



The role of positron emission tomography with 18F-fluoro-2-deoxy-D-glucose in respiratory oncology
- 1Respiratory Oncology Unit, Dept of Pulmonology and 2PET-Centre, Dept of Nuclear Medicine, University Hospital Gasthuisberg, Catholic University Leuven, Belgium
- J.F. Vansteenkiste, Respiratory Oncology Unit, Dept of Pulmonology, University Hospital Gasthuisberg, Herestraat 49, B-3000, Leuven, Belgium. Fax: 3216346803
Abstract
In the past 5 yrs, positron emission tomography (PET) with 18F-fluoro-2-deoxy-d-glucose (FDG) has become an important imaging modality in lung cancer patients. At this time, the indication of FDG-PET as a complimentary tool to computed tomography in the diagnosis and staging of non-small cell lung cancer has gradually gained more widespread acceptance and also reimbursement in many European countries.
This review focuses on the data of FDG-PET in the diagnosis of lung nodules and masses, and in locoregional and extrathoracic staging of non-small cell lung cancer. Emphasis is put on the potential clinical implementation of the currently available FDG-PET data. The use of FDG-PET in these indications now needs further validation in large-scale multicentre randomized studies, focusing mainly on treatment outcome parameters, survival and cost-efficacy.
Interesting findings with 18F-fluoro-2-deoxy-d-glucose-positron emission tomography have also been reported for the evaluation of response to radio- or chemotherapy, in radiotherapy planning, recurrence detection and assessment of prognosis. Finally, a whole new field of application of positron emission tomography in molecular biology, using new radiopharmaceuticals, is under extensive investigation.
- decision trees
- emission computed tomography
- 18F-fluoro-2-deoxy-d-glucose
- lung neoplasms
- non-small cell lung carcinoma
- predictive value of tests
This data was presented in part in the review-of-the-decade lecture at the 2000 Florence meeting of the European Respiratory Society
Lung cancer is the most common cause of cancer-related death in the Western world. Approximately three million new cases per year are estimated worldwide, of which more than 200,000 are in the European Union. An increase in incidence is to be expected until the first decades of the 21st century.
Imaging techniques such as chest radiography, computed tomography (CT), ultrasonography (US), and sometimes magnetic resonance imaging (MRI) are essential in the diagnosis, staging, and follow-up of patients with lung cancer. These imaging tests are based on differences in the structure of tissues, measured by differences in density (for CT), in surface reflectivity (for US), or in chemical environment (for MRI). Although current imaging technology allows exquisite anatomical detail, the density differences often don't allow a definitive diagnosis and staging, and more invasive tests with tissue sampling are required.
Positron emission tomography (PET) has been used over the last decades mainly as a research tool for brain function studies 1, 2 and for the assessment of cardiac metabolism. In the past 5 yrs, it has generated widespread enthusiasm as an innovative imaging technique in oncology, based on its ability to visualize differences in metabolism of tissues.
Lung tumour cells have a much higher rate of glycolysis in comparison with non-neoplastic cells, and an increased cellular uptake of glucose, probably due to an increased expression of glucose transporter proteins 3–6. FDG, a glucose analogue in which the oxygen molecule in position 2 is replaced by a positron-emitting 18fluorine, undergoes the same uptake as glucose, but is metabolically trapped and accumulated in the neoplastic cell after phosphorylation by hexokinase (fig. 1⇓) 7–9.
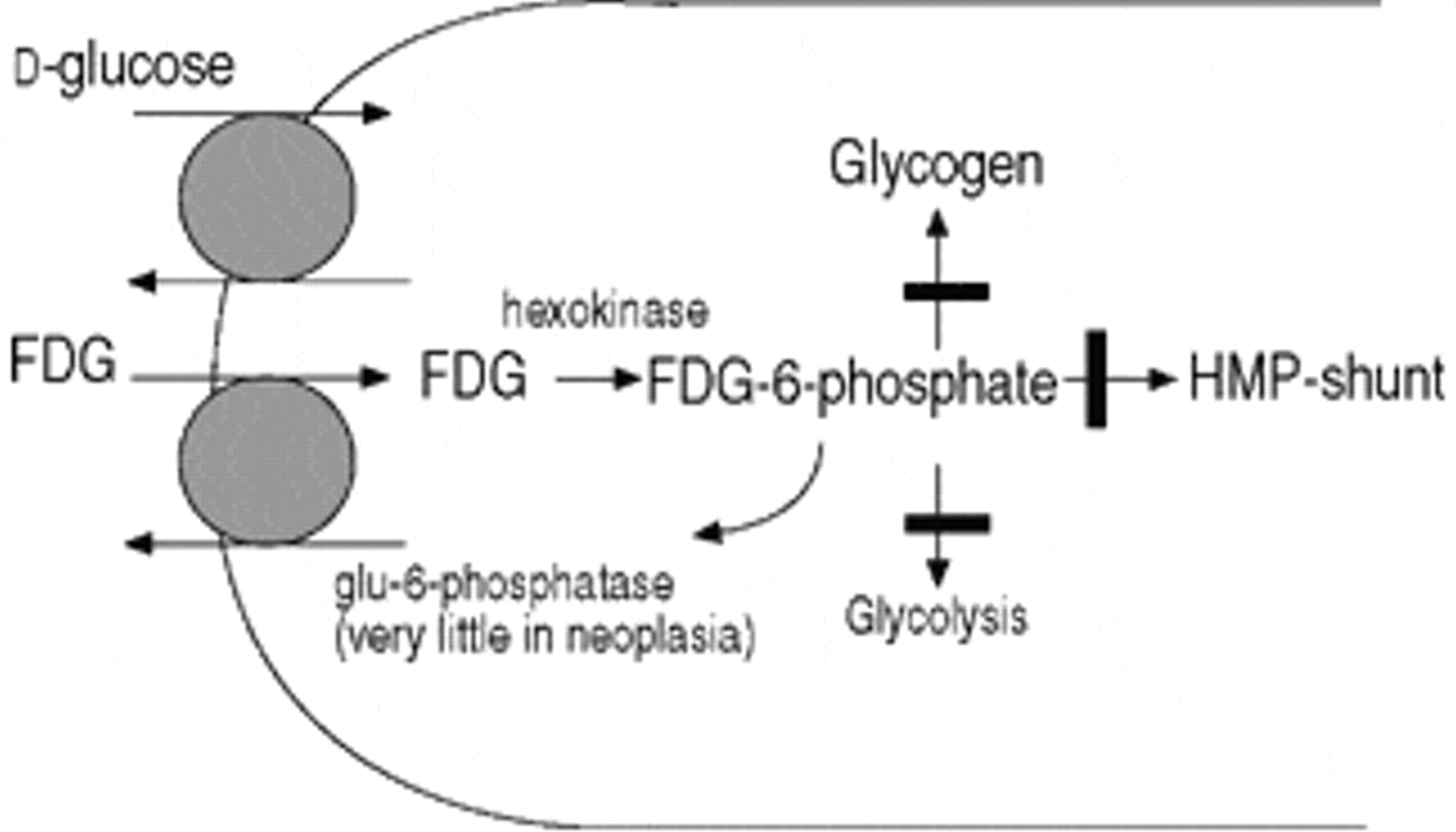
Lung tumour cells have an increased uptake of 18F-fluoro-2-deoxy-d-glucose (FDG) and an increased activity of hexokinase generating large amounts of FDG-6-phosphate. This glucose analogue is metabolically trapped and accumulated in the neoplastic cell. HMP: hexose monophosphate pathway.
