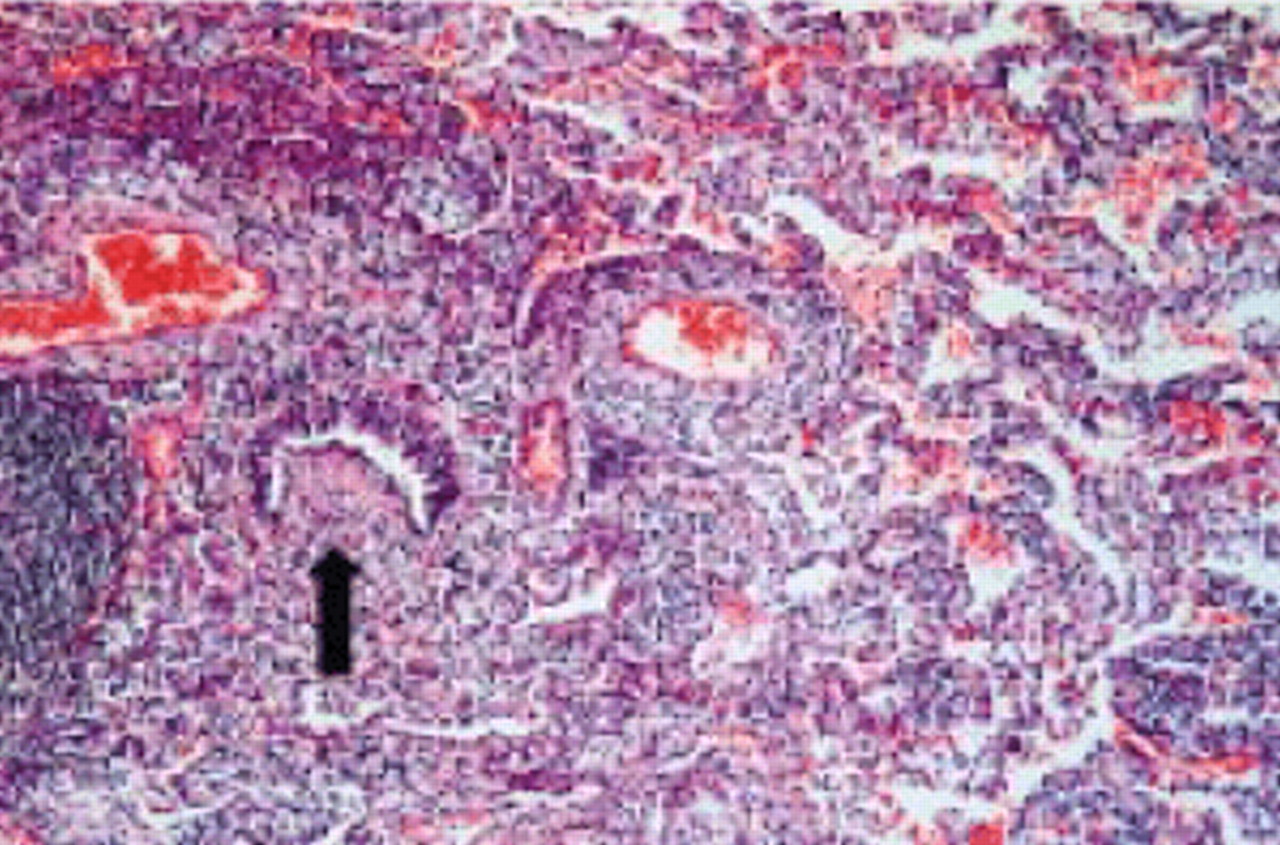
Dense interstitial infiltrate by CD3 positive T-lymphocytes and small bronchiole with bronchioiitis obliterans (arrow).

{kind=link}
{kind=link}
{kind=link}
Immunohistochemical staining demonstrates distinct membranous deposits of immunoglobulin (Ig)-G and C1q in areas of alveolar haemorrhage, indicating immune complex induced alveolitis. IgA, IgE and IgM are found in plasma cells only.
Discussion
NDI is a highly reactive aromatic diisocyanate which is used mainly in the automotive industry for the production of high-quality elastomers, resins and synthetic rubber. At room temperature the substance is solid and of a pale yellow colour. Asthma due to NDI has been described by several authors 10.
The patient gave a history compatible with occupational hypersensitivity pneumonitis due to isocyanates. Although the present immunological evaluation after 1-yr without any exposure to isocyanates did not reveal isocyanate-specific IgE or IgG antibodies, the diagnosis of early hypersensitivity pneumonitis due to NDI is supported by the symptoms, the histological and immunohistochemical findings as well as the present challenge test. Also neutrophilia in BALF, as seen in this patient, is compatible with an acute form of hypersensitivity pneumonitis 12. The subject mainly used NDI at his workplace. The fall of Pa,O2 after challenge with MDI is difficult to interpret, but might indicate cross-reactivity between both diisocyanates.
The schedule of the challenge tests with diisocyanates differs from reported schedules in the literature 13, which are performed on at least 3 days (1 day at the Research Institute for Occupational Medicine, Bochum, Germany). The challenge performed in this subject proved safe in a high number of asthmatic subjects and also in a small number of subjects with hypersensitivity pneumonitis due to diisocyanates 7. Nonetheless a 10-min step with diisocyanate concentrations only slightly above the detection limit of the monitoring device was used.
To the best of the authors' knowledge, this is the first case of hypersensitivity pneumonitis and haemorrhage due to NDI reported in the literature. In a similar case report of haemorrhage after occupational inhalation of diisocyanates the authors proposed the term “immunological haemorrhagic pneumonia” 5. In that case, a 34-yr-old MDI spray painter developed haemoptysis, pulmonary radiographical infiltrates, and hypoxaemia rapidly progressing to ventilatory failure. Open lung biopsy revealed intra-alveolar haemorrhage and haemosiderin-laden macrophages. Although antibodies to isocyanate-human serum albumin could be detected in the worker's serum, pulmonary haemorrhage due to diffuse alveolar damage cannot be ruled out as little information about exposure to isocyanates was provided. Reports about TMA-induced haemorrhage have universally been associated with spraying operations, typically with metal baking processes where fume exposure was heavy. The present case suggests rather an acute hypersensitivity pneumonitis with haemorrhage probably due to immune complex mediated necrotizing alveolitis (and bronchiolitis). Interestingly, symptoms were reproduced by low isocyanate concentrations during challenge. Exposure to isocyanates in the patient's workplace was reportedly low. However, intermittent higher isocyanate exposure cannot be excluded. This argues for an immunological disease and does not support the view of haemorrhage due to diffuse alveolar damage, although there may be a spectrum of responses that includes pulmonary haemorrhage as a pathological component rather than a clear and absolute demarcation between “diffuse alveolar injury with haemorrhage” and “diffuse pulmonary haemorrhage” 14.
Although the precise mechanism of bleeding remains unclear, the present case clearly shows that isocyanates may trigger hypersensitivity reactions in susceptible subjects at very low concentrations in the range of the present threshold limit value and that this may result in life-threatening pulmonary haemorrhage within a few weeks of exposure to these chemicals. It is not known whether higher exposure levels than those of the present challenge are necessary to induce haemorrhage.
Acknowledgments
The authors acknowledge the support of G. Wittstock, Institute of Pathology and M. Kunze, Berufsgenossenschaft der Chemischen Industrie, Hamburg, Germany as well as L. Brown, Baltimore, USA for translating the manuscript.
- Received May 11, 2001.
- Accepted August 2, 2001.
- © ERS Journals Ltd
References









