





Abstract
Sarcoidosis and usual interstitial pneumoniae (UIP) are diseases of unknown aetiology affecting the lower respiratory tract. Although there are a number of studies investigating the causal role of these disorders, no micro-organism could be identified as the causal agent. The high incidence of Chlamydophila pneumoniae infections associated with lung injury encouraged the present investigations to screen patients with sarcoidosis and with UIP for their Chlamydophila-specific immune response.
Thirty-nine patients with sarcoidosis, 26 patients with UIP and 34 controls were tested for the prevalence of Chlamydophila-specific antibodies in bronchoalveolar lavage fluids (BALF) and sera. Samples were tested for the presence of antibodies in a genus-specific test for Chlamydophila-lipopolysaccharide (LPS) and in a species-specific test for C. pneumoniae.
This study revealed a significantly higher prevalence of Chlamydophila LPS-specific immunoglobulin (Ig)-G in the BALF of sarcoidosis patients (36.8%) compared to controls (8.8%) and patients with UIP (12.0%). Similar findings were observed in sera. The prevalence of C. pneumoniae-specific antibodies in BALF was significantly higher in sarcoidosis patients for IgG and IgA (IgG: 74.4%; IgA: 46.2%) and in UIP for IgG (IgG: 50.0%; IgA: 11.5%) compared to controls (IgG: 14.7%; IgA: 14.7%).
The elevated prevalence of Chlamydophila-specific antibodies in sarcoidosis patients might implicate Chlamydophila as a causal agent. However, considering the high prevalence of Chlamydophila antibodies in the healthy population, the data presented might reflect Chlamydophila co-infections in pre-injured lungs seen in these patients.
Sarcoidosis is a systemic, granulomatous disease of unknown aetiology affecting mainly the respiratory tract and the hilar lymph nodes 1. Many agents have been implicated as granuloma-inducing factors. Numerous studies have been published investigating the possible role of infective agents such as mycobacteria 2, 3, Borrelia burgdorferi 4, Corynebacteria 3, 5 or herpesviruses 6. Another candidate highly associated with chronic respiratory disorders is Chlamydophila pneumoniae 7. The first report of an association between a Chlamydophila-specific antibody response and sarcoidosis is dated to 1976 8 and was followed by other studies discussing a link between C. pneumoniae-specific antibody titres and sarcoidosis 7. In spite of these findings, efforts to demonstrate the presence of C. pneumoniae deoxyribonucleic acid (DNA) in lung biopsies of 24 sarcoidosis patients failed 9. Nevertheless, infection with C. pneumoniae may trigger a self-maintaining immune response that could persist even after elimination of the pathogen from the affected tissue.
Another group of interstitial lung diseases of unknown aetiology are called cryptogenic fibrosing alveolitis or idiopathic pulmonary fibrosis. Recently, this group of interstitial lung diseases was subdivided in unique clinicopathological subgroups with distinctly different natural histories 10. Usual interstitial pneumoniae (UIP), characterized by an increase of inflammatory cells in, and fibrosis of the alveolar epithelium and the lung interstitium, is the member of this group which most frequently leads to death occurring within 3–6 yrs after diagnosis 11. Several studies demonstrated the central role of alveolar macrophages in UIP 12, 13. An interesting finding, in the context of the present study, is the ability of alveolar macrophages from patients with cryptogenic fibrosing alveolitis to phagocytose intracellular bacteria, and yet they fail to kill the pathogens 14. This could support persistence of the infectious agents, resulting in chronic infection. Moreover, the increased cytokine production by alveolar macrophages seen in this type of disorder may indicate a response to an unknown stimulus, for example a pathogen 15.
To address the question whether Chlamydophila is involved in the pathogenesis of the named disorders, the presence of immunoglobulin (Ig)-G and IgA antibodies was measured in bronchoalveolar lavage fluid (BALF) and sera directed against genus-specific Chlamydophila lipopolysaccharide (LPS). To obtain information on the Chlamydophila species, a newly-developed serological assay to measure species-specific antibodies against C. pneumoniae-specific proteins was used.