Positron-emitting isotopes such as 18fluorine have an excess of protons and are, therefore, unstable. They decay by emission of a positron, which is the subatomic, positively charged, antiparticle of the negatively charged electron. The positron released in this process has kinetic energy, travels a short distance, and then annihilates with an electron. This annihilation creates two 511 keV photons, emitted in opposite directions. The detection of a number of these annihilations by the detector rings of the PET-camera generates high resolution pictures (resolution 5–10 mm) indicating the sites of FDG accumulation in the body 10. The preferential accumulation of FDG in neoplastic cells permits differentiation between benign and malignant tissue. In this way, FDG-PET compliments the anatomical information on standard imaging with “metabolic” information.
In contrast to the rapidly evolving data on the role of FDG-PET in non-small cell lung cancer (NSCLC), there are only a few anecdotal reports dealing with small cell lung cancer 11, 12.
After a short technical note on PET scanning protocols, this review will mainly focus on the current clinical indications of FDG−PET: diagnosis of lung nodules and masses, and staging of NSCLC (table 1⇓). For these indications, there is already reimbursement in several European countries. It continues with a short overview of the studies on other applications in NSCLC, and end with some prospects for the future.
Indications for 18f-fluoro-2-deoxy-d-glucose positron emission tomography (FDG-PET) in respiratory oncology
Technical note
The behaviour of FDG in normal and neoplastic tissues can be studied with different PET acquisition protocols.
Nonattenuation corrected whole-body images
This is the most commonly used imaging protocol in clinical oncology studies (fig. 2⇓). FDG is injected outside the PET-camera. After an uptake period of ≥1 h, necessary to obtain a good tumour to normal tissue contrast, the patient is positioned into the camera. Since the field of view of the PET-camera is only 10–15 cm, different bed positions need to be scanned to obtain a whole-body survey. At the end, the data of the different bed positions are reconstructed to a whole-body image by a computer algorithm, taking into account the physical decay of the FDG tracer during the examination. The advantage of this technique is that it allows a fast acquisition (usually <45 min) of information of the total body. The disadvantage is that, since no attenuation correction is performed, this technique only generates images for visual interpretation.
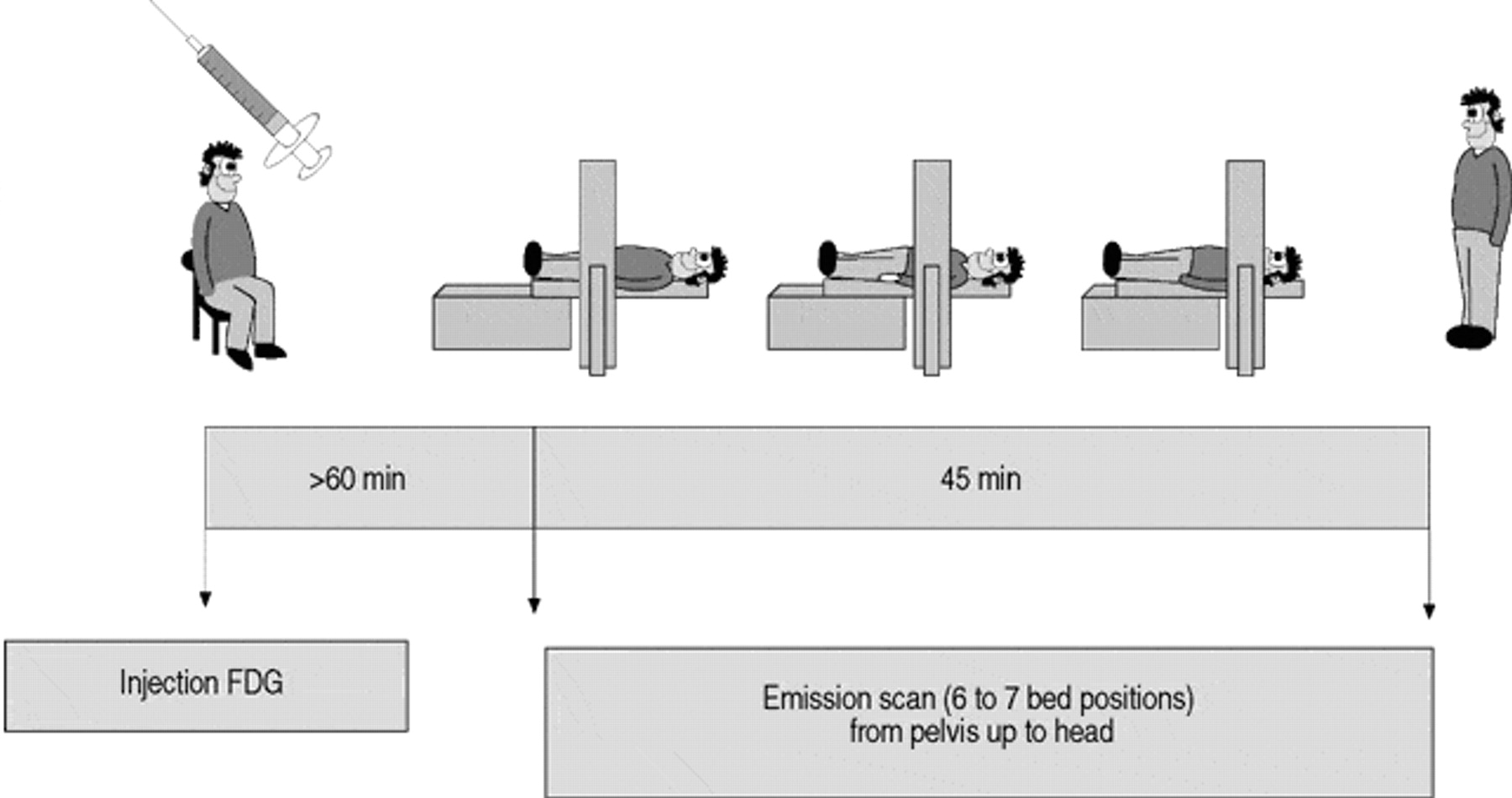
Protocol of nonattenuation corrected 18F-fluoro-2-deoxy-d-glucose positron emission tomography (FDG-PET). Approximately 1 h after injection of FDG, when a more or less stable distribution in the tissues has occurred, a whole-body emission scan is acquired during 6–7 camera positions.
