





Abstract
Noneosinophilic asthma is increasingly recognised as an important clinical–pathological phenotype in adults. However, this entity has scarcely been investigated in children. In particular, it is unknown whether airway remodelling would develop in children with non-eosinophilic asthma to the same degree as in children with eosinophilic disease.
We analysed bronchial biopsies from 80 children undergoing bronchoscopy for appropriate clinical indications: 21 with noneosinophilic asthma, 34 with eosinophilic asthma and 25 control children. Features of airway remodelling – basement membrane thickening, epithelial loss and angiogenesis – and immune activation – inflammatory infiltrate, interleukin (IL)-4, IL-5, transforming growth factor (TGF)-β, TGF-β receptor type II – were quantified by histology and immunohistochemistry.
The main components of airway remodelling were present in children with noneosinophilic asthma just as in those with eosinophilic disease. Indeed, compared with control children, both noneosinophilic and eosinophilic asthmatic children had thickened basement membrane, increased epithelial loss and higher number of vessels. Moreover, in both groups of asthmatics, expression of IL-4 and IL-5 was increased, while that of TGF-β receptor type II was reduced, compared with controls.
This study demonstrates that structural changes typical of asthma develop in asthmatic children even in the absence of a prominent eosinophilic infiltrate, indicating that other mechanisms, besides eosinophilic inflammation, may promote airway remodelling early in life.
Bronchial asthma has become an increasing public health concern, especially in industrialised countries. The prevalence of asthma has increased significantly over the past 20 yrs and its incidence has become particularly high in children [1, 2]. It is now widely accepted that childhood asthma is more complex than previously recognised, with distinct phenotypes that may differ significantly in terms of aetiology, pathophysiology and clinical outcomes [3–5].
Eosinophils have long been credited with a central role in asthma. Indeed, the pathology of asthma is characterised by a chronic inflammation of the airways, comprising increased numbers of eosinophils, mast cells and T-lymphocytes. This pro-inflammatory milieu is modulated via T-helper (Th)2 mechanisms (involving interleukin (IL)-4 and IL-5), but recent evidence suggests that other subsets of lymphocytes may be important, such as Th17 and Th9, whose activation depends on transforming growth factor (TGF)-β signalling [6]. Furthermore, the inflammatory reaction is associated with structural changes of the bronchial wall. These changes, collectively termed “airway remodelling”, include epithelial loss, basement membrane thickening, smooth muscle increase and angiogenesis.
The relationship between eosinophilic inflammation and airway remodelling is not completely understood; traditionally, remodelling has been considered the unavoidable consequence of long-term airway inflammation. However, the first studies that evaluated the pathology of asthma in children showed that both airway eosinophilia and all the structural changes characteristic of asthma were present in children, even at pre-school age [7–11]. These results indicate that the processes leading to remodelling of the airway wall begin early in the course of the disease and most probably occur in parallel with the establishment of chronic inflammation rather than subsequently to it.
Moreover, most studies that have provided direct evidence for eosinophils as effectors of tissue remodelling were performed in animal models [12, 13]. Evidence that eosinophils are required for development of airway remodelling is less compelling in humans and, more importantly, it is now well established that human asthma does not necessarily imply eosinophilic inflammation. Indeed, although asthmatics have median eosinophil counts higher than controls, a significant proportion of patients shows no evidence of eosinophilia, despite having all symptoms and functional alterations typical of asthma [14–16].
The issue of noneosinophilic asthma was first raised in patients with severe disease [17], but there is now more comprehensive information, using induced sputum, that the noneosinophilic phenotype is rather common among patients with asthma, not only in those with severe, but also in those with milder forms of the disease [14–16].
As far as we know, it has never been investigated whether the eosinophilic and noneosinophilic patterns of inflammation are associated with different characteristics of airway remodelling in children. Hence, the aim of this study was to investigate the pattern of structural changes (epithelial loss, basement membrane thickening and angiogenesis) and cytokines (IL-4, IL-5, TGF-β and its type II receptor) in children with noneosinophilic asthma, comparing the results to those of children with the eosinophilic form of the disease and control children without asthma.