Material and methods
Study population
The diagnosis of nonacute sarcoidosis was established in 39 patients in accordance with previously defined criteria 16, including noncaseating granulomata identified by transbronchial biopsies. The diagnosis of UIP was established in 26 patients based on typical clinical, radiographical and histopathological findings. In high-resolution tomography of the thorax, intralobular interstitial opacities, irregular interlobular septal thickening, and honeycombing of the lower zones were required 17. In histopathological specimens of transbronchial biopsies, a patchy distribution with alternating zones of interstitial fibrosis, inflammation, honeycomb, and normal lung served as diagnostic pattern 10. In view of unequivocal histopathological findings, active exclusion of other differential diagnoses, and the fact that none of the patients were younger than 50 yrs of age, open lung biopsies or video-assisted thoracoscopic biopsies were not performed to obtain tissue specimens, which is an accepted diagnostic strategy 17. Clinically an insidious onset, a chronic progressive course with loss of lung volumes and reduction of diffusion capacity, were prerequisites for diagnosis 17. All stains and cultures for fungi or bacteria, including mycobacteria, were negative both in bronchoalveolar lavage (BAL) and tissue specimens. All specimens used in this study were taken at the time point of making the diagnosis and none of the patients were undergoing therapy. Thirty-four patients who underwent bronchoscopy due to chronic cough and were retrospectively free of inflammatory or malignant disorders served as controls. Characteristics of the study populations are described in table 1⇓. All patients gave their informed consent for BAL.
Characterization of the study populations
Bronchoalveolar lavage and cytology
BAL was performed as previously described 18. Briefly, 200–300 mL of sterile saline (0.9% NaCl) was instilled in 25-mL aliquots into a lingula or middle lobe segment. Each aliquot was immediately aspirated. Mean recovery was 62.4% and the average cell number·100 mL−1 of BAL cells was 18.5±2.1×106. The cells were centrifuged at 500×g and washed three times with phosphate buffered saline (PBS) at 4°C. Cell differentials were determined by counting ≥200 cells on a cytocentrifuge preparation (Cytospin II, Shandon Instruments, Sewickley, PA, USA). Cells were stained with Haemacolor (Merck, Darmstadt, Germany). Results of differential counting of BAL cells are depicted in table 1⇑.
Detection of Chlamydophila lipopolysaccharide antibodies in bronchoalveolar lavage fluid and serum
For the genus-specific recombinant enzyme-linked immunosorbent assay (rELISA), an artificial glycoconjugate containing the deacylated carbohydrate backbone of a recombinant Chlamydophila-specific LPS 19, 20 was used as a solid-phase antigen. The rELISA was used to measure IgG and IgA antibodies against Chlamydophila LPS in BALFs and sera, and IgM antibodies in sera. The assay was performed as described earlier 20 with the following modifications: to block unspecific binding, PBS was supplemented with 0.05% Tween-20 and 2.5% casein. Sera, BALFs and secondary antibodies were diluted in PBS supplemented with 0.05% Tween-20, 2.5% casein and 5% bovine serum albumin (BSA). For IgG and IgA sera, samples were considered positive when the optical density (OD) was 10% above the cut-off level of 0.32, and for IgM OD was 15% above the cut-off of 0.37. Positive sera were titrated. A BALF was defined as positive at an OD>0.5 for IgA and IgG in 1:2 dilution.