Attenuation-corrected images
An important number of the emitted photons are absorbed in the patient's body. This absorption depends on the position in the body (e.g. superficial lesions are less attenuated than those situated in deeper layers of the body) and the type of surrounding tissue (e.g. lung tissue is less attenuating than muscle tissue). Since the intensity of photon emission of a lesion is position dependent, the intensity seen on the nonattenuation corrected whole−body images (figs. 2 and 3⇑⇓) does not truly reflect the actual FDG-uptake. If the images are corrected for photon attenuation by a so-called transmission scan, which makes an estimate of the attenuating characteristics of the patient, quantification of the FDG-metabolism becomes possible. This transmission scan, which can be performed prior to (“cold transmission”) or after (“hot transmission”) FDG-injection, will prolong the acquisition time substantially.

a) Nonattenuation corrected protocol as described in fig. 2⇑ (duration 40 min). b) Attenuation corrected protocol with “cold” transmission scan before injection of 18F-fluoro-2-deoxy-d-glucose (FDG) (duration 150–180 min). c) Attenuation corrected protocol with “hot” transmission scan after injection of FDG (duration 60–80 min). PET: positron emission tomography; □ : FDG injection; └ : FDG-uptake phase; ┘ : transmission/bed position;  : emission/bed position.
: emission/bed position.
In absolute quantification protocols, in which the FDG-uptake can be expressed in mg·g-1 tissue, certain kinetic models that describe the behaviour of FDG in a tumour cell are used 13. This quantification, however, requires a dynamic acquisition over the target lesion from the time of injection until a steady- state situation is reached (usually ≥1 h) and arterial blood sampling to measure the FDG input function. Since this procedure is time-consuming, rather invasive, and allows imaging in only one camera position (10–15 cm of the patient), its use is limited to more fundamental research studies (e.g. functional brain research 14, 15), and has little application in clinical lung cancer imaging.
The FDG-uptake in most clinical studies is expressed by the standardized uptake value (SUV). The SUV of a lesion is a semiquantitative index of the glucose utilization that is obtained by normalizing the accumulation of FDG in the lesion to the injected dose and patient's body weight 16. Compared to the absolute quantification, no dynamic data are necessary, which allows evaluation of different bed positions and thus a larger field of view in the same image session.
Initially, the transmission scan to correct for photon attenuation could only be performed prior to FDG-injection (“cold transmission”, fig. 3⇑). After FDG-injection, the patient had to remain without any movement in the PET-camera for ∼1 h, the time needed to obtain a good tumour to normal tissue contrast. Then the acquisition of the emission images, usually limited to two or three bed positions, completed the examination. A total camera time of nearly 3 h was needed for the entire sequence. With the introduction of “hot transmission” i.e. acquisition of transmission images after injection, and alternating with emission images, on the new PET-devices, and the development of new reconstruction methods to decrease transmission time, whole-body attenuation corrected images can now be obtained in a time of 60–80 min (fig. 3⇑) 17, 18.
Dual-head gamma camera coincidence imaging
The conclusions on the use of FDG-PET in respiratory oncology are mainly based on studies with high performance PET-cameras (so-called dedicated PET scanners), characterized by a high resolution and sensitivity. Because of the cost of a dedicated PET-camera, a considerably cheaper alternative has been designed by adding coincidence imaging to a dual-head gamma camera (gamma camera imaging: GCI). The crystals used in the gamma camera, however, have less stopping power for high energy photons compared to the ones used in dedicated systems, which results in a decrease in positron emission detection and, thus, in sensitivity 19.
Some studies have compared GCI with dedicated PET in lung cancer, usually on a limited number of cases, in 23 20, 27 21, 28 22 and 31 patients 23. Some series suggested that both techniques are equivalent. These series usually included larger lesions visible on both techniques. In a more challenging study, GCI detected 13 (93%) of the 14 lung nodules seen on PET, 20 (65%) of the 31 metastatic mediastinal nodes, and only 27 (42%) of the 64 distant metastases 23. Another study found an 86% overall accuracy in staging lung cancer with FDG−PET, compared to only 64% with GCI 22. Present experience suggests that the sensitivity of CGI clearly decreases for lesions smaller than 2 cm. Obviously, this has consequences for the detection of small metastatic deposits in mediastinal nodes or distant sites. One should thus be very careful in extrapolating the conclusions on clinical decision making obtained with dedicated PET to a situation where GCI is used.
Current clinical indications
Diagnosis of lung nodules and masses
Clinical setting
Central lung tumours can usually be diagnosed by fibreoptic bronchoscopy. Peripheral solitary pulmonary nodules (SPN) often represent a diagnostic challenge, especially if they are noncalcified 24. Absence of growth over a 2-yr period is highly suggestive of a benign lesion, but often comparative chest radiographs are not available 25. Bronchoscopic samples taken in patients with a peripheral nodule <3 cm yield a pathological diagnosis in only 20% of the cases 26. A transthoracic needle aspiration biopsy has a higher diagnostic yield, but can be complicated by a pneumothorax, requiring drainage in 5–10% of procedures 27. Moreover, the technique is still hampered by the possibility of a false negative test result, which carries the risk of an unacceptable expectation in patients with early-stage lung cancer 28, 29. Often, more invasive procedures such as thoracoscopy or thoracotomy are needed for a final diagnosis. Consequently, a reliable, noninvasive imaging test, able to differentiate between benign and malignant nodules, could be very useful.
18F-fluoro-2-deoxy-d-glucose positron emission tomography data
FDG-PET has been studied extensively in the evaluation of indeterminate lung lesions 30–41 (fig. 4⇓). The prospective studies in this indication are listed in table 2⇓. The technique has proven to be accurate in differentiating benign from malignant lesions as small as 1 cm. In general, there appears to be no significant difference in accuracy when a visual analysis of whole-body images and a semiquantitative approach using a threshold SUV of 2.5 are compared 31, 41, 42. When data from table 2⇓ are put together, an overall sensitivity of 96% (range 83–100), a specificity of 79% (range 52–100) and an accuracy of 91% (range 86–100) are obtained. The different results of the series can be explained by the prevalence of malignancy in the study population, which is the result of the varying epidemiology of solitary pulmonary lesions in different areas of the world (e.g. more histoplasmosis in North−America than in Europe). Another factor is the inclusion criteria of the different series (e.g. a lower sensitivity can be expected in series on very small nodules).

a) and b) Suspected coin lesion in the left upper lobe on computed tomography (CT), clearly 18F-fluoro-2-deoxy-d-glucose (FDG)-positive on positron emission tomography (PET)-images. Peripheral adenocarcinoma at resection. c) and d) Suspected coin lesion in the right upper lobe on CT, unremarkable on PET-images. Necrobiotic nodule at resection.
