





Abstract
Recent studies suggest that use of inhaled corticosteroids (ICS) in chronic obstructive pulmonary disease (COPD) may be associated with a higher incidence of pneumonia. However, it is unclear whether COPD subjects on ICS who develop pneumonia have worse outcomes. Therefore, our aim was to examine the association of prior outpatient ICS therapy with mortality in hospitalised COPD subjects with pneumonia.
We included subjects ≥64 yrs of age, hospitalised with pneumonia in US Veterans Affairs hospitals, and assessed the association of ICS exposure with mortality for hospitalised COPD subjects with pneumonia in a covariate-adjusted regression model.
We identified 6,353 subjects with a diagnosis of pneumonia and prior COPD, of whom 38% were on ICS. Mortality was 9% at 30 days and 16% at 90 days. In regression analyses, outpatient ICS therapy was associated with lower mortality at both 30 days (OR 0.76, 95% CI 0.70–0.83), and 90 days (OR 0.80, 95% CI 0.75–0.86).
Outpatient therapy with ICS was associated with a significantly lower 30- and 90-day mortality in hospitalised COPD patients with pneumonia.
Chronic obstructive pulmonary disease (COPD) has a significant morbidity, mortality and cost 1–4. It is estimated that COPD accounts for ∼120,000 deaths annually in the USA and is predicted to become the fourth most important disability-producing illness. The Global Initiative for Chronic Obstructive Lung Disease (GOLD) has recommended specific therapies for patients with COPD according to the severity of illness. Therefore, the GOLD guidelines recommend the addition of inhaled corticosteroids (ICS) to long-acting β-agonists (LABA) for symptomatic patients with severe to very severe COPD (forced expiratory volume in 1 s (FEV1) <50% predicted) and for those with repeated exacerbations 5. ICS have been demonstrated to reduce the overall frequency of exacerbations of COPD and improve quality of life 6, 7. However, ICS use has also been demonstrated to be associated with an increased incidence of pneumonia 8–12. The concern is that pneumonia constitutes the fifth leading cause of death in those aged ≥65 yrs in the USA 13, 14. In addition, episodes of pneumonia occur more often in patients with COPD 12, 15; however, previous studies have shown conflicting results as to whether COPD is associated with higher mortality in patients with pneumonia 8, 16–19. Limited information is available regarding the association of ICS with clinical outcomes in COPD patients that develop pneumonia 9.
Therefore, the objective of the present study was to assess the association of the prior use of outpatient ICS on 30- and 90-day mortality, in a cohort of hospitalised COPD patients with pneumonia.
METHODS
This study was conducted with Department of Veterans Affairs (VA) healthcare use and outpatient pharmacy data from 19 of 22 VA healthcare networks that were collected as part of a larger study of inappropriate prescribing practices in the elderly 20. The Institutional Review Board of the University of Texas Health Science Center at San Antonio, TX, USA evaluated the research protocol and gave it exempt status.
Study population, inclusion and exclusion criteria
We identified all subjects who were hospitalised with pneumonia in a VA facility during financial year (FY)2000 (October 1, 1999–September 30, 2000) with a primary discharge diagnosis of pneumonia (International Classification of Diseases, ninth revision (ICD-9), codes 480.0–483.99 or 485–487.0) or a secondary discharge diagnosis of pneumonia with a primary diagnosis of respiratory failure (ICD-9 code 518.81) or sepsis (ICD-9 code 038.xx), who also had a diagnosis of COPD (490–492,496). Subjects were included in the study if they: 1) were ≥65 yrs of age on the date of hospital presentation; 2) were hospitalized with an ICD-9 discharge diagnosis of pneumonia for >24 h during FY2000; 3) had a pre-existing diagnosis of COPD; 4) had received ≥1 yr of outpatient primary care from the VA prior to admission; and 5) had at least one filled and active prescription at the time of presentation to ensure that subjects were receiving medications from the VA.
We excluded subjects with history of asthma (with a diagnosis ≥1 yr prior to admission) and those who were treated with recent (<90 days prior hospitalisation) outpatient oral corticosteroids. If a subject was admitted to the hospital more than once during the study period, only the first hospitalisation was included in our analysis.