Detection of Chlamydophila pneumoniae protein antibodies in bronchoalveolar lavage fluid and serum
C. pneumoniae species-specific IgG and IgA antibodies in sera and BALFs were measured by enzyme immunoassay (EIA). Purified and formaline-treated (0.02%) C. pneumoniae (strain TW-183) elementary bodies (EB) were used as antigen (2 µg·well−1 in 50 mM carbonate buffer (pH 9.2)) to coat EIA plates (Maxisorp, Nunc, Wiesbaden, Germany) for 48 h at 4°C. If not stated elsewhere, 50 µL volumes were used. Excess antigen was removed by two washing steps with PBS (200 µL·well−1), followed by blocking with PBS supplemented with 2.5% casein for 1 h at 37°C. After washing with PBS, the plates were dried for 1 h at room temperature and subsequently for 1 h at 37°C. Prior to testing, samples were absorbed with recombinant Chlamydophila-specific LPS complexed with BSA 21. Sera were diluted in PBS supplemented with 2.5% casein and 5% BSA (PBS-C-BSA), 1:200 for IgG and 1:100 for IgA, and BALF 1:2 for IgG and IgA. Aliquots (100 µL) of each prediluted sample were absorbed with 10 µL (1 mg·mL−1) of LPS-BSA-complex for 1 h at 37°C in a water bath, interrupted by careful shaking after 30 min followed by a centrifugation step (1 h, 15,000×g, 4°C). The absorbed samples were added to the coated plates, serially diluted in PBS-C-BSA and incubated for 1 h at 37°C. After two washing steps with PBS, samples were incubated (1 h at 37°C) with peroxidase conjugated goat antihuman IgG and IgA (1:1,000 and 1:1,200, respectively in PBS-C-BSA; Fc portion of the g heavy chain (Fcγ)- and α-chain-specific respectively; Dianova, Hamburg, Germany). After another three washing steps in PBS, the plates were washed once in substrate buffer (0.1 M sodium citrate, pH 4.5). Substrate solution was freshly prepared and was composed of azino-di-3-ethylbenz-thiazolin sulfonic acid (1 mg; Sigma, Munich, Germany) dissolved in 1 mL substrate buffer followed by the addition of hydrogen peroxide (25 µL 0.1% H2O2). After 30 min at 37°C, the reaction was stopped by the addition of 2% aqueous oxalic acid. The OD was measured by a microplate reader (Dynatech MR 5000, Dynex Technologies, Inc., Chantilly, VA, USA) at 405 nm. End-point titres of sera were defined as the final dilution yielding OD405>0.5. A serum sample was defined as positive at an OD>0.6 for IgA and IgG and for BALFs was defined as an OD>0.5 for IgA and IgG.
Tumour necrosis factor-α assay
Tumour necrosis factor (TNF)-α was determined by an ELISA as described 22. The monoclonal antibody directed against recombinant human TNF-α (rhTNF-α), clone 195 and rhTNF-α were a gift of Fa. Knoll, Ludwigshafen, Germany. For the TNF-α assay, healthy individuals (n=25) described in 22 served as controls.
Statistical analysis
Comparisons were performed using Mann-Whitney U-test and Chi-squared test. The correlations between different parameters were analysed using Spearman's rank correlation coefficient (rs). p-Values <0.05 were considered as significant.
Results
Clinical features
The 99 individuals in this study were divided into three groups according to their diagnosis: sarcoidosis (n=39), UIP (n=26) and controls (n=34). The three groups did not differ significantly in sex and smoking history (table 1⇑). The mean age of the UIP patients was significantly higher than that of the control group and the sarcoidosis group (p<0.0001). Sarcoidosis and UIP patients presented with decreased lung function parameters (table 1⇑).
Bronchoalveolar lavage, immunological and serological parameters
As shown in table 1⇑, the percentage of alveolar macrophages (p<0.0001), BAL lymphocytes (p<0.0001), neutrophils (p<0.01) and eosinophils (p<0.05) was significantly higher in the sarcoidosis group than in the control group, a significant elevation could also be noted for the CD4/CD8 ratio (p<0.05). For the UIP group, similar trends could be observed except for BAL lymphocytes and the CD4/CD8 ratio, which were comparable to the control group (alveolar macrophages: p<0.05; neutrophils: p<0.0001; eosinophils: p<0.001). The observed changes in different cell counts are typical for the analysed disorders. As shown in table 1⇑, the mean spontaneous release of TNF-α by cultured BAL cells of the sarcoidosis group (p<0.0001) and of the UIP group (p<0.01) differed significantly from that of controls. There was no significant correlation between the TNF-α release of BAL cells and the Chlamydophila-specific immune response analysed in this study. In all groups, peripheral blood leukocyte counts were within the normal range, although in UIP a significant elevation was observed.
