



Allergic sensitization and diet: ecological analysis in selected European cities
- 1GSF National Research Center for Environment and Health, Institute of Epidemiology, Neuherberg and 2University of Applied Sciences Albstadt-Sigmaringen, Dept of Food and Hygiene Technology, Sigmaringen, Germany
- J. Heinrich, GSF National Research Center for Environment and Health, Institute of Epidemiology, D‐85758, Neuherberg, Germany. Fax: +498931873380
Abstract
It has been postulated that the prevalence of atopic diseases and their increase over time are associated with regional differences in diet and trends. The results of an ecological correlation study comparing the mean daily intake of selected dietary constituents and the prevalence of allergic sensitization in adults in Europe is presented.
Prevalence data from the European Community Respiratory Health Survey (ECRHS) were used. For eight out of 37 ECRHS centres (including 3,872 subjects), comparable dietary data could be obtained. The effect for each dietary constituent was modelled using logistic regression analyses with a term for over dispersion.
Inverse associations between the prevalence of allergic sensitization and the energy adjusted intake of fruit were found (odds ratio (OR)=0.68, p=0.034). Furthermore OR for energy adjusted intake of vitamin A (OR=0.73, p=0.057), vitamin C (OR=0.83, p=0.338) and riboflavin (OR=0.72, p=0.077) were consistently <1, but confidence intervals were wider. Daily intake of monounsaturated fatty acids (energy adjusted) was positively associated with sensitization prevalence (OR=1.59, p=0.035).
These results support the hypothesis that a high intake of monounsaturated fatty acids might promote the development of allergic sensitization.
- allergic sensitization
- antioxidants
- diet
- ecological study
- ECHRS
- fatty acids
Regional differences in the prevalence of asthma and allergic sensitization in adults 1, 2, in childhood 3, and the increase in asthma prevalence in many Western countries over recent decades 4, highlight the need for a greater understanding of the risk factors for asthma and allergic sensitization. The currently known environmental determinants of asthma seem to contribute very little to the observed increase in prevalence. It has been hypothesised that dietary constituents influence the immune system and thus, may be involved in the development of allergic diseases 5, 6, 7. The possible role of diet in the development of these atopic diseases may be summarised as follows. First, a food allergy can cause asthma attacks, thus avoidance of allergenic food may lead to improvement of respiratory symptoms. Second, a number of studies have investigated the role of breast feeding for prevention of asthma later in life, but the results are controversial 8, 9. Third, a low intake of antioxidative dietary constituents might be a risk factor for asthma 5. Vitamin A, C, E and other unspecified antioxidants prevent oxidative injury. Therefore, it may reduce inflammation caused by chemical oxidants derived from cigarette smoke, viral infections or allergen exposure 10. Results of a limited number of epidemiological studies relating the intake of antioxidants to respiratory health effects, suggested a consistent inverse association for the intake of vitamin C and asthma. The Zutphen Study reported a negative association between the intake of fruit and the risk of developing chronic nonspecific lung disease (CNSLD) (chronic cough, phlegm production, shortness of breath and wheezing) in middle-aged men over a 25-yr period after control of potential confounders 11. In contrast, the intake of vitamin A, beta-carotene, and vitamin C did not differ between incident CNSLD patients and healthy subjects 11. The authors argued that misclassification, especially with regard to vitamin A, may have occurred.
A fourth pathway of how diet may affect the development of asthma is through the role of cations like sodium, potassium and magnesium. However, this idea is still controversial 10. Finally, it has been suggested that the intake of fatty acids, especially the ratio of omega‐3 and omega‐6 fatty acids may be contributing to the development of asthma 6. However, results from two prospective studies that considered different respiratory health endpoints were not consistent. While the Zutphen Study revealed that higher intakes of monounsaturated (MUFA), polyunsaturated fatty acids (PUFA) and linoleic acid were associated with a higher incidence of chronic nonspecific lung disease 11, data from the Nurses Health Study showed inverse associations between the intake of MUFA and linoleic acid and asthma incidence 12. Recently published results using fish consumption as a proxy variable for the intake of omega‐3 fatty acids were consistent 13, 14.