METHODS
Subjects
80 children undergoing fibreoptic bronchoscopy for appropriate clinical indications were recruited in this study: 55 had symptoms of asthma, while 25 did not have these symptoms and were included as controls. Children were defined as having asthma when they had repeated episodes of wheezing, breathlessness and cough, particularly at night and early in the morning, that were present even when the child did not have a cold. Moreover, in all asthmatic children, symptoms had to be responsive to bronchodilators. Presence and reversibility of episodic symptoms were assessed by a specific questionnaire administered to parents investigating the pattern of symptoms and the clinical benefit of bronchodilators (symptom resolution or significant improvement). This information was confirmed by the child's paediatrician [7, 10].
Asthmatic children were then categorised as eosinophilic or noneosinophilic according to a threshold corresponding to the 90th percentile of the distribution of biopsy eosinophils in controls (28 cells·mm−2; fig. 1). Based on this partitioning, in our population of asthmatic children, 34 had eosinophilic asthma (62%) and 21 had noneosinophilic asthma (38%).

Individual values for eosinophils in bronchial biopsies in asthmatic and control children. ––––––: median values; ---------: 90th percentile of eosinophil values in controls (28 cells·mm−2), used to subgroup asthmatics as noneosinophilic and eosinophilic. #: p<0.0001.
Children with eosinophilic asthma underwent bronchoscopy for recurrent pneumonia (n=19), chronic cough (n=10), stridor (n=1), difficult asthma (n=3) or middle lobe syndrome (n=1); children with noneosinophilic asthma underwent bronchoscopy for recurrent pneumonia (n=11), chronic cough (n=7), stridor (n=1), difficult asthma (n=1) or obstructive sleep apnoea syndrome (n=1) and control children underwent bronchoscopy for recurrent pneumonia (n=12), chronic cough (n=9), stridor (n=3) or laryngomalacia (n=1).
On the basis of the intensity of treatment required to control symptoms, children were considered to have mild, moderate or severe disease [1]. 36 out of 55 asthmatic children had mild asthma and were treated with inhaled salbutamol only when needed. 15 out of 55 asthmatic children had moderate asthma (treated with equivalent daily doses of beclomethasone ranging 200–400 μg) and the remaining four out of 55 had severe asthma (equivalent daily doses of beclomethasone ≥800 μg). None of the children were being treated with oral corticosteroids or antibiotics at the time of fibreoptic bronchoscopy. The distribution of mild, moderate and severe asthma was similar in the eosinophilic and noneosinophilic groups. In particular, mild asthma was present in 20 (59%) out of 34 children with eosinophilic asthma and 12 (57%) out of 21 children with noneosinophilic asthma. Moderate asthma was present in 11 (33%) children with eosinophilic asthma and in eight (38%) with noneosinophilic asthma. Severe asthma was present in three (8%) children with eosinophilic asthma and in one (5%) child with noneosinophilic asthma.
The presence of atopy was defined by an increase in total (paper radioimmunosorbent test) or specific (radioallergosorbent test) immunoglobulin (Ig)E. In particular, specific IgE for all the following aeroallergens were investigated in all children: house dust mite (Dermatophagoides pteronyssinus and Dermatophagoides farinae), moulds (Alternaria alternate), cat dander and grass pollens (Lolium perenne, Poa pratensis, Phleum pratense, Dactylis glomerata and Cynodon dactylon). Control children were nonatopic.
The prevalence of atopy was similar in children with eosinophilic and noneosinophilic asthma: 56% of children with eosinophilic asthma and 52% of those with noneosinophilic asthma were atopic.
All children underwent routine blood tests, while spirometry was performed only in children who were able to cooperate with the test (n=39). Forced expiratory volume in 1 s (FEV1), forced vital capacity (FVC) and FEV1/FVC were measured using a 10-L bell spirometer (Biomedin, Padua, Italy) and the best of three manoeuvres was expressed as % predicted reference values.
Bronchoscopy with airway biopsies and bronchoalveolar lavage was conducted according to guidelines [18] and written consent was obtained from the children's parents. The study was performed according to the Declaration of Helsinki and was approved by Padua Hospital Ethics Committee (Institutional Review Board approval number 494P). Some of the children examined in the present study had been included in a previous study [10].
