





Abstract
It was hypothesised that the time to detect Mycobacterium tuberculosis in liquid culture of sputum from patients with pulmonary tuberculosis may be a better indicator for the duration of respiratory isolation than sputum smear status.
Pre-treatment and during-treatment sputum acid-fast bacilli (AFB) smear and culture results were reviewed in 284 patients with pulmonary tuberculosis. The time to detect M. tuberculosis in liquid culture (TTD-TB) was the number of days from inoculation of the Mycobacterial Growth Indicator Tube to culture detection and visualisation of AFB.
The median (interquartile range) TTD-TB for smear group 0 (no bacilli seen) was 14 (12–20) days. This value was used as the standard at which release from isolation could be permitted. In smear group 4 (>9 AFB per high-power field (hpf) in sputum specimens before treatment) patients, the TTD-TB exceeded 14 days after a median of 25 days of treatment.
The current authors recommend that patients in smear groups 1 and 2 (1–9 AFB per 100 hpf and 1–9 AFB per 10 hpf in sputum specimens before treatment, respectively) receive treatment in respiratory isolation for 7 days, provided the risk of drug resistance is low. Smear group 3 (1–9 AFB per hpf) and 4 patients should receive treatment in respiratory isolation for 14 and 25 days, respectively. These criteria would have reduced the duration of respiratory isolation by 1,516 days in the 143 study participants with sputum smear-positive pulmonary tuberculosis.
Provided clinical and radiographical criteria are satisfactory, use of the time to detect Mycobacterium tuberculosis in liquid culture could enable the duration of respiratory isolation to be predicted from the pre-treatment sputum smear grade. The recommendations enable isolation to end well before sputum becomes smear negative, with considerable benefits to patients and healthcare providers.
- Infectivity
- pulmonary tuberculosis
- respiratory isolation
- time to detect tuberculosis in liquid culture
- transmission
- treatment
Drug treatment of active tuberculosis (TB) is a key factor in interrupting the transmission of this disease. The duration of treatment required to render patients noninfectious varies between individuals and remains largely unknown 1. It is recommended that patients with sputum smear-positive pulmonary TB (PTB) receive initial treatment in respiratory isolation 2–4. Infectivity is closely related to sputum smear status 5–10. Patients with negative sputum smears are not routinely placed in respiratory isolation, even though they may transmit tuberculosis 11. This is because smear-negative cases are less infectious than those who are smear positive 5–8, reflecting the number of viable bacilli expectorated 9, 10. Treatment rapidly reduces colony counts of Mycobacterium tuberculosis in the sputum of patients with PTB 12, 13.
Contemporary liquid culture methods allow for the rapid detection of M. tuberculosis, particularly in highly smear-positive samples. The current authors hypothesised that time to detect M. tuberculosis in liquid culture may be a better indicator for the required duration of respiratory isolation than sputum smear status: after weeks of treatment, smear status alone does not show whether organisms are viable. In the present study, the initial objective was to examine whether time to detect TB in liquid culture (TTD-TB) correlated with smear status; if so, it would provide an indirect indication of the number of viable bacilli in sputum samples. The second objective was to determine the duration of treatment required to reduce the TTD-TB of a patient with positive sputum smears to that of a sputum smear-negative patient, and, by implication, the time at which they could be released from respiratory isolation. The final objective was to estimate the number of days of respiratory isolation that might have been saved if the study population was subject to the new recommendations the current authors devised, based on TTD-TB.
METHODS
The present study was a retrospective, laboratory-based audit. A study proposal was submitted to the Northern New Zealand Health and Disability Ethics Committee (Auckland, New Zealand), who advised that formal ethical approval was not required. The Auckland District Health Board mycobacterial laboratory (Auckland, New Zealand) was the regional reference laboratory. Patients with PTB were identified from its database.
Inclusion and exclusion criteria
To be eligible for inclusion in the present study, patients were required to have had a positive sputum or induced-sputum TB culture between January 1, 2000 and December 31, 2003. To increase uniformity within the principal group analysed (patients with fully susceptible isolates), only patients receiving isoniazid, rifampicin and pyrazinamide, with or without ethambutol, were included. Patients in respiratory isolation were treated with daily therapy and each dose was observed by a nurse. Excluded patients were those whose isolates were resistant to isoniazid, rifampicin or pyrazinamide, who did not receive treatment at the current authors’ hospital, or who were receiving treatment when their first positive specimen arrived in the laboratory.