Prospective series on the use of 18f-fluoro-2-deoxy-d-glucose positron emission tomography (FDG-PET) in the differential diagnosis of lung nodules or masses
A critical mass of metabolically active malignant cells is required for PET diagnosis. Therefore, false negative findings can occur in lesions <10 mm 32, 34, 38, 39, 43, in tumours with low metabolic activity (e.g. carcinoid tumours 34, 44), or in bronchioloalveolar cell carcinoma 43, 45–47. It should also be mentioned that the sensitivity of FDG-PET is probably slightly less in the lower lung fields, due to respiratory motion. Finally, in small lesions (mostly for lesions <15 mm, depending on the resolution of the PET system) the FDG-uptake is underestimated because of partial volume effects (i.e. the activity of the lesion is averaged with the activity of a rim of normal tissue surrounding the lesion).
FDG-uptake is not specific for malignancy, and false positive findings can occur in inflammatory conditions such as bacterial pneumonia 48, pyogenic abscess or aspergillosis, granulomatous diseases such as active sarcoidosis 49, tuberculosis, histoplasmosis, coccidiomycosis, Wegener's disease and coal miner's lung. In these lesions, the FDG-uptake has been attributed to an increase in granulocyte and/or macrophage activity 50.
For some lesions with equivocal findings on whole-body images or with a SUV 2–3, the use of dynamic measurement of FDG-uptake can be of additional benefit 41 to discriminate inflammatory from malignant lesions. The substantially longer scan-time required for these dynamic studies is, however, not justifiable in the clinical routine.
In North-American series, it was shown that FDG-PET reduced the number of patients with an indeterminate SPN undergoing unnecessary resection of a benign lesion by 15%. This resulted in a decrease in cost of US$1,192 per patient 51, 52. It is not yet clear whether this cost saving will also be present in Europe. In a Japanese study, the use of FDG-PET was unlikely to be cost-effective, maybe because of the different prevalence of malignancy in patients with a SPN in Japan and the differences in cost of surgical procedures 53.
Clinical application of 18F-fluoro-2-deoxy-d-glucose positron emission tomography
Possibilities and limitations of FDG-PET in the patient with a SPN should be considered. The key question for the clinician is: “below which SUV can an SPN be considered benign and is expectation justified?” Most literature series use the criterion that an SPN with a SUV <2.5 (or with a low uptake on whole-body images) is likely to be benign. With its sensitivity of 96%, FDG-PET will indeed have a very good negative predictive value, and will be able to exclude malignancy correctly in the vast majority of cases. In these patients, a thoracotomy can be avoided, and a repeat chest radiograph or CT scan at 6 or 12 months can be used to confirm the absence of growth.
Difficult situations, where the critical mass of metabolically active malignant cells required for an SUV >2.5 is not always present, are: 1) Lesions <10 mm; other clinical (age, smoking history) and radiological (spiculation) factors determining the likelihood of malignancy should be considered where a specific CT-study 54, 55, very close follow-up, or more invasive tests can be appropriate. 2) Tumours with low metabolic activity; carcinoid tumours are the most common example, but this tumour usually has a central location, amenable to bronchoscopic biopsy 56. 3) Bronchioloalveolar cell carcinoma; in most of these cases, other features, especially on CT 57, will be suggestive for the diagnosis, and will point at the scrutiny needed for interpretation of the FDG-PET results. With its specificity of 79%, FDG-PET will also have a good positive predictive value, but not as good as its negative predictive value. A positive scan is possible in the previously listed inflammatory conditions, which should be excluded by appropriate tests in case of clinical suspicion. In case of doubt, lesions with increased FDG-uptake should, however, be considered malignant until proven otherwise, and managed accordingly.
Locoregional staging: primary tumour (T status) and locoregional lymph nodes (N Status)
Clinical setting
Accurate staging is essential to make estimates of prognosis, and to choose the best combination of treatment modalities such as surgery, radiation and chemotherapy, in an attempt to improve survival and optimize the use of imaging resources.
Extension of the primary tumour is usually assessed by thoracic CT, occasionally complemented by MRI, e.g. in situations where superior sulcus extension or relationship with the heart or large vessels is of importance 58. With their exquisite anatomical detail, modern CT and MRI are the preferred tests to evaluate the T-factor. FDG-PET offers no extras in this respect, due to its limitations in spatial resolution and anatomical detail within the image.
Perhaps even more important for the prognosis is the locoregional lymph node (LN) spread. Patients without malignant LNs in the mediastinum are usually treated with straightforward surgical resection. Patients with diseased mediastinal LNs are candidates for induction chemotherapy up-front, followed by surgery and/or radiotherapy 59–63. It is therefore of considerable clinical interest to evaluate these mediastinal LNs as accurately as possible.
CT is the most commonly used noninvasive staging method of the mediastinum, but is far from satisfactory and less accurate than invasive surgical staging (ISS) 64–67. In prospective data from the Radiological Diagnostic Oncology Group, the sensitivity and specificity of thoracic CT were only 52% and 69%, respectively 68. In the authors' (the University Hospital Gasthuisberg), the best results were obtained when LNs ≥1.5 cm at their maximal cross-sectional diameter were considered to be metastatic 69. Using this criterion, the sensitivity was 69% and the specificity 71%. Given this very moderate level of accuracy of CT, ISS by mediastinoscopy remained, until recently, the only adequate tool for mediastinal LN staging. FDG-PET as a noninvasive tool for determination of LN spread has thus been examined extensively.
18F-fluoro-2-deoxy-d-glucose positron emission tomography data
An important number of prospective studies have compared the performance of CT and FDG-PET in mediastinal LN staging in potentially operable NSCLC 30, 70–85 (fig. 5⇓). In all but one 82 of these studies, FDG-PET proved to be more accurate than CT. Quite evidently, a recent meta−analysis has confirmed this finding 86. Additionally, FDG−PET can indicate suspect LNs in stations not amenable to ISS by mediastinoscopy.

a) Computed tomography (CT)-image of a patient with left upper lobe tumour without suspect adenopathy in the mediastinum (N0-disease). b) and c) Transaxial and frontal positron emission tomography (PET)-images suggest N3-disease with left and right paratracheal lymph node metastasis (arrows), which was confirmed at mediastinoscopy.
Most of the studies have reported the results on a per patient basis, and compared the accuracy of CT and FDG-PET in distinguishing between presence (N2–N3) or absence (N0–N1) of malignant mediastinal LNs (table 3⇓). When the results from table 3⇓ are put together, an overall sensitivity of 89% (range 67–100), a specificity of 92% (range 79–100) and an accuracy of 90% (range 78–100) are obtained for FDG−PET. For CT, the results are a sensitivity of 65% (range 20–86), a specificity of 80% (range 43–90), and an accuracy of 75% (range 52–79). The information in table 3⇓ also shows that studies in which FDG-PET images are interpreted with the aid of CT (complementary) usually have slightly better results than those in which FDG-PET images are read independently. In the two studies, that directly compared these two methods of interpretation, an additional gain in sensitivity was noted: from 67–93% 75 in one, and from 73–82% in the other 77. This difference is the expression of the fact that the precise anatomic information on CT is complementary to the metabolic information images of FDG−PET, which lack precise anatomical detail. Therefore, the correlative interpretation will help in the distinction between, for example, central tumours and adjacent LNs, or between adjacent LN stations. This difference is of critical importance if the distinction is to be made between hilar and adjacent right tracheobronchial or subaortic nodes, and thus between N1 (operable) and N2 (nonoperable) disease. A study in the authors' centre addressed the question of whether digitally fused CT and FDG-PET images (so-called anatometabolic fusion images) could further increase the accuracy of noninvasive LN staging 74. It was found that, for an experienced reader, the gain in accuracy compared to visual correlation was very small, since the errors due to minimal tumour load (false negatives) or inflammation (false positives) were not corrected.