Prevalence of Chlamydophila-specific immunoglobulin-G and immunoglobulin-A in bronchoalveolar lavage fluid and immunoglobulin-G, immunoglobulin-A and immunoglobulin-M in serum
Analysing the Chlamydophila genus-specific LPS-IgG antibodies in BALF revealed a significantly higher mean OD of 545.6±131.2 (36.8% positive samples) for the sarcoidosis group compared to 151.5±44.7 (8.8%) in the control group (p<0.01). The mean OD obtained for the UIP group (250.5±97.8; 12.0%) did not differ significantly from the controls (fig. 1a⇓). These data could be confirmed by measuring the anti-LPS IgG antibodies in serum: the mean OD of 1120.4±152.8 (74.4% positive sera) for the sarcoidosis group was significantly higher than that of the control group with 701.2±132.3 (47.1%; p<0.05) and the UIP group with 811.1±152.9 (57.7%; fig. 1a⇓). The anti-LPS IgG concentration in serum of UIP patients showed a positive correlation with age (p<0.01; Rho=0.529). The analysis of the IgA response in BALF with 452.5±119.4 (26.3%) as well as in serum with 724.7±138.1 (53.8%) revealed no significant difference for the sarcoidosis group compared to the control group (BALF: 230.4±61.0 (26.5%); serum: 370.6±79.5 (35.3%)). For the UIP group, a significant elevation of the mean OD of IgA in serum (652.2±138.4 (42.3%); p<0.05) was noted, which did not parallel in BALF (174.1±40.8 (12.0%) fig. 1b⇓). Determination of IgM in sera revealed comparable levels for all groups tested without significant differences (sarcoidosis: 186.8±54.5 (7.7%); UIP 146.9±35.2 (15.3%); controls: 222.0±64.4 (11.8%)).
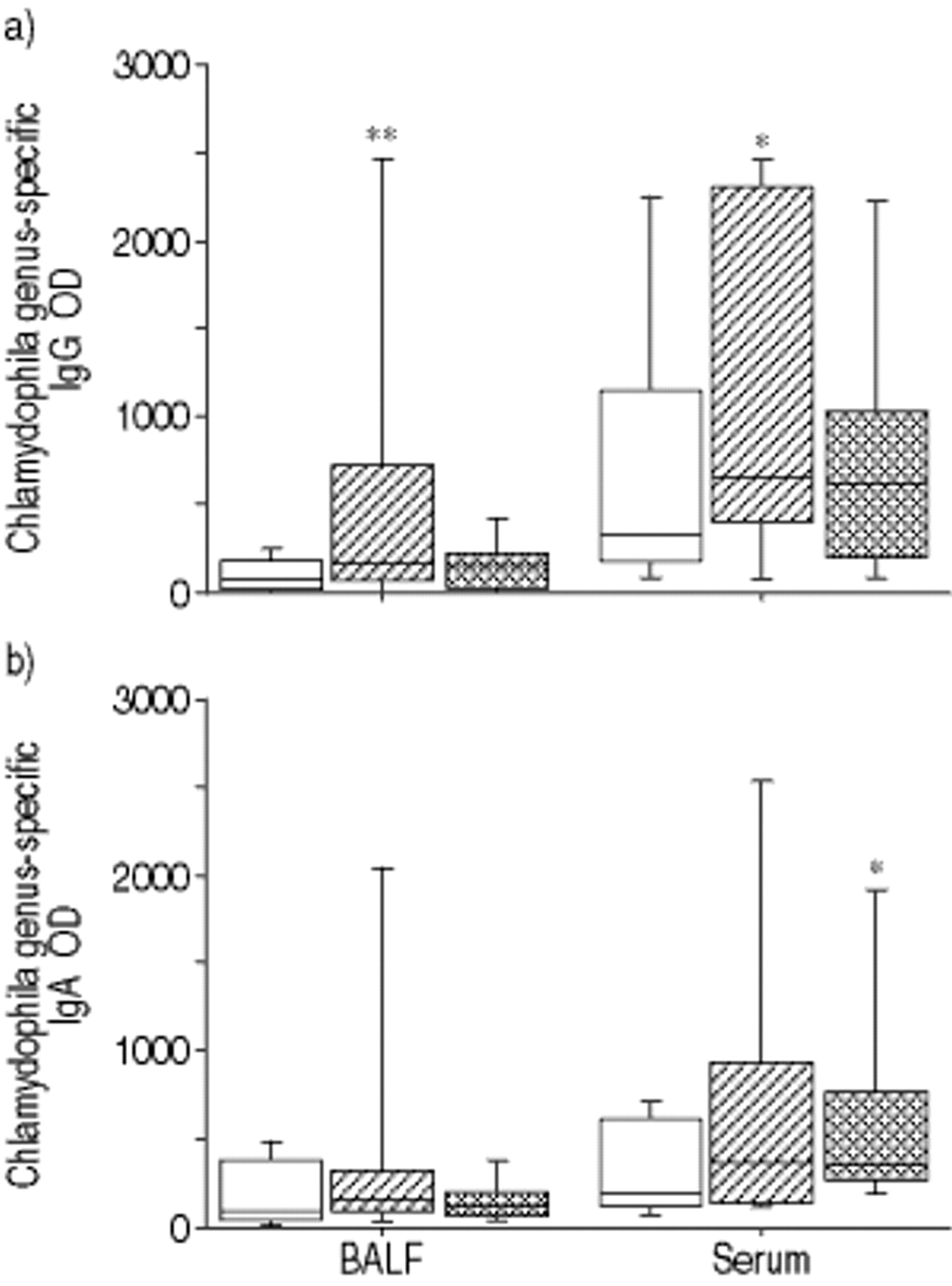