Biopsy analysis
Bronchial biopsies were processed as described in the online supplementary material. Analysis of epithelial loss and reticular basement membrane thickness was performed on sections stained with haematoxylin–eosin. Briefly, epithelial loss was quantified by measuring the length of the incomplete epithelium and expressed as a percentage of the total basement membrane length. The thickness of the reticular basement membrane was assessed by taking measurements at 50-μm intervals along all the basement membrane length. Vessels were assessed by immunohistochemistry using a monoclonal anti-CD31 antibody as previously described [8], and expressed as number of vessels per mm2 of examined subepithelium. Analysis of inflammatory cells (eosinophils, neutrophils, mast cells, macrophages, CD4- T-lymphocytes), as well as of IL-4, IL-5, TGF-β and TGF-β receptor type II was performed by immunohistochemistry as previously described [7, 8], and results were expressed as number of positive cells per mm2 of examined subepithelium.
The cases were coded and measurements performed without knowledge of the clinical data. Differences were evaluated using ANOVA and unpaired t-test for clinical data, while the nonparametric Kruskal–Wallis test and Mann–Whitney U-test were applied for morphological data.
Correlation coefficients were calculated using Spearman's rank method.
RESULTS
The bronchoscopy procedure was well tolerated by all children and no complications were encountered. The clinical characteristics of the children studied are shown in table 1. Children with eosinophilic asthma were slightly older than children with noneosinophilic asthma and controls. Importantly, the age at onset of symptoms and symptom duration were not significantly different between the two groups of asthmatics.