Laboratory methods
Sputum specimens were processed following standard smear and culture methods 14 in a fully accredited mycobacterial reference laboratory. Microscopy was performed on all specimens, which were also cultured using both Lowenstein–Jensen solid medium (Fort Richard, Auckland, New Zealand) and the BACTEC 960 Mycobacterial Growth Indicator Tube (MGIT; Becton Dickinson, Sparks, MD, USA) broth, used in a BACTEC MGIT 960 incubator. The BACTEC MGIT 960 system is a continuously monitored device. There is neither reader bias nor reading interval bias in identifying a positive culture. Specimens taken before treatment were incubated until culture positive, or for up to 28 days, when they were deemed to be culture negative. Specimens from patients already known to have TB (those receiving treatment) were incubated for 42 days.
Susceptibility testing to first line drugs was performed with the BACTEC MGIT 960 system. Susceptibility to pyrazinamide was further confirmed by the Wayne method 14. M. tuberculosis complex was identified by nucleic acid probe testing (GenProbe, San Diego, CA, USA). The current authors defined TTD-TB as the number of days from inoculation of the MGIT to the detection of positive growth and visualisation of acid-fast bacilli (AFB) in the smear from the positive MGIT broth.
Data collection and sputum sampling
Initial data collected on patients included patient characteristics, start date of culture, date of positive MGIT culture, smear grade 14, TTD-TB of each specimen, isolate drug susceptibility and the number of days patients spent in respiratory isolation. Patients were grouped by their highest pre-treatment smear grade (table 1⇓). All patients had at least two sputum specimens examined before assignment to a group 15. The policy for patients in respiratory isolation was for sputum samples to be collected weekly. Once a sample was smear negative, two further samples were collected on the following 2 days in order to determine whether the patient still required respiratory isolation 2.
Characteristics of study patients with pulmonary tuberculosis
Data analysis
Once patients had been allocated to the appropriate smear group, pre-treatment median TTD-TB and interquartile range (IQR) values were calculated for each group. Culture-negative specimens taken before treatment were assigned a TTD-TB of 29 days: 1 day longer than the incubation period for these specimens. Due to the retrospective study design and performance in a clinical, nonresearch setting, sputum specimens were not obtained at strictly uniform intervals. Thus, specimens taken after starting therapy had to be grouped into 7-day periods. To avoid overestimating treatment effect on TTD-TB, only culture-positive specimens were analysed after treatment had started. For example, in group 2 the median TTD-TB would become 24 days rather than 19 days in the second week of treatment if the culture-negative samples were included in the analysis.
Spearman's correlation coefficient was used to examine the strength of relationships between TTD-TB versus smear grade in pre-treatment specimens, smear grade versus duration of treatment, and TTD-TB versus duration of treatment.
RESULTS
Before treatment, 589 sputum or induced-sputum samples from 284 patients were culture positive for M. tuberculosis. In total, 23 patients were excluded; in 20 cases this was due to drug resistance. Table 1⇑ shows patient characteristics in each smear group and the duration of in-patient respiratory isolation. After exclusion criteria were applied, 648 specimens from 261 patients were analysed to determine pre-treatment TTD-TB values (table 2⇓). Specimens that were smear-negative (patient smear group 0) had a median (IQR) TTD-TB of 14 (12–20) days. In specimens from smear group 4 patients, the median TTD-TB was 5 (4–6) days. An inverse correlation was observed between the TTD-TB and smear grade on specimens collected before treatment had begun (Spearman's correlation coefficient -0.87; p<0.01). As expected, duration of isolation closely followed the time to smear conversion to negative: for the smear group 3 patients the median (IQR) time spent in in-patient isolation was 27 (18–37) days; and for the smear group 4 patients it was 38 (27–53) days. Sputum became smear negative after a median (IQR) of 25 (17–34) days of treatment in group 3, and after 34 (24–51) days in group 4.
Effect of tuberculosis treatment on time to detect drug-susceptible Mycobacterium tuberculosis in liquid culture (TTD-TB)
Table 2⇑ shows the median (IQR) TTD-TB for each smear group by day-ranges that correspond to weeks of anti-tuberculous treatment. For specimens from smear group 1 and 2 patients, median TTD-TB values exceeded 14 days (i.e. that of smear-negative patients before treatment) in the second week of treatment. Analysis of smear groups 1 and 2 were limited by the small proportion of patients who had a positive sputum culture after 7 days of treatment. In these two groups, only 10 out of 36 patients had a culture positive specimen after 7 days of treatment. The median (IQR) TTD-TB for these specimens was 17 (14–22) days. In contrast, 25 (96%) out of 26 smear group 3 patients and all smear group 4 patients had a culture-positive specimen after treatment had started.