Prospective comparator studies of computed tomography (CT) and 18f-fluoro-2-deoxy-d-glucose positron emission tomography (FDG-PET) in mediastinal lymph node staging in non-small cell lung cancer, reporting the results per patient
In one of the authors' studies, it was examined if the use of an SUV threshold for LNs improved the results, compared to simple visual analysis 72. The best SUV threshold to distinguish benign from malignant LNs was 4.4, but the analysis with the SUV threshold did not prove to be superior to the simple visual reading.
Some studies have reported the results on a per LN station basis, and compared the accuracy of CT and FDG-PET in the detection of metastatic deposits in the different LN stations 72, 74, 78, 79, 81, 84, 85 (table 4⇓). These studies have convincingly demonstrated that the superiority of FDG-PET can be explained by the more frequent correct identification of “small malignant nodes” and “large benign nodes”. Indeed, the moderate accuracy of CT in LN staging is explained by the fact that size is a relative criterion. LN can be enlarged due to infectious or inflammatory causes, and small-sized nodes can nonetheless harbour metastases 64, 67–69, resulting in overstaging as well as understaging.
Prospective comparator studies of computed tomography and 18f-fluoro-2-deoxy-d-glucose positron emission tomography (FDG-PET) in mediastinal lymph node staging in non-small cell lung cancer, reporting the results per lymph node station
False negative findings can occur when the tumour deposit in the mediastinal nodes is small. In the authors' experience, this was mainly the case in some patients with minimal areas of metastatic cells in LNs with a maximal diameter rarely exceeding 2.5 mm (unpublished data). False positive images are possible in LNs containing anthracosilicosis 36 or inflammatory tissue with high metabolic activity. In some cases, however, no particular pathological abnormalities explaining the false positive FDG image can be found (unpublished data).
Clinical implication of 18F-fluoro-2-deoxy-d-glucose positron emission tomography
How should mediastinal FDG-PET be implemented in clinical practice? In nonmetastatic NSCLC patients, survival results after resection are worthwhile in three groups: 1) those without metastasis in mediastinal lymph nodes at thoracotomy; 2) those with so-called “unforeseen N2” i.e. metastasis in ipsilateral mediastinal lymph nodes found at thoracotomy after a negative preoperative mediastinoscopy 87–92 and; 3) those with so-called “minimal N2” detected at mediastinoscopy (according to the International Association for the Study of Lung Cancer 93, minimal N2 is defined as “one positive lower mediastinal nodal station excluding subcarinal adenopathy”). Mediastinoscopy, therefore, plays a central role in the preoperative staging of potentially operable NSCLC: it will be negative in groups 1 and 2, while it will confirm “minimal N2” in group 3. If mediastinoscopy shows “more than minimal N2” or N3 disease, the survival results of direct surgery are marginal 91, 94, 95, mainly due to the development of systemic relapses 96. These patients will be treated in a multimodality protocol, including induction chemotherapy followed by radiotherapy and/or surgery 59–63.
The issue whether FDG-PET is able to replace mediastinoscopy involves two questions. 1) Is it possible to proceed directly to thoracotomy in the case of a negative mediastinal PET? In the authors' view, yes, since mediastinal PET has a very high negative predictive value in the exclusion of N2 or N3 disease. Occasionally, a patient with a false negative mediastinal PET proceeds to straightforward thoracotomy, but in these cases “minimal N2” is found, where, as already mentioned, a reasonable prognosis after surgical resection can be expected 88. 2) Can we leave out straightforward thoracotomy in the case of a positive mediastinal PET? In the authors' view, no. Although the positive predictive value in the confirmation of N2 or N3 disease is also high, mediastinoscopy is still advised to prove N2 or N3 disease in patients with positive mediastinal nodes on PET. Mediastinal mapping by mediastinoscopy is justified before the start of a chemotherapy induction protocol, and is needed to ensure that no single patient with N0- or N1- disease is denied the chance of cure by direct surgical resection based on a false positive PET.
Even when only the high negative predictive value of mediastinal PET is implemented, this resulted, in the authors' experience, in nearly a 50% reduction of the number of mediastinoscopies. In the USA, it has been suggested that the use of a combined FDG-PET and CT strategy is more cost-effective than CT alone in the staging of NSCLC 52, 97.
Extrathoracic staging (M status)
Clinical setting
The finding of extrathoracic metastases implies that a patient is no longer amenable to long-term remission or cure. Standard staging for extrathoracic disease is based on clinical and biological factors, and imaging tests, such as CT, ultrasound, or bone scintigraphy. Whether these examinations need to be performed in every patient remains controversial. This issue is beyond this review, and the authors only refer to some recent guidelines 98, 99.
Current standard staging is far from perfect. After radical treatment for apparently localized disease, the present authors have found that an important proportion of patients, ranging from 20 100 to 22% 101, 102, will nonetheless have an early distant relapse. This means that detection of micrometastases that are already present at the time of initial staging is not possible 103. The most common sites of metastasis are the adrenal glands, bones, brain, and liver 104. Up to 35–45% of the patients will have detectable distant disease at presentation 105.
18F-fluoro-2-deoxy-d-glucose positron emission tomography data
In the detection of bone metastasis, 99m-technetium-methylene-diphosphonate (99mTc-MDP) scintigraphy is considered to be the most practical technique for assessing the entire skeleton. It has a reasonable sensitivity of ∼90%, but the clinical interpretation is hampered by its low specificity (false positive findings in arthrosis, arthritis, post-traumatic abnormalities, etc.). Often, additional studies such as bone radiographs, bone CT, or bone MRI are needed. One study pointed at an equivalent sensitivity of FDG-PET and 99mTc-MDP bone scintigraphy, but with a much higher specificity for FDG-PET (98% versus 61%) 106. In another series, FDG-PET proved to be more sensitive than 99mTc-MDP bone scintigraphy, and allowed better differentiation between benign and malignant lesions 107. Whether FDG-PET can replace 99mTc-MDP bone scintigraphy remains an open question. Studies in breast cancer have indicated false negative FDG-PET findings in bone metastases, especially in osteoblastic lesions 108, 109. Obviously, more data are needed to answer this question. Another point in this discussion is the fact that a whole-body FDG-PET gives an image from the head to just below the pelvis, while a standard 99mTc-MDP bone scintigraphy images the entire skeleton.