FEV1 (% pred), FVC (% pred) and FEV1/FVC did not differ significantly between children with eosinophilic and noneosinophilic asthma. The two groups of children also showed a similar degree of reversibility after bronchodilator administration. Levels of circulating eosinophils and BAL eosinophilic cationic protein were increased in eosinophilic asthmatic children, but not in noneosinophilic asthmatic children, compared with control children.
When we examined the different parameters of airway remodelling, we found that not only children with eosinophilic, but also those with noneosinophilic asthma, had a thickened basement membrane (median 5.4 (range 2.5–11.5) μm and 5.3 (3.8–8.6) μm, respectively, versus 3.1 (1.8–4.9) μm for controls; p<0.0001 versus controls for both), an increased epithelial loss (65 (18–100)% and 50 (12–94)%, respectively, versus 33 (0–100)% for controls; p<0.005 and p<0.05, respectively, versus controls) and an increased number of vessels (259 (9–704) vessels·mm−2 and 250 (0–493) vessels·mm−2, respectively, versus 114 (0–576)vessels·mm−2 for controls; p<0.05 versus controls for both) (fig. 2). Examples of these morphological changes in a child with noneosinophilic and a child with eosinophilic asthma are illustrated in figure 3.
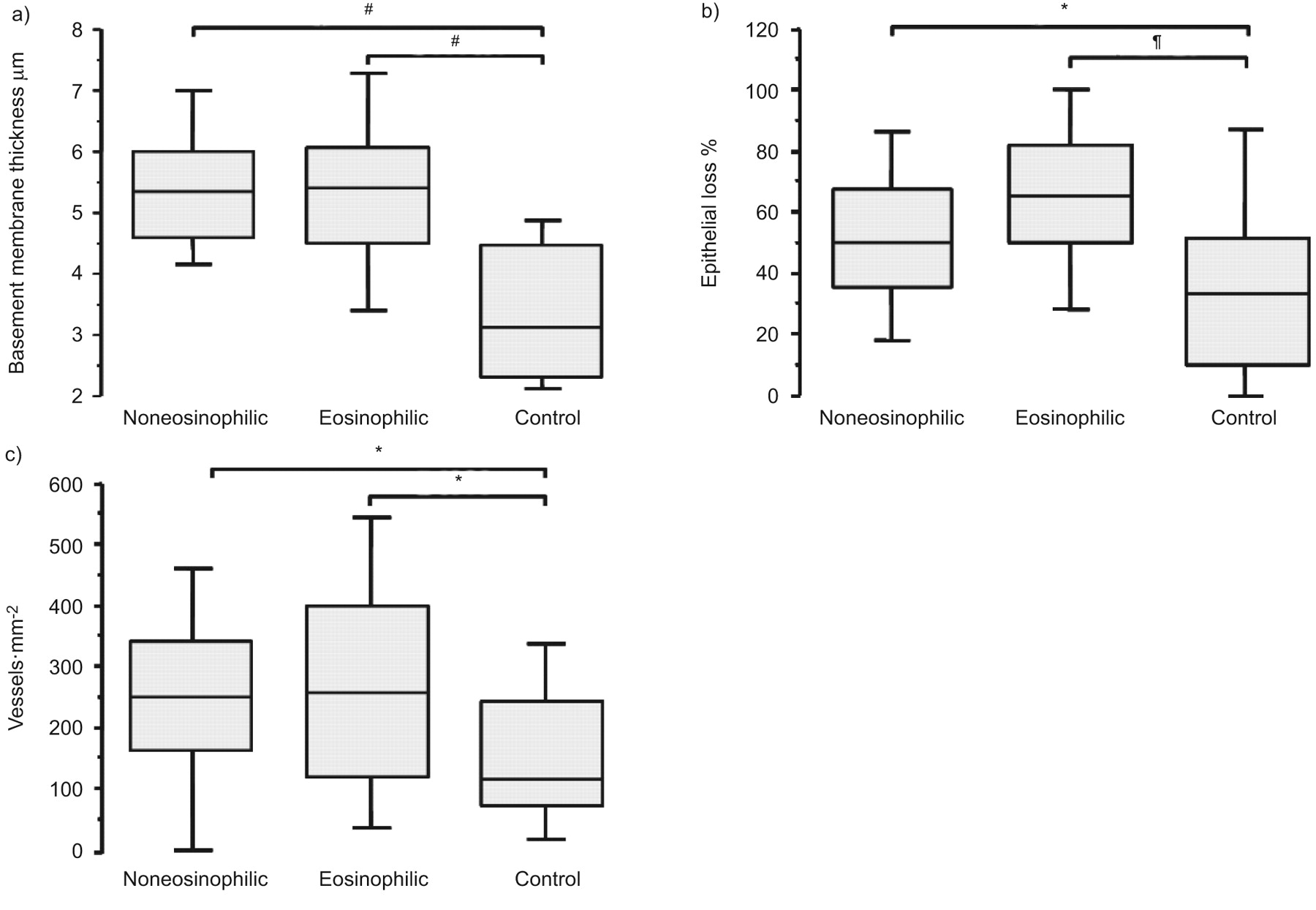
Individual values for a) basement membrane thickness, b) epithelial loss and c) vessels in children with noneosinophilic asthma, children with eosinophilic asthma and control children. The bottom and top of the boxes denote the 25th and 75th percentiles, respectively, the solid line is the median and the brackets are the 10th and 90th percentiles. p-values shown were calculated using the Mann–Whitney U-test; Kruskal–Wallis test p-values were: a) p<0.0001; b) p=0.001; and c) p<0.05. #: p<0.0001; ¶: p<0.005; *: p<0.05.

Bronchial biopsy sections from children with a, c) noneosinophilic asthma and b, d) eosinophilic asthma. a, b) Immunostaining with monoclonal anti-EG2 antibody (eosinophils in red). c, d) Immunostaining with monoclonal anti-CD31 antibody (vessels in brown). Original magnification ×630. Arrowheads: epithelial loss; arrows: reticular basement membrane thickening. Scale bars: 10 μm.