Prevalence of Chlamydophila genus-specific immunoglobulin (Ig)-G and IgA in bronchoalveolar lavage fluid (BALF) and in serum detected by recombinant enzyme-linked immunosorbent assay. a) IgG and b) IgA concentrations in BALF and serum of controls (C, □), usual interstitial pneumoniae patients (UIP,  ), and sarcoidosis patients (S, └,)). OD: optical density. Diagnosis (positive/n, %) in a) IgG in BALF: C (3/34, 8.8), S (14/38, 36.8; p<0.05), UIP (3/25, 12.0); IgG in serum: C (16/34, 47.1), S (29/39, 74.4; p<0.05), UIP (15/26, 57.7); and in b) IgA in BALF: C (9/34, 26.5), S (10/38, 26.3; p<0.05), UIP (3/25, 12.0); IgA in serum: C (12/34, 35.3), S (21/39, 53.8), UIP (11/26, 42.3). *: p<0.05; **: p<0.01.
), and sarcoidosis patients (S, └,)). OD: optical density. Diagnosis (positive/n, %) in a) IgG in BALF: C (3/34, 8.8), S (14/38, 36.8; p<0.05), UIP (3/25, 12.0); IgG in serum: C (16/34, 47.1), S (29/39, 74.4; p<0.05), UIP (15/26, 57.7); and in b) IgA in BALF: C (9/34, 26.5), S (10/38, 26.3; p<0.05), UIP (3/25, 12.0); IgA in serum: C (12/34, 35.3), S (21/39, 53.8), UIP (11/26, 42.3). *: p<0.05; **: p<0.01.
For more detailed information on the extent of positive results, titres of IgG, IgA and IgM in positive sera were determined in all groups. More sarcoidosis patients (6/39; 15.4%) showed IgG titres >1:3,200 in serum, compared to the control group (2/34; 5.8%) or the UIP group (1/26; 3.8%). A similar situation could be noted for the IgA Chlamydophila genus-specific LPS response: 6/39 (15.4%) sarcoidosis patients presented with IgA titres >1:800 in serum, compared to 0/34 (0.0%) controls or 0/26 (0.0%) in the UIP patients. Data are shown in table 2⇓.