The mechanisms of action proposed for dietary polyunsaturated omega‐6 and omega‐3 fatty acids include modulation of gene expression, signal transduction pathways and production of eicosanoids and cytokines 7, 14, 15. Predominance of linoleic acid (C18:2 omega‐6), compared to alpha-linoleic acid (C18:3 omega‐3), in the diet is thought to alter the T‐helper (Th)1/Th2 cell balance by production of arachidonic acid-derived eicosanoids, resulting in the stimulation of immunoglobulin (Ig)E production 7. On the other hand, unsaturated fatty acids in trans-configuration, occurring in ruminant fat, dairy products and industrially hydrogenated fats, have been found to exhibit inhibitory effects on desaturation and chain elongation of essential fatty acids into precursors of inflammatory mediators and on the activity of cyclooxygenase 16.
Although some researchers would argue that an allergic component contributes to >80% of young asthmatics and approximately 40% of adult asthmatics experience 17, the association between diet and nonfood allergies are widely ignored. To the best of the authors knowledge, Black and Sharpe (1997) 6 were the first to suggest that the effect of diet on asthma could be mediated through increase in the synthesis of prostaglandin E2. This could in turn promote the formation of IgE and consequently allergic sensitization. Apart from food allergy very little data on the associations between diet and allergy is available.
The European Respiratory Health Survey (ECRHS) using standardised methods provided data on the prevalence of allergic sensitization from 37 centres, distributed throughout Europe. These data were employed in the present ecological study testing the hypothesis that the intake of dietary antioxidants is inversely associated with allergic sensitization. The authors also examined whether a positive correlation exists between the intake of MUFA and PUFA and the prevalence of allergic sensitization.
Methods
Prevalence data on allergic sensitization
The study protocol of the ECRHS has been described in detail elsewhere 1. Prevalence data on allergic sensitization in random samples of 20–44 yr old subjects, taken from 37 centres located throughout Europe, were recently published 1. Allergic sensitization was assessed by measurement of specific IgE against Dermatophagoides pteronyssinus, timothy grass, cat, cladosporium herbarum and a local allergen using the Pharmacia CAP System 1.
Prevalence of overall allergic sensitization was estimated using 0.35 kU·l−1 as the cut-off (CAP class>0) of the specific IgE's. Age-sex-standardised prevalence of allergic sensitization was calculated using identical weights for males and females as well as for age groups. Only data from eight out of the 37 centres could be included in this ecological study because of a lack of appropriate dietary data from the other centres.
Dietary data
Dietary information from previous surveys conducted among adults living in or near any of the 37 ECRHS-centres was gathered through searches in Medline, Nutrition Abstracts and Reviews and personal contacts. To achieve a high comparability between the dietary information from different sources, the following inclusion criteria were applied: dietary data had to be: 1) collected 1985–1992 to cover similar years prior to the ECRHS survey; 2) based on records or recalls, which compared to the questionnaire-based data in general provide better retrospective comparability for the average intake in a group 18, 19, 20; and 3) gathered in randomly selected samples of the adult population. To receive enough data points, two exceptions from the criteria were made for the French and the Swedish centre 21, 22.
It was possible to obtain approximately contemporaneous data on both the prevalence of allergic sensitization (early 1990s) and adult diet, assessed by records or recalls (mid 1980s to early 1990s), from eight of the ECRHS centre's. These covered populations from the North, the West and the South of Europe. The dietary survey of the Catalan population 23 provided data that was used as a proxy for the intake in Barcelona, Spain. Data for Erfurt, Germany originated from a dietary survey carried out in connection with the Erfurt ECRHS 24, 25. The Dutch National Consumption Survey provided data for the South and the North of The Netherlands 20, 26, which was taken as a proxy for Geleen and Bergen-op-Zoom (Region South) and Groningen (Region North), respectively. A paper on the diet in three English cities by Cade et al. 27, contained dietary information for Ipswich, UK. Dietary data from a validation study in subjects from the Department of Hérault 22 supplemented by further data from this study (M. Gerber, Montpellier, personal communication), were used as a proxy for the intake in Montpellier, France. Data on dietary intake in Uppsala, Sweden was taken from a survey of all employees of the Swedish Telephone Company in Uppsala 21. The dietary surveys are described in table 1⇓.