Adrenal masses are found in up to 20% of NSCLC patients at initial presentation 110–112. The finding of an isolated adrenal mass on CT is often a diagnostic challenge. About two-thirds of cases could be explained by an asymptomatic adrenal adenoma in some series 110, 113. An adrenal mass, therefore does not imply inoperable disease, but rather the need for further (pathological) examination by, for example, puncture or biopsy of the lesion 113. FDG-PET can be a useful adjunct to other imaging modalities of the adrenals. The available (small) series point at a high sensitivity of FDG-PET in the detection of adrenal metastases 114–116. An equivocal lesion on CT without FDG-uptake on PET will usually not be metastatic. However, it is necessary to be very careful with the interpretation of small lesions. Indeed, the available series have studied lesions with an average diameter of 30 mm. Specificity in the available data lies 80–100%, because some false positive findings have been described 114. In the case of an isolated FDG-positive adrenal lesion, pathological proof is still required before a decision towards inoperable disease is made.
The evaluation for liver metastasis is usually less difficult because the liver is less frequently an isolated site of disease, and because the combination of ultrasonography and CT can solve most cases 117. There are no series that specifically focus on the performance of FDG-PET in the evaluation of liver lesions in NSCLC patients. Data from studies on staging of NSCLC in general, suggest that FDG-PET is more accurate than CT in liver staging, mainly because of better specificity 118, 119. A series on examination of the liver in patients with different primary tumours reported a sensitivity of 97% and a specificity of 88% for FDG-PET, in comparison to 93% and 75%, respectively for CT (a nonsignificant difference) 120. Similar findings have been reported in studies on colorectal 121, 122, pancreatic 123 or oesophageal tumours 124. False positive findings have been described in some liver abscesses 125. The main advantage of FDG-PET is its ability to differentiate hepatic lesions that remain indeterminate by conventional studies: in one study, FDG-PET accurately indicated liver metastases in 11 patients, two with negative and nine with equivocal conventional imaging. On the other hand, FDG-PET could exclude metastasis in four cases with suspect conventional imaging 120.
In the authors' experience, FDG-PET was also of help in some patients in the detection of metastases that otherwise could have escaped notice, for example, small nodules in the other lung, soft tissue lesions, retroperitoneal LNs, hardly palpable supraclavicular LNs, etc. Finally, FDG-PET also pointed at a coexistent asymptomatic second primary tumour, mainly of colorectal origin.
FDG-PET is not suited for the detection of brain metastasis. The sensitivity of FDG-PET in the detection of brain lesions is low, because the surrounding normal brain tissue has a high glucose uptake. CT and/or MRI remain the standard imaging tests in this indication 126.
Clinical implication of 18F-fluoro-2-deoxy-d-glucose positron emission tomography
Whole-body FDG-PET improves the imaging of metastases for two reasons. 1) It is able to detect metastatic lesions that would have been missed on conventional imaging, or in clinically hidden or difficult areas (bone, liver, soft tissue, some LNs, etc.) (fig. 7⇓). Since most of the organ-specific literature series are still on small numbers of patients and contain some false positive findings, it should be a golden rule to obtain verification by other methods or by tissue sampling of an isolated positive finding that determines resectability. 2) It is able to exclude malignancy in lesions that are equivocal on conventional imaging (fig. 8⇓). Exclusion of malignancy by FDG-PET should be done with caution in case of small lesions, e.g. adrenal nodules of <1 cm.

Importance of computed tomography-positron emission tomography (CT-PET) correlation. a) Two suspect lesions (arrows) are present in the right lung on CT. b) Two suspect lesions in the right lung (arrows) are withheld on PET-images (N0-disease?). c) Correlation locates one of the 18F-fluoro-2-deoxy-d-glucose (FDG) hot-spots in the largest parenchymal lesion and the other one in a mediastinal node anterior of the superior vena cava (N2-disease). The small peripheral lung nodule does not exhibit FDG-uptake.

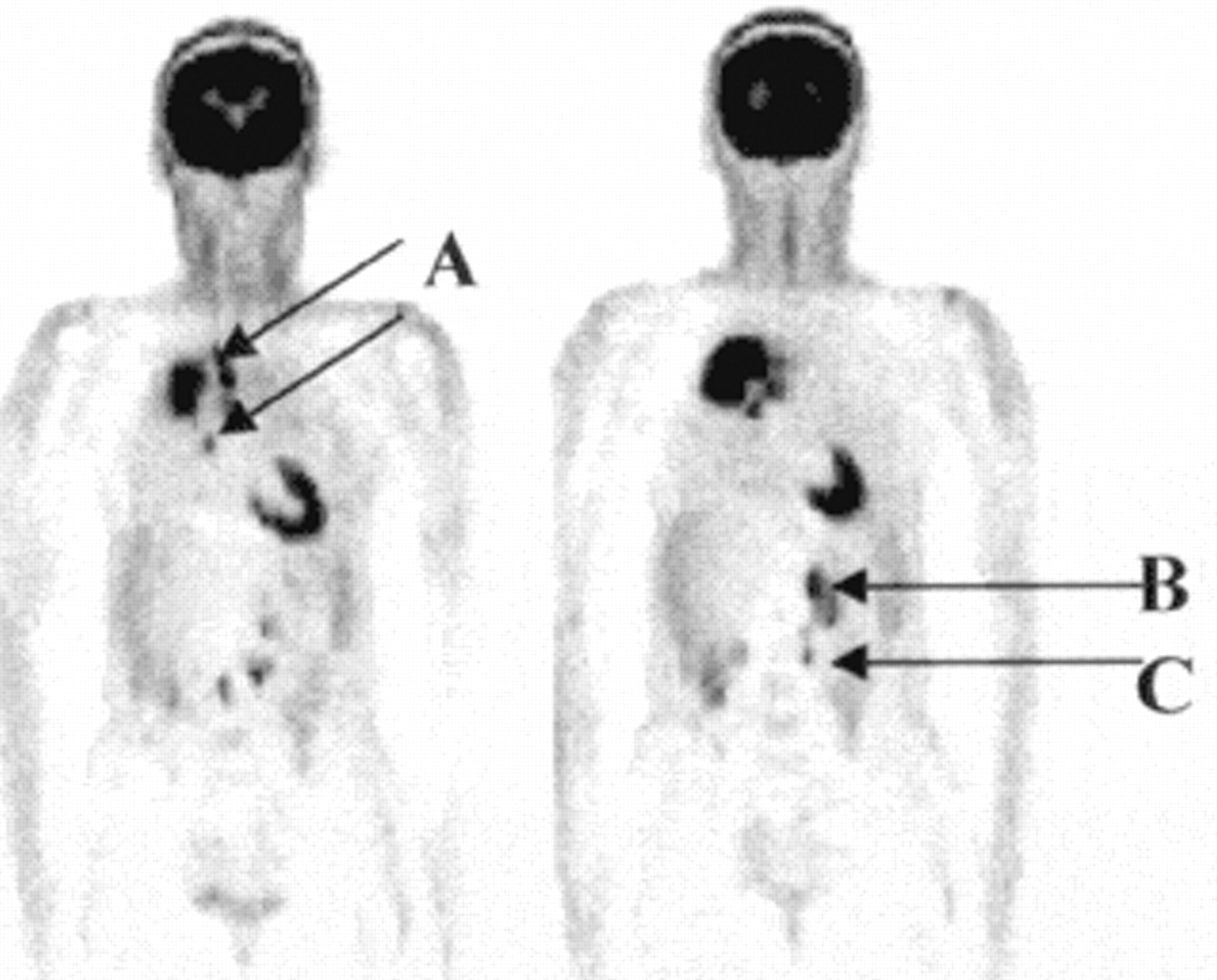
Patient referred for induction treatment for presumed stage IIIA-N2 disease. On 18F-fluoro-2-deoxy-d-glucose positron emission tomography (FDG-PET), a) mediastinal lymph node spread is very important, and b) unsuspected left adrenal and c) abdominal lymph node lesions are found.