Data
Demographic information (age, sex, race) was obtained from in-patient and outpatient VA healthcare system data. Missing race data were supplemented using self-reported race from the 1999 Large Health Survey of Veterans, a nationally representative survey of VA enrollees (July 1, 1999–January 1, 2000) 21. Race categories included White, Black, Hispanic, and other/unknown. In addition, we utilised information on the VA means test as a surrogate for income, and use of geriatric clinics in the preceding year as a potential indicator of subject frailty.
Comorbid conditions were obtained from in-patient and outpatient records for ≥1 yr prior to the date of hospitalisation. Charlson's comorbidity score was used to develop indicators for pre-existing comorbid conditions 21, 22. Charlson's comorbidity score is based on 19 comorbid conditions, each of which has an associated prognostic weight; the summary measure ranges 1–6.
The primary predictor of interest was use of ICS. Pharmacy data were obtained from the VA's Pharmacy Benefits Management. Subjects were considered current users of a given medication if they had enough doses to last until the date of hospitalisation, assuming an 80% compliance rate.
Medications classified as ICS included triamcinolone, fluticasone, budesonide, beclamethasone and flunisolide. Patients that were receiving any of these ICS (e.g. monotherapy or in combination therapy as ICS/long-acting bronchodilators) were defined as ICS. To further control for potential confounding, each patient's count of unique drugs in each of the following classes was calculated for drugs filled or refilled within 90 days prior to presentation: cardiac medications, respiratory medications (other than ICS) and diabetic medications. Previous research has demonstrated that using the count of these medication classes is preferable to adjusting for the individual medications 23–25.
Outcomes
Our primary outcomes were 30- and 90-day mortality starting on the date of admission 14, 26. Mortality was assessed using the VA's Beneficiary Identification Records Locator Subsystem death file and in-patient portion of the National Patient Care Database. Previous studies have demonstrated that after 1972, this methodology had a sensitivity of ∼96% for veterans' deaths 27.
Statistical analyses
Bivariate statistics were used to test the association of demographic and clinical characteristics with all-cause 30- and 90-day mortality. Categorical variables were analysed using the Chi-squared test, and continuous variables were analysed using an unpaired t-test. Due to the large sample size of this data set, statistical significance was set at p<0.001.
A propensity score technique was used to balance covariates associated with ICS use between groups 28–30. The propensity score was derived from a logistic regression model with ICS use as the dependent variable. We included variables in the propensity score if previous research demonstrated a relationship between a variable and ICS use, or if we hypothesised that it may be related to prescription of the medications. The covariates included in the propensity score models were age, sex, race, marital status, socioeconomic status, classes of medications (cardiac, diabetic, respiratory other than ICS), and the Charlson's comorbidity score. We then created an ordered categorical variable based on a quintile stratification of the propensity score to include in the multilevel models. Our primary analysis employed generalised linear mixed-effect models with the subject's hospital as a random effect. We created separate models, one with 30-day mortality as the dependent variable and another with 90-day mortality, with ICS use and the propensity score as the independent variables. A subanalysis was performed using a similar model, but including the cohort of COPD patients with at least one medication during the same study period for COPD, such as any form of β-agonists, anticholinergics or theophyline, so as to reaffirm the diagnosis as it was validated by Joo et al. 23. We used the Kaplan–Meier to graph the proportion of survivors according to the use of ICS status.
All analyses were performed using STATA 9 (StataCorp, College Station, TX, USA).