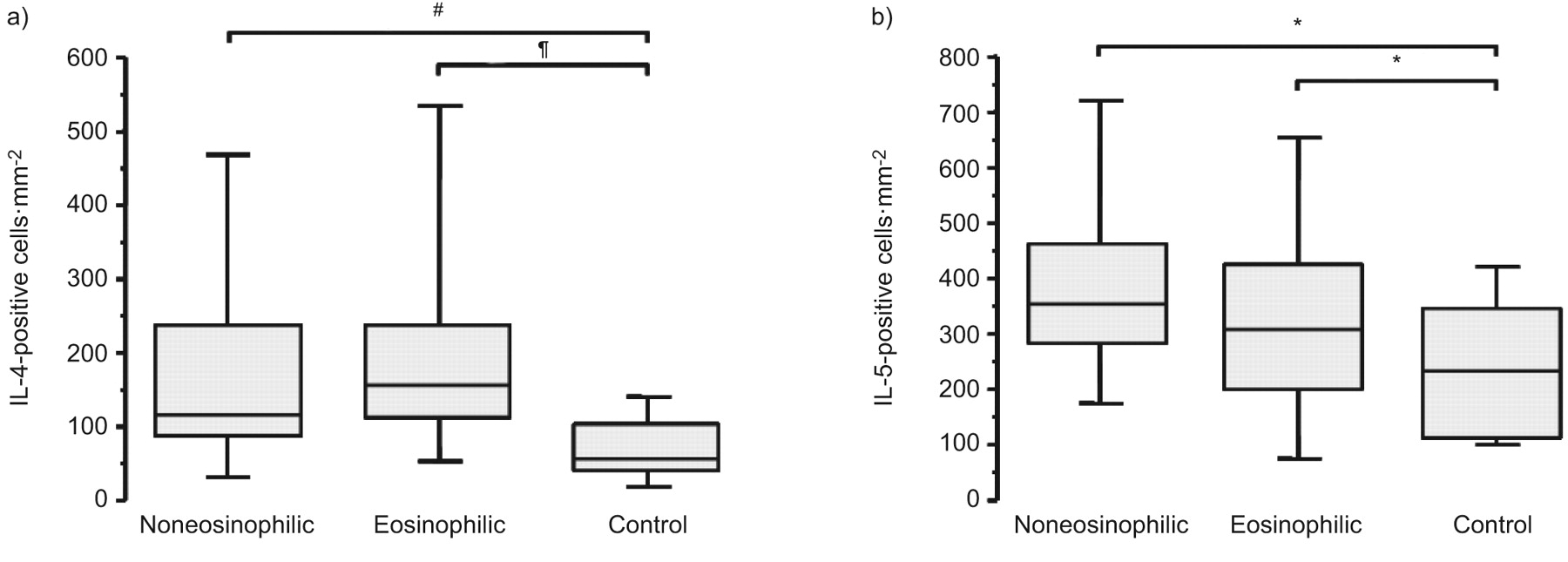
Furthermore, both eosinophilic and noneosinophilic asthmatic children had increased numbers of IL-4-positive cells (156 (0–676) cells·mm−2 and 117 (0–824) cells·mm−2, respectively, versus 56 (8–732) cells·mm−2 for controls; p<0.0001 and p=0.007, respectively, versus controls), as well as IL-5-positive cells (310 (0–834) cells·mm−2 and 356 (0–920) cells·mm−2 versus 235 (0–659) cells·mm−2 for controls; p<0.05 and p=0.007, respectively, versus controls) (fig. 4). No significant difference in the expression of TGF-β was observed among the three groups of subjects examined, but both eosinophilic and noneosinophilic asthmatics had a decreased expression of TGF-β receptor type II compared with controls (48 (0–829) cells·mm−2 and 19 (0–451) cells·mm−2, respectively, versus 160 (0–1,048) cells·mm−2 for controls; p<0.05 for both versus controls) (fig. 5).

Individual values for a) interleukin (IL)-4-positive cells and b) IL-5-positive cells, in children with noneosinophilic asthma, children with eosinophilic asthma and control children. The bottom and top of the boxes denote the 25th and 75th percentiles, respectively, the solid line is the median and the brackets are the 10th and 90th percentiles. p-values shown were calculated using the Mann–Whitney U-test; Kruskal–Wallis test p-values were: a) p=0.0001; and b) p=0.002. #: p=0.007; ¶: p<0.0001; *: p<0.05.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Individual values for: a) transforming growth factor (TGF)-β-positive cells; and b) TGF-β receptor type II (RII)-positive cells in children with noneosinophilic asthma, children with eosinophilic asthma and control children. The bottom and top of the boxes denote the 25th and 75th percentiles, respectively, the solid line is the median and the brackets are the 10th and 90th percentiles. p-values shown were calculated using the Mann–Whitney U-test; the Kruskal–Wallis test p-value for b) was p=0.05. *: p<0.05.