Chlamydophlia-specific antibody titres in positive serum samples
Prevalence of Chlamydophila pneumoniae-specific immunoglobulin-G and immunoglobulin-A in bronchoalveolar lavage fluid and immunoglobulin-G and immunoglobulin-A in serum
To obtain more detailed information on the causative Chlamydophila species, the same samples were additionally tested in the species-specific EB-EIA, which detects only antibodies specific for C. pneumoniae and not for other Chlamydophila species. After LPS absorption, the samples were included in the EB-EIA described above using purified EBs as antigen. The mean OD level of C. pneumoniae-specific IgG in the BALF of the sarcoidosis group (1350.0±140.1 (74.4%)) was significantly elevated (p<0.0001) compared to the control group (335.8±79.0 (14.7%)). The mean OD determined for anti-C. pneumoniae IgG in the UIP group was 720.4±145.8 (50.0%) and also showed a significant elevation (p<0.01). Detection of C. pneumoniae-specific IgG antibodies in serum revealed very high concentrations for all samples tested with only slight differences between the three groups (sarcoidosis: 2231.1±102.9 (92.3%); UIP: 2167.2±116.0 (96.2%); controls: 1922.9±156.1 (82.4%)). However, in the sarcoidosis group, 79.5% showed an OD of >2,500 (fig. 2a⇓).

{kind=link}
{kind=link}
Prevalence of Chlamydophila pneumoniae (C. pneumoniae) species-specific immunoglobulin (Ig)-G and IgA in bronchoalveolar lavage fluid (BALF) and in serum detected by elementary body enzyme immunoassay. a) IgG and b) IgA concentrations in BALF and serum of controls (C, □), usual interstitial pneumoniae patients (UIP,  ) and sarcoidosis patients (S, └). OD: optical density. Diagnosis (positive/n, %) in a) IgG in BALF: C (5/34, 14.7), S (29/39; 74.4; p<0.001), UIP (13/26, 50; p<0.01); IgG in serum: C (28/34, 82.4), S (36/39, 92.3), UIP (25/26, 96.2); and in b) IgA in BALF: C (5/34, 14.7), S (18/39, 46.2; p<0.05), UIP (3/26, 11.5); IgA in serum: C (23/34, 67.6), S (25/39, 64.1), UIP (23/26, 88.5). *: p<0.05; ***: p<0.001; #: p<0.0001.
) and sarcoidosis patients (S, └). OD: optical density. Diagnosis (positive/n, %) in a) IgG in BALF: C (5/34, 14.7), S (29/39; 74.4; p<0.001), UIP (13/26, 50; p<0.01); IgG in serum: C (28/34, 82.4), S (36/39, 92.3), UIP (25/26, 96.2); and in b) IgA in BALF: C (5/34, 14.7), S (18/39, 46.2; p<0.05), UIP (3/26, 11.5); IgA in serum: C (23/34, 67.6), S (25/39, 64.1), UIP (23/26, 88.5). *: p<0.05; ***: p<0.001; #: p<0.0001.
For the species-specific IgA response, a similar situation could be noted. BALFs of sarcoidosis patients showed a significant increase (693.4±111.8 (46.2%); p<0.0001) compared to those of controls (263.8±81.5 (14.7%)). As for IgG in BALF, the UIP patients showed no significant difference for IgA (209.3±58.2 (11.5%)). Although on a very high level, the IgA titre in serum produced no significant differences between the groups tested (sarcoidosis: 1502.4±125.0 (64.1%); UIP: 1611.8±148.6 (88.5%); controls: 1274.2±154.6 (67.6%). It can be noted that the results obtained for the genus-specific response, concerning the titres of the positive sera, were confirmed in the species-specific IgG and IgA response: 16/39 (41.0%) sarcoidosis patients showed C. pneumoniae-specific IgG titres >6,400 in serum, compared to 5/34 (14.7%) in the control group or 7/26 (27.0%) in the UIP group. Also for the IgA titres, the highest percentage (8/39 (20.5%)) positive sera>1,600) was observed in the sarcoidosis group; however, lower percentages were determined for UIP patients (2/26 (7.7%)) or controls (4/34 (11.8%)). Data are shown in figure 2⇑ and table 2⇑.