RESULTS
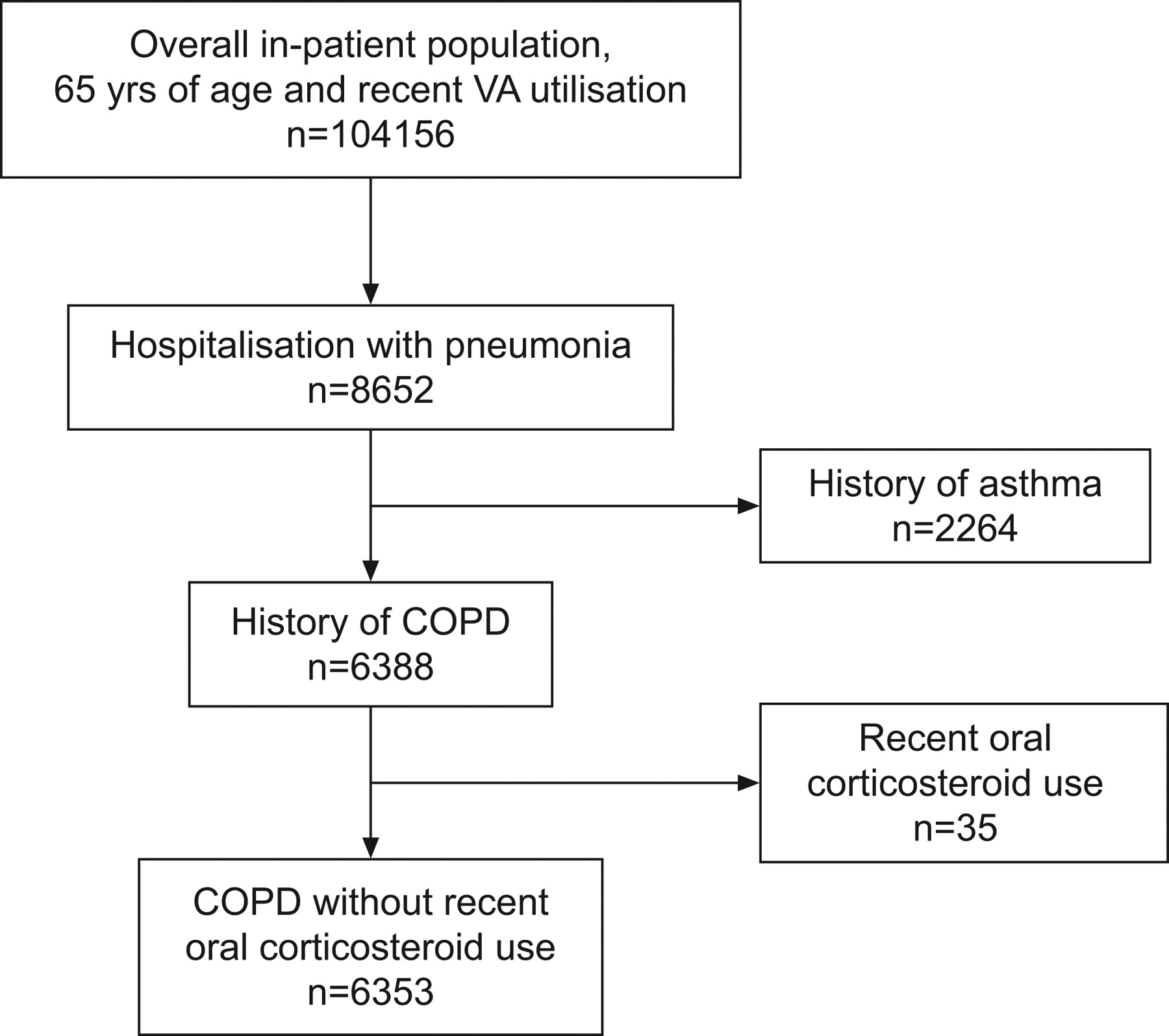
There were 6,353 hospitalised COPD patients with pneumonia who met the inclusion and exclusion criteria (fig. 1). The median±sd age was 74.7±5.8 yrs (range 65–107), and 98% were male. In our cohort, 566 (8.9%) subjects died within 30 days of presentation, and 1,016 (16.0%) died within 90 days of presentation. 2,420 (38.1%) were ICS users and only 29 (0.49%) subjects were on prior outpatient oral corticosteroids. We did not find any statistically significant difference between ICS users and nonusers for oral corticosteroid use.