No significant differences were observed among the three groups of children for CD4-positive T-lymphocytes, neutrophils and mast cells, while there was a trend for macrophages to be increased, particularly in children with eosinophilic asthma (table 2).
Since the threshold chosen to identify children with eosinophilic and noneosinophilic asthma was somewhat arbitrary, to validate our results, we decided to compare the two extreme subsets: i.e. asthmatic children within the highest quartile of eosinophils (>140 cells·mm−2) and those within the lowest quartile (<21 cells·mm−2). No significant differences were observed between asthmatic children in the highest quartile and those in the lowest quartile for basement membrane thickness (5.9 (3.5–11.5) μm versus 5.4 (3.8–8.6) μm), epithelial loss (63 (18–100)% versus 50 (20–94)%), vessels (300 (9–620)vessels·mm−2 versus 250 (0–493) vessels·mm−2), IL-4-positive cells (208 (0–676) cells·mm−2 versus 101 (56–451) cells·mm−2), IL-5-positive cells (303 (0–810) cells·mm−2 versus 323 (0–920)cells·mm−2) and TGF-β receptor type II (47 (0–829) cells·mm−2 and 19 (0–451) cells·mm−2). Importantly, versus control children, all the pathological features were present not only in asthmatic subjects in the highest quartile of eosinophils, but also in those in the lowest quartile (except for IL-5-positive cells, which did not reach levels of statistical significance).
Interestingly, in our study, levels of circulating eosinophils paralleled those in bronchial biopsies in the two groups of subjects. In particular, it is worthwhile to note that, among 21 patients considered noneosinophilic based on tissue analysis, none had peripheral eosinophilia (eosinophil counts in peripheral blood >450 mm−3). Conversely, among 34 patients considered to be eosinophilic based on tissue analysis, 14 also had peripheral eosinophilia, while 20 did not. These results indicate that when blood eosinophilia is present, then tissue eosinophilia is to be expected, but low levels of blood eosinophils do not exclude airway eosinophilia. Finally, when we compared subjects with concordant tissue/blood eosinophilia versus discordant tissue/blood eosinophilia, there were no pathological or clinical features able to differentiate the two subsets.
Since asthmatic children included in our study had a broad age range (2–15 yrs), to validate our findings in more homogeneous subgroups, we performed an age-stratified analysis, considering separately children aged <6 yrs (n=49) or ≥6 yrs (n=31). There was no difference in any of the examined parameters (either structural or inflammatory) between asthmatic children of pre-school and school age (see online supplementary material). Moreover, in both age groups, structural and inflammatory parameters were increased in asthmatic children compared with controls, with no differences between the eosinophilic and noneosinophilic forms of the disease (tables 3 and 4). Compared with controls, all trends were confirmed numerically but some of the differences did not reach the levels of statistical significance, probably because of the low number of subjects in each subgroup.
Furthermore, to exclude the potential confounding effect of steroid therapy in some patients, we limited our analysis only to asthmatic children who were not being treated with inhaled corticosteroids (n=36). The main results of our study were confirmed (online supplementary material, table E1). Indeed, even among untreated children, there were no differences in the results pertaining to epithelial loss, basement membrane thickening, angiogenesis or cytokine levels between children with eosinophilic and noneosinophilic asthma.
Since recurrent pneumonia was a frequent indication for bronchoscopy in our study, we performed a subanalysis considering only patients without recurrent pneumonia, and all the main messages were confirmed. Indeed, when we compared children with eosinophilic and noneosinophilic asthma in this population, there were no differences in the results pertaining to epithelial loss, basement membrane thickening or angiogenesis, nor to cytokine levels (online supplementary material, table E2).
Finally, we evaluated possible relationships between morphological and functional parameters characteristic of the disease. When all asthmatics were considered together, the number of eosinophils was not related to parameters of airway remodelling, but it correlated marginally with the number of macrophages (r=0.28, p=0.04), with that of circulating eosinophils (r=0.28, p=0.01), with the expression of IL-4 (r=0.29, p=0.004) and with FEV1/FVC ratio (r=-0.39, p=0.03). Neither epithelial loss, basement membrane thickening nor the number of vessels was related to FEV1/FVC, FVC, FEV1 or bronchodilator reversibility. This lack of correlation was a consistent finding whether we considered all asthmatic children as one group or as eosinophilic and noneosinophilic groups considered separately. Other weak correlations were observed, whose correlation coefficients never exceeded 0.5. These are reported, for completeness, in the online supplementary material.