a) Patient referred for chemotherapy for presumed T1N0M1 adenocarcinoma (A) with lumbar pain due to adrenal metastasis on computed tomography (CT). b) Positron emission tomography (PET)-images demonstrate 18F-fluoro-2-deoxy-d-glucose (FDG)-uptake in the primary tumour only. Surgical exploration revealed an adrenal adenoma with central bleeding (B).
Because whole-body FDG-PET is able to stage both intra- and extra-thoracic sites in one examination, and because of its greater accuracy than conventional imaging, this technique is reported to change patient management in 19% 119, 20% 118, 30% 71, 31% 127, or even 41% 128 of patients. Numerous data indicate that FDG-PET can complement conventional imaging, but the authors clearly do not have enough data to accept that FDG-PET can replace it. In contrast with the large amount of data on locoregional staging, most of the organ-specific studies are small, and did not include an adequate number of small lesions, which truly challenge the technique. Further studies of this type have to be awaited.
Other applications
Radiotherapy planning
Although most of the FDG-PET studies of locoregional NSCLC staging were performed in a preoperative setting, the use of this technique could be of equivalent importance in radiotherapy planning in nonmetastatic patients not suitable for surgery e.g. due to cardiopulmonary limitations. The extent of the tumour will not only influence the treatment intention, i.e. curative or palliative, but also the volumes to be treated and therefore the toxicity to be expected. Indeed, several authors have suggested that a dose-volume effect for radiopneumonitis exists 129–132.
Classical radiotherapy planning uses conventional imaging such as chest radiography and CT to describe the tumour and to draw the target volume for irradiation. The main limitations of this method are the poor demarcation of some tumours on CT, and the inability of CT to distinguish between benign and malignant LNs. In one study including 20 patients, twelve had poorly demarcated tumours. CT and FDG-PET volumes corresponded in seven patients, but in three of 12 patients, the CT abnormalities were larger than on FDG-PET, and in two of 12 patients the abnormalities on FDG-PET extended outside the region of CT changes 133. Another study pointed at the substantial reduction in radiation fields by FDG-PET in cases with postobstructive atelectasis 134.
As for the effect of LNs, a simulation study on the potential impact of FDG-PET on the radiation treatment plan of 105 patients with NSCLC was carried out at the authors' centre 135. For 73 of these patients, with positive LNs on CT and/or on FDG-PET, a theoretical study was performed in which for each patient the gross tumour volume (GTV) was defined based on CT and on PET-CT data. For each GTV, the completeness of tumour coverage was assessed, using the available surgical pathology data as gold standard. Tumour coverage improved from 75% when the CT-GTV was used, to 89% with the PET-GTV (p=0.0005). In 45 patients (62%) the information obtained from FDG-PET would have led to a change of the treatment volumes. It was concluded that assessment of locoregional LNs by FDG-PET improved tumour coverage. In selected patients, it also reduced the volume of normal tissues irradiated, and thus toxicity, opening possibilities for treatment intensification. Similar findings were reported in smaller studies 134, 136, 137. Future prospective comparative studies are indicated to examine whether these advantages of combined CT-PET planning will actually result in reduced toxicity, better local control, and increased survival.
Response evaluation postradiotherapy
Response after radiotherapy is usually evaluated by comparing tumour volumes on chest radiographs or CT images pre- and post-therapy. An important limitation of this method lies in the fact that changes in tumour viability (and thus prognosis) do not necessarily correlate with changes in volume. Data on the possible extra value of FDG-PET in NSCLC in this setting are still limited. In one study, tumours with a high FDG-uptake responded better to radiotherapy than those with a low uptake 138. Other series suggested that there was a correlation between volume changes on CT and decrease of FDG-uptake on PET, but that a persistently elevated FDG-uptake after radiotherapy predicted an early relapse, irrespective of the volume changes on CT 138, 139.
Response evaluation post (induction) chemotherapy
If the mediastinoscopy in potentially operable NSCLC patients is positive for N2-disease, the results of direct surgical resection (or radiotherapy) are very disappointing 88, 91, 94, 140, mainly due to systemic relapses 96. Rapidly increasing amounts of data indicate that effective systemic therapy (induction chemotherapy), followed by resection with mediastinal dissection, is a better treatment option for these patients 59–63. Many authors pointed out that clearance of viable tumour cells in the mediastinum (so-called downstaging) is very important for the long-term prognosis 141–146. It was further stressed, in the Memorial-Sloan-Kettering series on induction chemotherapy, that the estimated 5-yr survival rate of patients with a pathological complete response was 54%, while it was only 15% in those without pathological complete response 147.
After induction chemotherapy, one should ideally be able to select the patients with clearance of mediastinal involvement for radical surgical treatment, and to avoid it in the others. CT has not proven to be a good tool to evaluate downstaging after induction chemotherapy. It is well known that patients with little decrease in measurements on CT can nonetheless have mediastinal LN downstaging, while those with an important decrease can still have viable tumour in their mediastinal LN. On the other hand, a remediastinoscopy is hardly technically feasible, due to fibrosis caused by the chemotherapy and by the extensive sampling during the first mediastinoscopy.
In a prospective pilot study, the authors examined if FDG-PET could be a reliable noninvasive technique to solve this problem 148. FDG-PET proved to be 100% accurate in the evaluation of downstaging (versus 67% for CT). Furthermore, outcome after the entire combined modality treatment was correlated with the findings on the postinduction FDG-PET; survival was significantly better in patients with mediastinal clearance on FDG-PET (p=0.01) or with >50% decrease of the SUV of the primary tumour (p=0.03) after induction chemotherapy (fig. 9⇓). A larger prospective multicentre study is ongoing. If these preliminary findings can be confirmed, PET could become a useful noninvasive tool to select patients for intensive locoregional treatment after induction chemotherapy.

a) Computed tomography (CT) before and b) after induction chemotherapy: partial response (70% decrease in bi-dimensional measurement). Positron emission tomography (PET) c) before and d) after induction: decrease in volume confirmed, but only a -20% decrease in 18F-fluoro-2-deoxy-d-glucose (FDG)-uptake. This patient developed an early systemic relapse.