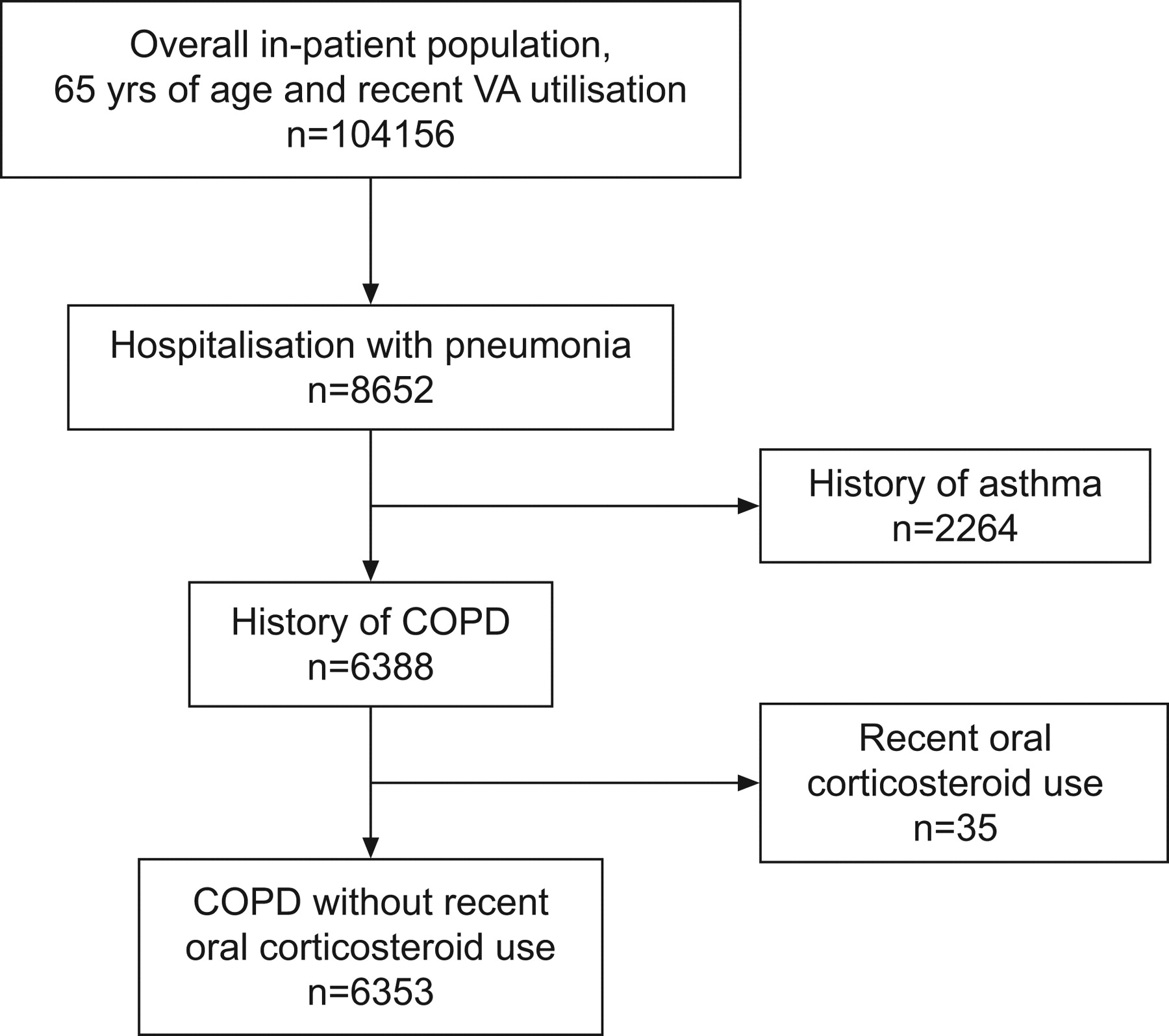
Flow diagram of the cohort selection of hospitalised pneumonia patients with chronic obstructive pulmonary disease (COPD). VA: Dept of Veterans Affairs.
Table 1 shows the demographic factors and clinical characteristics stratified by the use of ICS. Hospitalised COPD patients with pneumonia who were ICS users were more likely to be married. Nonusers were significantly more likely to have complicated diabetes, metastatic cancer, dementia, and renal failure.
Subject characteristics and their relationship with mortality are shown in table 2.
In the bivariate analysis, 30-day mortality was positively associated with metastatic cancer, and negatively associated with diabetes medications and complicated diabetes. Similarly, 90-day mortality was positively associated with metastatic cancer, non-metastatic solid tumour, and dementia, while negatively associated with complicated diabetes.
Figure 2 was created using a Kaplan–Meier curve to graph the baseline survivor functions for ICS use over the first 90 days after admission.

{kind=link}
{kind=link}
Kaplan–Meier curve of the proportion of surviving subjects hospitalised with pneumonia by outpatient inhaled corticosteroid use (—; n = 2,420) versus non-use (---; n = 3,933) (p<0.001).