Dietary surveys included into the present ecological study, by selected crieria
Since sex specific prevalence of allergic sensitization from the ECRHS is not yet published 1, sex-stratified dietary data were transformed into mean daily intake data for both sexes together (weighed 1:1). When age-stratified dietary data were available, only the age group that was most appropriate in relation to the 20–44 yr old ECRHS-populations, was taken into account.
Absolute intake values were taken as presented in the publications. For reasons of comparability, relative intake values were deduced as follows: percentages oftotal energy intake from macro nutrients (en%) werecalculated using the following factors: 1 g protein=17 kJ, 1 g fat=37 kJ, 1 g carbohydrates=17 kJ, 1 g alcohol=29 kJ. Nutrient density (g or mg/MJ)=mean daily intake of a nutrient/mean daily intake of energy; P/S ratio=mean daily intake of PUFA/mean daily intake of saturated fatty acids (SFA).
From the various dietary constituents under discussion, three food groups have been focused on including fruit, vegetables and fish, and the nutrient vitamins A, C and riboflavin and the fats, including SFA, MUFA and PUFA. With respect to vitamin A, only data of those surveys were included which refer to comparable vitamin A equivalents (retinol and all carotinoids). Data on vitamin E will not be presented because these data are available for 4 centres only.
Statistical analysis
The relationship between allergic sensitization and diet was examined separately for each dietary variable using logistic regression models. Since no detailed information on sensitization in the different age-sex-strata was available, the age-sex-standardised prevalence was treated like raw proportions. A parameter for over dispersion was also included in every model, because a single nutrient and the binomial variance alone cannot be expected to explain the total variation between the prevalence. The % GLIMMIX macro in the SAS package (version 6.12, Casy, NC, USA) was used for the computations. Results are presented as odds ratios (OR) comparing centres of maximal versus minimal intake of dietary constituents.