Diagnosis of recurrence
The interpretation of a post-treatment chest radiograph or CT can be hampered by anatomical changes such as distortion of bronchi, infiltration of the lung parenchyma or mediastinum, or fibrotic changes, which may be difficult to distinguish from tumour relapse. The exact differential diagnosis can be of importance, especially in the light of the expanding possibilities for second-line treatment 149–153.
In one study, FDG-PET gave a correct positive result in 16 indeterminate lung lesions after previous lung tumour resection 32. Other studies in patients whose CT images were suspect of recurrence have pointed at the possible distinction between post-therapy scarring and new viable tumour with sensitivity for FDG-PET 97–100%, specificity 62–100%, and accuracy 78–98% 133, 154–158. False positive studies may occur if the FDG-PET is performed shortly after surgery or radiotherapy. These false positive findings are ascribed to either radiation pneumonitis or macrophage glycolysis in tumour necrosis 157. An interval 4–6 months after therapy is recommended to be sure that inflammatory changes have subsided, so that adequate assessment of tumour viability is possible.
Prognosis
The TNM-staging is the most important tool to estimate the prognosis of NSCLC patients. It does not, however, always give a satisfactory explanation for differences in survival. Resected stage I NSCLC is a typical example; many patients are cured, but some have an early relapse and die. Recent advances in molecular biology 159 have already helped to increase understanding of different patterns of survival in resected stage I NSCLC 160, 161. For instance, in the Boston experience based on a molecular-biologic staging including angiogenesis, proto-oncogene erbB-2, suppressor gene p53, and the proliferation marker KI-67, a 5-yr survival of 81% was found in resected stage I NSCLC patients without any adverse marker, while it was only 49% in those with ≥3 markers 162.
Since NSCLC is characterized by important carbohydrate metabolic derangement's, which have also been identified as independent prognostic factors correlated with poor treatment response and survival 163, 164, measurement of the glucose metabolism in vivo with FDG-PET might have prognostic importance. This hypothesis is further substantiated by the finding that FDG-uptake in NSCLC cells is correlated with growth rate and proliferation capacity 165.
In one of the authors' studies, it was examined whether the SUV of the primary tumour at baseline was predictive for the prognosis after treatment in 125 NSCLC patients 166. It was found that an SUV of the primary tumour >7 had independent prognostic value, apart from the performance status and stage. In patients with a resected T1 tumour, the 2-yr survival was 86% if the SUV was <7, and 60% if >7. Similar findings, based on a cut-off SUV of 10 were reported by another group 167. These researchers also examined the prognostic value of FDG-PET after primary treatment 168. They found that patients with a positive FDG-PET after initial treatment had a median survival of 12 months, in contrast with those with a negative FDG-PET, of whom 85% were still alive at the time of analysis, after a median follow-up of 34 months (p=0.002).
Conclusions and future directions
The indication of FDG-PET as a complimentary tool to CT in the diagnosis and staging of NSCLC gradually gains widespread acceptance and also reimbursement in many European countries. A summary of its possible clinical implementation is depicted in figure 10⇓. Further development is expected when commercial isotope distributors will be able to deliver FDG, so that an on-site cyclotron is no longer a prerequisite. 18FDG has a half-life of 110 min, so a practical distribution radius 200–300 kilometres should be feasible. Another factor will be the more widespread availability of PET-cameras. The question whether the use of dual-head GCI will be a useful substitute still requires a large amount of carefully controlled clinical studies. It is also expected that the resolution and performance of both dedicated PET and dual-head GCI will still improve in the future 169. The use of FDG-PET in the current clinical indications now needs further validation in multicentre, large-scale, randomized studies, focusing mainly on treatment outcome parameters, on the question whether FDG-PET actually improves survival prospects and on cost-efficacy issues. Other indications, such as evaluation of radio- or chemotherapy, radiotherapy planning, recurrence detection and prognosis determination need further well designed prospective investigations in more specialized centres.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Algorithm for the implementation of 18F-fluoro-2-deoxy-d-glucose positron emission tomography (FDG-PET) in non-small cell lung cancer (NSCLC). LN: lymph node; M+: metastasis.
Finally, a whole new field using PET in molecular applications is under exploration. FDG, with it's possibility to study tumour glucose metabolism, has paved the way for PET in clinical oncology. Several other radiopharmaceuticals can also be used to study processes such as blood flow (H215O), protein metabolism (11C−methionine, 11C−choline) and carbohydrate metabolism (11C−acetate) 170. One step further is the study by PET of cellular functions such as receptors, transport proteins or intracellular enzymes. The use of PET to study the efficacy of gene therapy in cancer is one example 171, 172. Another example is how PET could be used as a guide in the selection or early assessment of anticancer therapy. Nowadays, it is difficult to predict response to chemotherapy and the choice of a chemotherapy regimen is mainly empirical. It is necessary to wait for the repeated chest radiograph or CT after several cycles before it can be determined whether therapy actually worked, thus, losing time and perhaps exposing the patient to needless toxicity. Ideally, it should be known what happens at the cellular level. Some years ago it was already reported that FDG-PET could demonstrate a significant decrease in tumour glucose metabolism after effective treatment for breast cancer, with a reduction in the glucose metabolism before the radiological decrease in tumour size 173. PET with 11C-thymidine or its analogues could theoretically evaluate the efficacy of a treatment very shortly after the first dose, since 11C-thymidine is rapidly incorporated into DNA, and thus mirrors proliferation of neoplastic cells 174. After demonstration of the possibility of PET imaging with thymidine, the feasibility of measuring the response to chemotherapy in humans with 11C-thymidine was recently reported 175.
Problems still to be solved relate to the short half-life of 11C-thymidine (creating practical problems) and the rapid catabolism of thymidine in human cells, which creates major noise in the positron emission tomography image, unless very complex interpretation algorithms are used. Extensive research is ongoing to test new thymidine analogues with a longer half-life, with the same deoxyribonucleic acid incorporation properties, but minimized intracellular breakdown 176, 177. If this concept can be brought into practice, it would enable us to tailor therapy for a specific patient, and move faster ahead in testing new drugs in phase I and II clinical studies, by using the endpoint of subclinical positron emission response response 178.
Acknowledgments
The authors would like to thank the numerous other coworkers involved in the FDG-PET research program of the Leuven Lung Cancer Group (LLCG): Data-nursing LLCG (B. Anrys, D. Strens); Nuclear Medicine (P. Dupont, L. Mortelmans, S. Stroobants); Pathology (E. Verbeken); Pneumology (M. Demedts, K. Nackaerts); Radiology (J. Bogaert, W. De Wever, J. Verschakelen); Radiotherapy (Y. Lievens, L. Van Uytsel); Thoracic Surgery (P. De Leyn, G. Deneffe, T. Lerut, D. Van Raemdonck).
- Received October 12, 2000.
- Accepted January 10, 2001.
- © ERS Journals Ltd