The crude and adjusted OR for 30- and 90-day mortality in COPD patients hospitalised for pneumonia are shown in table 3. In the generalised linear mixed-effect models, after adjusting for the propensity score and clustering within the admitting hospital, prior outpatient use of ICS was significantly associated with lower 30-day mortality (OR 0.76, 95% CI 0.70–0.83) and 90-day mortality (OR 0.80, 95% CI 0.75–0.86). When we used a case definition of COPD and COPD medications in the subanalysis 23, we obtained similar results with ICS use associated with lower 30-day (OR 0.66, 95% CI 0.52–0.84) and 90-day (OR 0.74, 95% CI 0.61–0.87) mortality.
DISCUSSION
Our primary finding was that hospitalised COPD patients with pneumonia who received prior outpatient ICS had significantly lower 30- and 90-day mortality, after adjusting for potential confounders. Although previous research has demonstrated that ICS use is associated with an increased incidence of pneumonia 8–12, our research suggests that ICS use is not associated with higher mortality from pneumonia, as compared to non-ICS users with COPD and pneumonia (administrative definition, not by pulmonary function tests).
ICS alone or in combination and LABA has been shown to reduce exacerbations and improve quality of life in subjects with COPD when compared to short-acting bronchodilators (placebo) treatment 8. However, five recent studies involving the use of outpatient ICS by subjects with COPD, have shown an increased risk of pneumonia. The Towards a Revolution in COPD Health (TORCH) study 8, which examined the potential benefit of ICS and LABA in reducing COPD mortality, showed that, although there was a significantly increased incidence of pneumonia (p<0.01), there was no significant difference in mortality 8. The study by Kardos et al. 10 randomised 994 subjects with COPD to receive either salmeterol alone or in combination with fluticasone. During follow-up, 23 cases of suspected pneumonia were observed in the combination group as compared with seven in the non-ICS group. There were only two deaths due to pneumonia (one in each group) in that study, limiting the power to assess differences by ICS status. The Investigating New Standards for Prophylaxis in Reduction of Exacerbations (INSPIRE) study, compared the combination of an ICS (fluticasone) and a LABA (salmeterol) versus the long-acting anticholinergic tiotropium 11. The study showed a small but significant increase in pneumonia in the combination group but again, despite this, there was still a mortality reduction in favour of the ICS-treated group 11. Ferguson et al. 31 designed a study to evaluate the effect of the combination of salmeterol with a lower dose of fluticasone (250 μg) and they found a higher risk of pneumonia in the ICS group. In addition to these randomised controlled trials, Ernst et al. 9, using a nested case-control design that included 175,906 COPD subjects, demonstrated an increase in risk of pneumonia with the use of ICS, but no associated higher risk of all-cause mortality. However, when the authors restricted the analysis to patients with pneumonia who died within 30 days of hospitalisation, they identified the following: “an increase of 53% (RR 1.53, 95% CI 1.30–1.80) was seen with current use of ICS, whereas use of higher doses, equivalent to fluticasone at 1,000 µg·day−1 or more, was associated with a 78% increase (RR 1.78, 95% CI 1.33–2.37) in the risk for pneumonia hospitalization followed by death within 30 days” 9. Ernst et al. 9 also showed a higher rate of hospitalisation for pneumonia with the highest doses of ICS, a result that was also suggested by a recent meta-analysis 32.
All these studies suggested an increased incidence of pneumonia, but none of them demonstrate corresponding higher mortality; however, it is possible these studies may have lacked the power to show differences. Similarly, both the TORCH and INSPIRE studies suggested no association with the incidence of pneumonia and overall change in health status assessed by St George's Respiratory Questionnaire 8, 11.
The randomised control studies were limited by the absence of a prospective definition of pneumonia and by the number of cases with pneumonia. Our estimate of a 5 and 7% absolute reduction in the risk of death at 30- and 90-days, respectively, in subjects exposed to ICS is consistent with the risk reduction for all-cause mortality in COPD patients by use of ICS reported in two meta-analyses 33, 34.