Results
Table 2⇓ shows the mean daily intake of selected dietary constituents in various European adult populations. The mean daily intake of energy ranged from 8.7 MJ·day−1 in Uppsala–10.7 MJ·day−1 in the two Dutch cities of Bergen-op-Zoom and Geleen (table 2⇓). The variations between the centres were more pronounced for the intake of protein, fat, and carbohydrates. Assessing the coefficients of variation of the various dietary constituents, the range of daily intake was largest for fish, followed by fruit and PUFA.
Prevalence of allergic sensitization and mean daily intake of selected dietary constituents in various European adult populations
Antioxidants
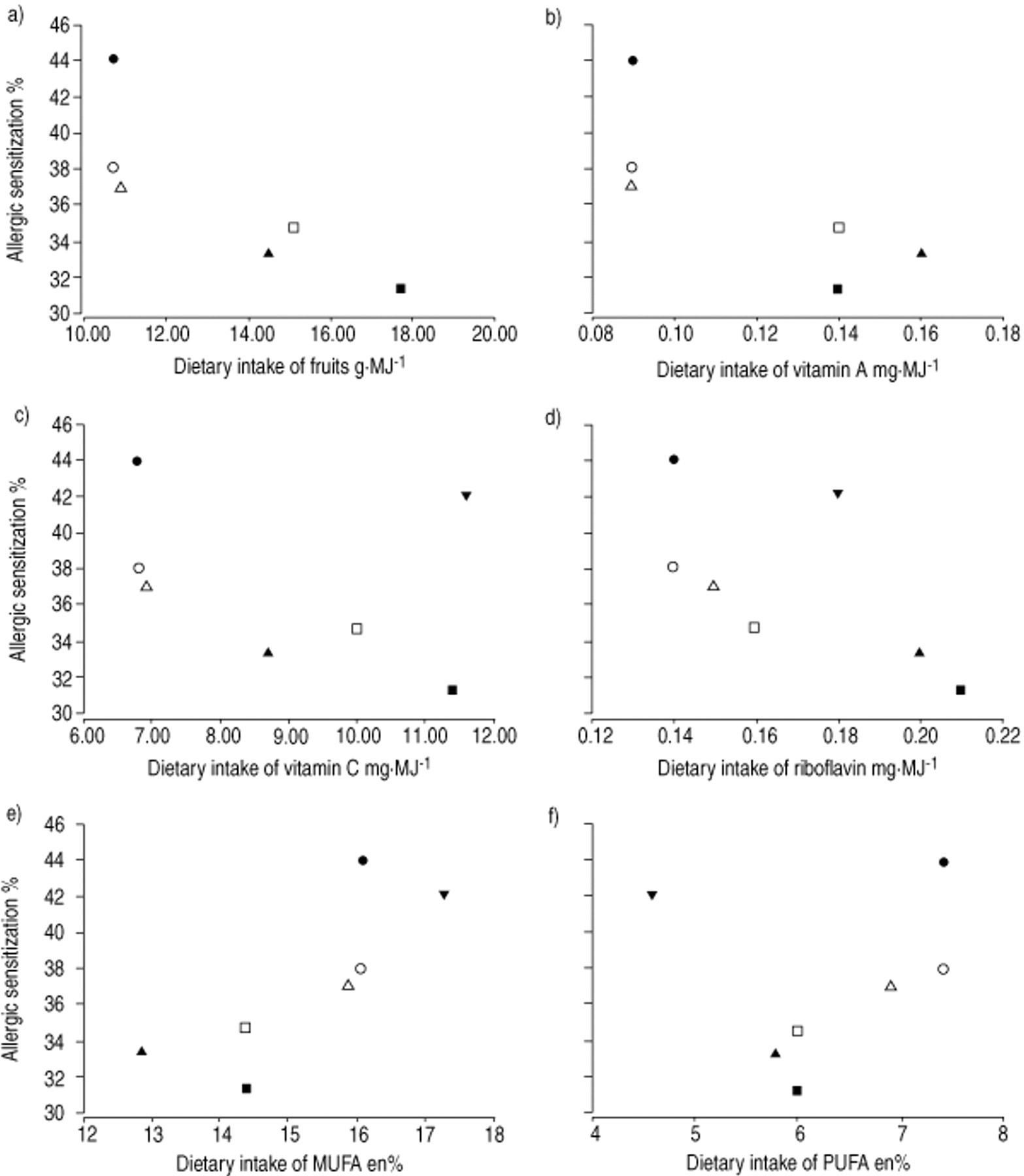
In figure 1⇓, the mean daily intake of fruit, antioxidative vitamins A and C, and riboflavin were plotted against the prevalence of allergic sensitization. Generally, the range of intake for these antioxidative dietary constituents was rather low; the highest coefficient of variation was observed for the intake of fruits. Overall, there was a tendency towards decreasing sensitization prevalence with higher intakes of fruit and of vitamin A and C. For dietary intake of vitamin A two clusters were seen, one cluster contained the Dutch centres and a second cluster included the remaining centre's. Riboflavin intake also showed a weak inverse relationship with allergic sensitization. The intake of fruit was inversely and statistically significant associated with theprevalence of allergic sensitization (OR=0.68, p=0.034). The intake of vegetables, however, did not show an association (table 3⇓). Although the OR for all the vitamins considered in this analysis were also consistently <1, the confidence intervals (CI) included the value of one (table 3⇓).
{kind=link}
Association between energy adjusted mean dietary intake of a) fruit, b) vitamin A, c) vitamin C, d) riboflavin, e) monounsaturated fatty acids (MUFA), f) polyunsaturated fatty acids (PUFA) and allergic sensitization (RAST) among adults from 6 to 7 European county centres. •: Geleen; ○: Bergen-op-Zoom; ▵: Groningen; □: Erfurt; ▴: Uppsala; ▪: Montpellier; ▾: Barcelona.