DISCUSSION
This study investigated, for the first time, airway remodelling in children with noneosinophilic asthma in comparison with the eosinophilic form of the disease, to elucidate the relationship between airway inflammatory and structural changes in the first years of life. Interestingly, it demonstrates that structural changes characteristic of asthma (basement membrane thickening, epithelial loss and angiogenesis) are present not only in children with eosinophilic, but also in those with noneosinophilic asthma. These results do not throw into question the importance of eosinophils as effector cells in asthma, but rather suggest that other pathways may be involved, thus highlighting the complexity of the disease.
Eosinophils have long been credited with a central role in asthma. Indeed, eosinophilia is a known risk factor for the development of respiratory symptoms, and, among asthmatics, it is associated with higher mortality risk, exacerbations and lung function impairment [19–22]. In particular, sputum eosinophilia is associated with lung function decline in asthmatic patients with persistent airflow limitation [23, 24] and, more importantly, eosinophilia is able to predict the subsequent development of persistent airway obstruction among adults with an early onset of symptoms [22]. Similarly, increased sputum and circulating eosinophils are associated with functional impairment even in children with asthma [25].
Based on these observations, it could be hypothesised that the relationship between eosinophils and impaired lung function could be mediated by an effect of these inflammatory cells on airway remodelling. Indeed, eosinophils have the potential to cause damage to the epithelium through the release of basic proteins, lipid mediators and reactive oxygen species. Moreover, they could contribute to remodelling of the airway wall through the release of mediators with fibrogenic activity [26, 27]. However, in our study, structural changes were present in children with noneosinophilic asthma just as in those with eosinophilic disease, and eosinophilic inflammation was not related to any of the components of airway remodelling. These results suggest that the factors promoting airway remodelling are probably different from those controlling airway eosinophilia. Interestingly, not only structural changes, but even the expression of IL-4 and IL-5 were not significantly different between children with eosinophilic and noneosinophilic asthma, indicating that persistence of eosinophils in the tissue is a complex process that goes beyond the upregulation of these Th2 cytokines. It may appear surprising that the expression of IL-4, and particularly IL-5, was upregulated in children with noneosinophilic asthma; however, this is consistent with the idea that some patients never exhibit eosinophilia [28], even in the presence of a pro-eosinophilic milieu.
Indeed, the degree of variability in tissue eosinophil counts in our study was considerable: ∼60% of asthmatic children had eosinophils above the 90th percentile of controls, while 40% had values below this cut-off. These frequencies are in line with those reported in adults with asthma by studies using induced sputum [14–16], suggesting that the partition we used was indeed appropriate. We should acknowledge that the stability of the noneosinophilic phenotype could be questionable. A recent longitudinal study reported that this pattern was fairly stable [29], while others showed a higher degree of variability [30, 31]. Many potential factors could influence variability of cellular counts, with inhaled corticosteroid use and active smoking being the most prevalent [16]. Of note, the influence of smoking can be considered trivial in our study (no active, very low prevalence of second-hand smoking) and a minority of children were being treated with inhaled corticosteroids (only four out of 55 with high doses). Moreover, our results were confirmed even when we excluded treated children from the analysis and when we compared the two extreme subsets for eosinophil distribution, i.e. asthmatic children within the highest quartile to those in the lowest quartile. In fact, the degree of airway remodelling was really the same in asthmatic children with scant eosinophils and in those in whom eosinophilic infiltration was massive.
Overall, as suggested by other observations [32, 33], airway inflammation in asthma seems to be dissociated from functional and structural abnormalities just as in our study inflammation is dissociated from airway remodelling.