Discussion
The study populations exhibited typical clinical, radiographical, and histopathological characteristics of sarcoidosis and UIP, two interstitial lung diseases of unknown origin for which infective triggers or even infectious aetiologies are discussed. The most interesting findings of the present study are the significantly elevated C. pneumoniae species-specific IgG and IgA concentrations in the BALF of sarcoidosis patients compared to control subjects. To the best of the authors' knowledge, this is the first report analysing Chlamydophila antibodies in BALF of patients with sarcoidosis or UIP. Furthermore, the study presents the parallel analysis of sera and BALFs that were tested in two different test systems: The rELISA detecting Chlamydophila LPS antibodies and the EB-EIA identifying C. pneumoniae-specific protein antibodies. Moreover, this study supplies the comparative analysis of two interstitial lung diseases with unknown aetiology.
A newly-developed serological assay to measure species-specific antibodies against C. pneumoniae proteins named EB-EIA was used in this study. Pre-incubation of samples with an absorbent containing the genus-specific carbohydrate epitope of Chlamydophila eliminated the cross-reactive LPS antibodies without affecting the reactivity of the remaining antibodies against species-specific protein. The assay is also sensitive enough to be used for the measurement of IgG and IgA antibodies in BALF. Additionally, the samples were tested for the presence of antibodies against genus-specific Chlamydophila LPS 21, 23. The microfluorescence assay (MIF) is regarded as the gold standard for Chlamydophila serology 24. However, it is reported that this test lacks standardization and produced high rates of disagreement for negative or “chronic” low IgG titres, often resulting in false positive serodiagnosis in an inter-laboratory study 25. Therefore, the newly developed EB-EIA, described in material and methods was used.
The search for a causative agent in sarcoidosis has so far failed to produce definitive results. C. pneumoniae is known to be a common respiratory pathogen 26, 27. Moreover, it has been shown that this intracellular bacterium may be involved in various chronic diseases 27, 28. Poulakkainen et al. 7 found an increased seroprevalence of anti-C. pneumoniae antibodies in sarcoidosis patients compared to controls. In spite of these reports, the efforts of Blasi et al. 9 to detect C. pneumoniae-specific DNA within sarcoid tissue failed. High antibody titres do not necessarily indicate a causal link to sarcoidosis. They could be a cumulative effect of the polyclonal B-cell activation observed in sarcoidosis and the high seroprevalence in the general population 29, 30. Alternatively, as proposed by Blasi et al. 9, C. pneumoniae may trigger a self-maintaining immune response, persisting even after elimination of the pathogen.
Chlamydophila LPS-specific IgM concentrations in serum, used as a marker for a primary or acute infection, showed no significant difference between either sarcoidosis or UIP patients compared to controls, which is in line with the chronic character of these interstitial lung diseases. Since IgG production generally starts later and lasts longer, the significantly-elevated titres of Chlamydophila LPS-specific as well as C. pneumoniae-specific IgG in the BALF of sarcoidosis patients could fit with chronic Chlamydophila infections in these patients. Since 80% of IgA in BALF is produced by the respiratory mucosa and its half-life is 5–6 days, the significantly higher concentrations of C. pneumoniae-specific IgA detected in BALFs of sarcoidosis patients compared to controls might indicate an acute or reinfection 31. For serum, it is generally accepted that high IgA levels are indicative for ongoing and chronic infections. Therefore, for diagnosis of chronic infections detectable IgG and IgA serum concentrations are needed. As depicted in figure 2⇑, sarcoidosis patients presented with significantly increased C. pneumoniae-specific IgG and IgA values in BALF, which is in line with hypothetical chronic infections or reinfections at the site of the lung in these patients.