Association between the mean daily intake of selected dietary constituents and the prevalence of allergic sensitization
Fatty acids
Dietary intakes of energy adjusted MUFA and PUFA were positively related to the prevalence of allergic sensitization (fig. 1⇑). Results of logistic regression analyses of the fatty acids reached statistical significance only for MUFA intake (OR=1.55, p=0.035). Fish intake was not correlated with prevalence of allergic sensitization.
Discussion
This ecological study compared the prevalence of allergic sensitization and mean daily intake of selected dietary constituents at 5–8 ECHRS centres distributed throughout Europe. The assumption that the mean food and nutrient intake assessed by 1–7 day dietary records or recall in a random sample of people (with exceptions of the samples from Montpellier and Uppsala) are valid measures of food consumption for another sample of residents from the same area was made. It was also assumed that current diet is a good indicator for past diet and thus relevant for the prevalence of allergic sensitization, although it was not known how many years ago study participants had become sensitised. Inverse associations were found between the prevalence of allergic sensitization and the intake of fruit (OR=0.68, p=0.034). For vitamin A (OR=0.73, p=0.057), vitamin C (OR=0.83, p=0.338), and riboflavin (OR=0.72, p=0.077) the OR were also consistently <1, but confidence intervals included the null value. The energy adjusted daily intake of MUFA was positively associated with sensitization prevalence (OR=1.59, p=0.035). The low or moderate intake of fish in five of the six centres might aggravate to identify an inverse association with prevalence of allergic sensitization. Several studies have reported protective effects of fish oil. For example, fish oil was found to be protective in asthmatic children 14, 28 and improve the lung function of adults in the National Health and Nutrition Survey (NHANES) I study 13.
For this evaluation of associations between diet and allergic sensitization, it is important to note that only 5–8 data points were available. The results, however, remained stable when any single point was left out. Furthermore three of the 5–8 data samples were collected in the Netherlands and the same food consumption data were used for two centres (Geleen, Bergenop-Zoom). Although food consumption is similar in two of the three Dutch study areas, the prevalence of allergic sensitization is not. The inclusion of the three Dutch study centres increased the heterogeneity of prevalence of allergic sensitization. However, if either one of the three Dutch study centres were left out, the results remained stable. No information on further potential confounding factors was available. Therefore, the findings have to be interpreted very carefully. Since the intake of fruit and the antioxidant vitamins A and C were highly correlated, the results (OR<1) showed internal consistency. The calculated p‐values should be considered as descriptive measures.
Data from NHANES I suggested an inverse association between serum vitamin C and the prevalence of wheezing, but not for vitamin C 29. Diminished lung function was observed in random samples of the UK population for subjects who consumed low levels of fresh fruit 30 and for participants in NHANES I who were found to have a low intake of vitamin C 29. A large cross-sectional study conducted in China found that forced expiratory volume in one second (FEV1) increased by 21.6 mL (95% CI −0.4–43.5) and forced vital capacity (FVC) by 24.9 mL (95% CI 0.2–49.6) for every 100 mg·day−1 increase in intake of vitamin C 31. A cross-sectional study of 6,555 Dutch adults found a higher FEV1 and FVC in subjects with a high intake of vitamin C(>90th percentile) compared to subjects with low intake (<l0th percentile) 32. Similar results were obtained for beta-carotene, but not for vitamin E 32. Britton et al. (1995) 33 confirmed the adverse effects of low vitamin C intake on lung function in a cohort study. The Nurses Health Study, however, failed to find associations between vitamin C intake and the incidence of asthma 12. A possible explanation for this discrepancy may be the use of vitamin supplements, especially in symptomatic subjects prior to the diagnosis of asthma, that could lead to misclassification attenuating the association between dietary intake of vitamin C and the development of asthma. The Nurses Health Study also showed a modest protective effect of vitamin E 12, whereas a Dutch prospective cohort study did not show any association between vitamin E intake and CNSLD 11. Data is scarce for additional antioxidants such as vitamin B6 and selenium 10.