Our observations could be relevant in the context of clinical studies testing whether anti-inflammatory therapies would be able to modify the impairment of lung function. For instance, selective removal of eosinophils with a monoclonal antibody against IL-5, though reducing the rate of exacerbations and improving asthma control in patients with refractory eosinophilic asthma, had little effect on functional parameters [34, 35]. Similarly, steroid therapy does not affect lung function impairment in very young children [36, 37], even if it seems to have a slight effect in adults with recent-onset asthma [38], suggesting that childhood asthma is probably different from adult asthma. On the same line, while we found that a thickened basement membrane was present even in children with noneosinophilic asthma, some studies in adults reported thickening only in patients with prominent eosinophilia [39, 40]. These observations again support the concept that phenotypes in childhood asthma represent a different population than in adults. Indeed, the lack of eosinophils in adults with asthma has been associated with increased pulmonary neutrophilia [14–17] while, in our study, there was no evidence of neutrophilia in children with noneosinophilic asthma.
We are well aware that there are diagnostic issues in children, particularly in the youngest ones, because of the multifactorial nature of wheezing [41]. We were very careful when assessing the pattern of symptoms that were not purely virus-induced, but rather multi-trigger, and had to be responsive to bronchodilators. As recently pointed out [41], there is insufficient evidence in the literature on the pathophysiological mechanisms at pre-school age. It is therefore important to highlight that in our study the airway pathology characteristic of asthma was present in children aged <6 yrs just as in the oldest ones, and that airway remodelling occurred both in children with eosinophilic and those with noneosinophilic disease even at pre-school age. Of interest, when we examined TGF-β signalling, which plays important regulatory roles in fetal and postnatal lung development, we observed a reduced expression of the type 2 receptor in both eosinophilic and non-eosinophilic asthma. This observation confirms our previous findings in a different subset of children [7], but its significance remains to be clarified. Since TGF-β signalling may affect the growth of both epithelium and smooth muscle, it is conceivable that alterations in this pathway may interfere with the growth of the lung structure.
There are potential criticisms of our study. We acknowledge that the majority of children underwent bronchoscopy for clinical indications other than asthma (otherwise biopsy sampling in children would not be feasible for ethical reasons), and the presence of concomitant diseases could have influenced the results. However, since these conditions were distributed equally among the three groups of subjects, we are confident that they did not affect the observed differences. Moreover, we should admit that a crucial component of airway remodelling, i.e. the increase in smooth muscle mass, has not been examined in our report. Because bronchial biopsies sample only a small portion of the bronchial wall, analysis of smooth muscle is not always possible and this is particularly true in children because biopsies are quite small. Lack of more refined functional parameters, such as forced oscillatory resistance or specific airway conductance, which could detect subtle changes in upper airway resistance, is also a significant weakness of the present study [42]. Finally, children with non-eosinophilic asthma were not completely devoid of eosinophils, having values marginally higher than controls. However it seems unlikely that the remodelling observed in these subjects was caused by these scanty eosinophils, since all components of airway remodelling were present even in children within the lowest quartile (whose eosinophil values were similar to controls). We should admit that our study gives only a static picture of the inflammation present in airway tissue at a specific time point, and therefore we cannot draw conclusions on the stability of the phenotypes, in particular in relation to exacerbation or remission of symptoms. Noninvasive markers can be evaluated longitudinally; however, analysis of airway biopsies, with all its limitations, gives us the unique opportunity to evaluate the inflammatory pattern exactly in the airway tissue, where structural changes occur.
In conclusion, this study demonstrates that, even among children, a considerable proportion of asthmatics do not have evidence of tissue eosinophilia. Interestingly, the typical airway remodelling is present in children with noneosinophilic asthma just as in those with the eosinophilic form of the disease. These results suggest that structural changes develop early in the airways of children with asthma, and eosinophilic inflammation is not a necessary requirement.
Acknowledgments
The authors thank C.A. Drace (University of Padua, Padua, Italy) for assistance in editing the manuscript.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Support Statement
The present study was funded by the University of Padua, Italian Ministry of Universities and Research and the Italian Society for Paediatric Respiratory Diseases (SIMRI).
Statement of Interest
A statement of interest for M. Saetta can be found at www.erj.ersjournals.com/site/misc/statements.xhtml
- Received October 28, 2010.
- Accepted January 25, 2011.
- ©ERS 2011
REFERENCES