Studies investigating C. pneumoniae seroprevalence by MIF, in the normal European population, report 20% positives in young adults to 80% in elderly males 32. Using rELISA to analyse the Chlamydophila LPS seroprevalence revealed 74.4% for the sarcoidosis group with an average age of 46 yrs, which is within the range of data published by Poulakkainen et al. 7. To a lesser extent, determination of anti-LPS-IgG in BALF confirmed the results obtained for serum; the prevalence in sarcoidosis patients was 36.8%, significantly higher than in control subjects (8.8%). Moreover, the prevalence for C. pneumoniae species-specific IgG in BALF was even more pronounced and significantly elevated to 74.4% compared to 14.7% in controls. For IgA, the seroprevalence of anti-LPS-antibodies was higher in sarcoidosis patients (52.6%) than in controls (35.3%), although the difference was not significant. Data obtained for IgA in BALF is of special value since it might indicate the potential site of infection in respiratory diseases. Of the total IgA measured in BALF, 85% is secretory IgA indicating that ∼80% of the measured BALF-IgA is produced in the lung 31. Therefore, the significantly-increased C. pneumoniae-specific BALF-IgA levels in 44.7% of sarcoidosis patients could be associated with chronic infections, although these data could not be confirmed by detection of Chlamydophila LPS-specific IgA in the same BALF. An association between the data obtained for sarcoidosis patients and the known hypergammaglobulinaemia 30 could be hypothesized. Moreover, a triggering function of Chlamydophila in sarcoid lungs seems possible, although the missing correlation between the significantly elevated TNF-α release of BAL cells and the prevalence of Chlamydophila-specific antibodies in BALF and serum is in conflict with a causal relationship of Chlamydophila in sarcoidosis. In summary, the data presented could not prove a causal role of Chlamydophila in sarcoidosis. The injured lung as a preferred habitat of C. pneumoniae might be a feasible alternative hypothesis to explain the elevated titres.
As mentioned previously, Chlamydophila infections are associated with multifactorial chronic diseases like asthma or arteriosclerosis 33, 34, but it is still not understood whether Chlamydophila infection is the cause of these disorders or if Chlamydophila is triggering the pathological changes. It is notable that C. pneumoniae can be phagocytosed by the alveolar macrophages of patients with cryptogenic fibrosing alveolitis (of which UIP is a subgroup); however, C. pneumoniae withstands killing, leading to chronic infection, which may trigger pathogenic mechanisms 14. Furthermore, several viral triggers for UIP or pulmonary fibrosis 35, as well as complicating infections with C. pneumoniae, have been observed that may promote specific pathomechanisms, which damage the microarchitecture of the lung 36, 37. However, there are no studies available that investigate a potential association between UIP and Chlamydophila infection.
The rELISA for detection of Chlamydophila genus-specific antibodies revealed an IgG seroprevalence of 57.7% and an IgA of 42.3% in UIP patients, which is significantly higher than the IgA prevalence in the control group or the published prevalence in the normal population 21. However, it has to be noted that the mean age of the UIP group in this study is significantly higher compared to the controls, which is a known hallmark of these patients 17. This could explain the elevated prevalence of IgA in these patients as demonstrated by the positive correlation of age and the anti-LPS IgG concentration in serum. With respect to the site of pathological changes in UIP, data obtained for BALF are of special interest. The Chlamydophila LPS-specific IgG and IgA prevalence of 12.0% and 12.5%, respectively, did not differ significantly from the control group.
In conclusion, the data presented in this study do not implicate any association between Chlamydophila infection and usual interstitial pneumoniae. On the basis of the presented data, the hypothesis of a causal involvement of Chlamydophila pneumoniae in usual interstitial pneumoniae should be rejected. The elevated Chlamydophila-specific antibodies in sera and bronchoalveolar lavage fluid of sarcoidosis patients seem to support a causal relationship between Chlamydophila pneumoniae and sarcoidosis. Moreover, the missing correlation between the elevated tumour necrosis factor-α release of bronchoalveolar lavage cells and the prevalence of Chlamydophila-specific antibodies in bronchoalveolar lavage fluid and serum is in conflict with a causal relationship of Chlamydophila in usual interstitial pneumoniae and sarcoidosis.
Acknowledgments
The authors would like to thank S. Cohrs for expert technical assistance.
- Received February 9, 2001.
- Accepted September 30, 2001.
- © ERS Journals Ltd
References