An ecological study using data from the International Study of Asthma and Allergies in Childhood 3 and the TRANSFAIR study 34 showed a positive association between the intake of trans-fatty acids and the prevalence of asthma symptoms, allergic rhinoconjunctivitis, and atopic eczema in children aged 13–14 yrs 35. Comparing the results of the two cross-sectional studies conducted in 1991–1992 and 1995–1996 in schoolchildren aged 9–11 yrs in East Germany, von Mutius et al. 36 demonstrated a positive association between margarine consumption and prevalence of hay fever, and an inverse association between butter consumption and prevalence of hay fever and atopic sensitization. Yu and Bjorksten 37 compared the composition of PUFA in serum phospholipids of 22 allergic children against 23 nonatopic controls. They proposed that a disturbance of the metabolism of omega‐3 long-chain PUFA is associated with allergy instead of an impaired delta‐6‐desaturase activity. There is one prospective cohort study that supports to some extent the association of fat intake and development of allergy 38. Low levels of alpha-linolenic acid and imbalanced relationships between omega‐3 fatty acids and omega‐6 fatty acids particularly in mature milk appeared to be associated with atopic sensitization in infancy 28.
Although the main sources of MUFA in the German diet are animal derived products such as sausages and butter, plant oils and margarine contribute a considerable amount of additional MUFA 39. Consequently, the results for MUFA intake are not comparable with the previous association reported for butter or margarine consumption and prevalence of hay fever and allergic sensitization 36.
Strengths of this study include the use of prevalence data on allergic sensitization assessed using highly standardised methods and comparable local dietary information, obtained with individual-based methods. Although results of ecological studies should be interpreted cautiously, this study design has some advantages. For example, the range of variation in dietary intake among populations of different European countries is larger than dietary variation in one location. Furthermore, regional differences might be more stable over time. Regional dietary data for adults provides a good measure of historical and spatial variability of average life-time nutrition. A limitation of this ecological study design is potential confounding by regional factors other than diet. Recent publications suggested that healthy gut microflora may protect against the development of allergic sensitization 40, 41. Whether and to what extent regional food consumption affects intestinal flora needs to be further investigated. Certainly, stronger study designs such as prospective cohort studies are needed to confirm the relationships suggested by the present ecological study.
The findings are in accordance with the hypotheses that a high intake of antioxidants might be protective and that a high intake of monounsaturated fatty acids might promote the development of allergic sensitization.
Acknowledgments
The study could only be carried out with the kind co-operation of many scientists. The authors gratefully acknowledge the contribution and help of the following colleagues who forwarded information on dietary surveys and dietary data or forwarded the names of contact persons: G. De Backer (Gent, Belgium); W. Becker (Uppsala, Sweden); S. Bingham (Cambridge, UK); A. Chrisholm (Dunedin, New Zealand); P. Ducimetiere (Paris, France); I. Elmadfa (Wien, Austria); M. Ferrario (Milan, Italy); A. Ferro-Luzzi (Roma, Italy); M. Gerber (Montpellier, France); M.J.Gibney and S. Foley (Dublin, Ireland); S. Hercberg (Paris, France); K. Hulshof (Zeist, the Netherlands); K.I. Klepp (Oslo, Norway); G. Lloveras i Valles (Barcelona, Spain); W.Kübler and K.J. Moch (Gieben, Germany); D. Kromhout and M. Ocke (Bilthoven, the Netherlands); D. Malvy (Bordeaux, France); A. Martinez (Pamplona, Spain); O. Moreiras (Madrid, Spain); P. Pietinen (Helsinki, Finland); A. Robertson (Copenhagen, Denmark); M. Saava (Tallin, Estonia); P.S. Shetty (London, UK); L. Steingrimsdottir (Reykjavik, Iceland); A. Trichopoulous (Athens, Greece). The authors would like to thank B. Ritz for critical reading of the manuscript.
- Received February 1, 2000.
- Accepted May 28, 2000.
- © ERS Journals Ltd