There are several possible explanations for our results, including ICS reduction of nonspecific inflammation and a decrease in neutrophil influx into the lungs 35–38. An excessive inflammatory response may have deleterious effects against infection 39. For this reason, we believe, that despite the excess incidence of pneumonia, COPD patients on ICS have lower mortality because of the blunted systemic inflammatory response. In addition, in pneumonia the presence of microorganisms results in increased polymorphonuclear leukocyte migration 40, and several investigators have postulated that excessive neutrophil sequestration in the lung may be a cause of severe lung injury 41, 42. Rello and co-workers 43, 44 suggested that radiological progression in pneumonia, probably resulting from an excessive inflammatory response, is an independent predictor of death. More recently, in a mouse model of lung infection, the investigators demonstrated that inhaled fluticasone propionate reduces the invasion of airway epithelial cells by Streptococcus pneumoniae and Haemophilus influenzae and thus reduces the bacterial load 45. However, a recent ad hoc analysis of the TORCH study concluded that despite the benefits of ICS-containing regimens in COPD management, healthcare providers should remain vigilant regarding the possible development of pneumonia as a complication in COPD patients receiving such therapies. In addition, despite the small number of patients, Crim et al. 46 concluded that pneumonia deaths were not higher in the ICS combination group. There are also published editorials, both for and against, addressing the issues associated with the use of ICS in COPD patients, adding to the debate of this hot topic. However, to our knowledge, our study is the first one to address it from the pneumonia standpoint, instead of the COPD view 47, 48.
There are several limitations to our study. The study was an observational study with a large database analysis, and is subject to the recognised limitations of this area, including confounding by indication. In addition, we carefully assembled our cohort from complete patient-discharge data to avoid ascertainment bias. Our sample was predominantly male due to our use of VA administrative data, and it is unclear whether females may have differential responsiveness to ICS as compared to males. In addition, the inclusion of the ICD-9 code 490 for COPD is overly sensitive, but extensively supported by the literature 49–52. Another difference among groups showed that diabetes with complications was associated with survival at 30 days, which may be due to random error. Also, we were unable to assess factors such as type of ICS used, differences in duration of exposure, in-patient continuation of ICS or dose effect, differences among groups regarding primary or secondary pneumonia, in-hospital or discharge treatment, and other important clinical outcomes (e.g. duration of hospital stay). Unfortunately, due to a VA data stand-down several years ago, the data required to perform this analysis has been deleted. Another consideration of possible bias is the possibility that the lack of information on prior pneumonias in patients with ICS may preclude a potential contraindication of the use of ICS for the treatment of COPD. In addition, we did not have pulmonary function test data on the subjects in this cohort; however, a recent study by Joo et al. 23 demonstrated that 80% of VA subjects with a ICD-9 diagnosis of COPD did have COPD according to pulmonary function tests. In addition, the proportion of COPD patients in each GOLD class utilising medications increased with disease severity 23. Therefore, the proportion of COPD patients in GOLD class 1–2 and 3–4 that received COPD medications was 59 and 91%, respectively 23. Future research in this area will need to take these factors into consideration.
In conclusion, this study showed that outpatient therapy with ICS was associated with a significantly lower 30- and 90-day mortality in hospitalised COPD patients with pneumonia. These results render new perspectives for the safety of ICS and potential future application of ICS as an immunomodulatory therapy of pneumonia. Further study in prospective COPD cohorts is needed.
Footnotes
Support Statement
R. Malo de Molina received funding from the Spanish Pulmonary Society (SEPAR), project 757. M.J. Pugh received funding from the Dept of Veterans Affairs IIR 02-076 and MREP 02-267. L.A. Copeland was supported by the Dept of Veterans Affairs MREP 05-145. M.I. Restrepo is supported by a Dept of Veteran Affairs Veterans Integrated Service Network 17 new faculty grant and National Health Institute KL2 Grant 9CTSA Award Number (KL2 RR025766). This material is the result of work supported with resources and the use of facilities at the South Texas Veterans Health Care System. The funding agencies had no role in conducting the study, or role in the preparation, review, or approval of the manuscript. The views expressed in this article are those of the authors and do not necessarily represent the views of the Department of Veterans Affairs.
Statement of Interest
Statements of interest for M.I. Restrepo and A. Anzueto can be found at www.erj.ersjounals.com/misc/statements.dtl
- Received May 12, 2009.
- Accepted April 4, 2010.
- ©2010 ERS