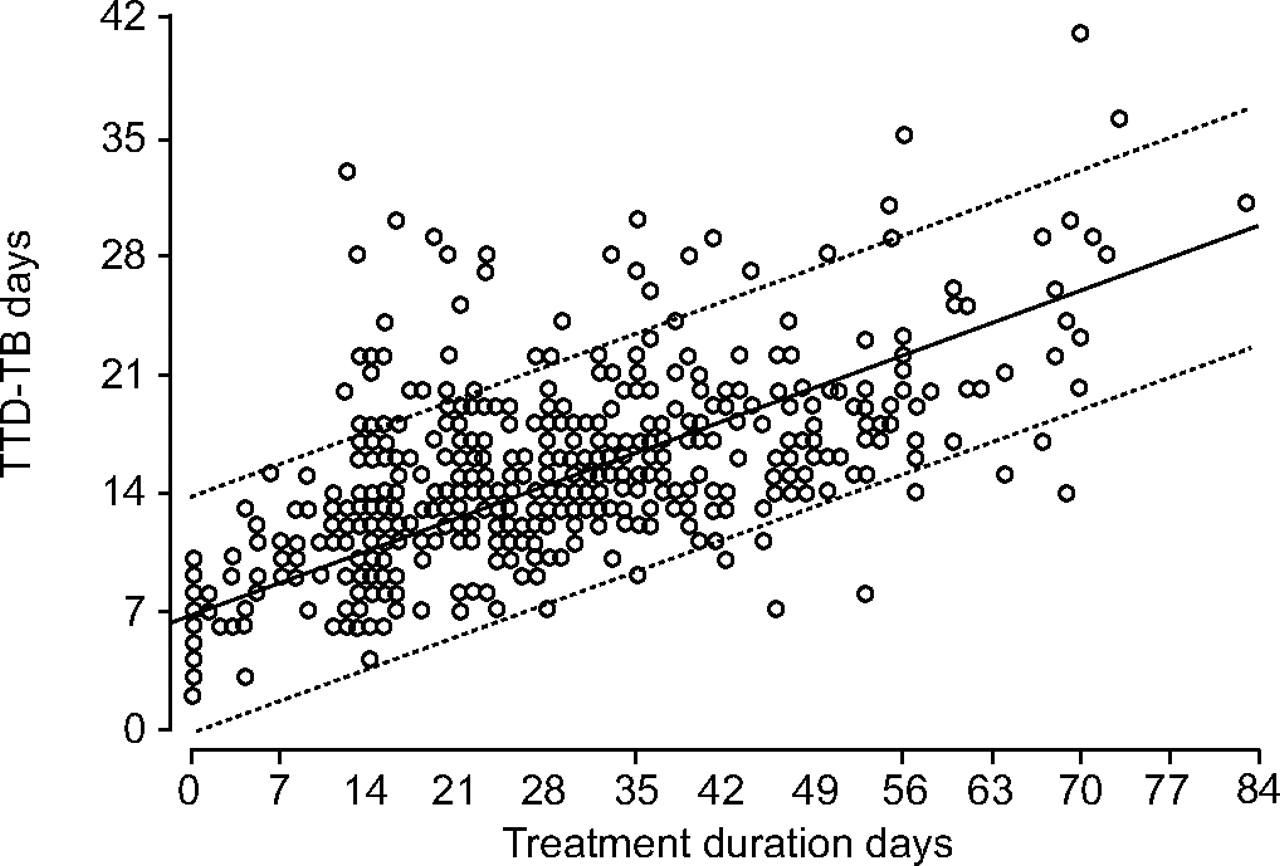
Figures 1⇓ and 2⇓ show the percentage of patients in groups 3 and 4 in whom TTD-TB was ≥14 days by duration of therapy. A patient was only deemed to have a TTD-TB >14 days once the TTD-TB of all subsequent specimens had exceeded 14 days. Before treatment, none of the patients in smear groups 3 or 4 had a TTD-TB ≥14 days. A median (IQR) of 15 (13–23) days of treatment was required before the TTD-TB in specimens from group 3 patients had increased to 14 days. In group 4, 25 (16–33) days of treatment was required to achieve this TTD-TB. There was a stronger correlation between duration of treatment and TTD-TB than sputum smear grade, as shown for smear group 4 patients in figures 3⇓ and 4⇓. Spearman's correlation coefficient for duration of treatment and TTD-TB in specimens from smear group 4 patients was 0.801 (p<0.01), while that for duration of treatment and smear grade was -0.552 (p<0.01).

Duration of treatment and development of time to detect tuberculosis in liquid culture ≥14 days (•) and sputum smear negativity (○) in sputum group 3 patients. p = 0.03 using Wilcoxon signed-rank test.

Duration of treatment and development of time to detect tuberculosis in liquid culture ≥14 days (•) and sputum smear negativity (○) in sputum group 4 patients. p = 0.003 using Wilcoxon signed-rank test.

Sputum smear results versus duration of treatment in smear group 4 patients. Line of best fit (——) and 95% confidence intervals (▒) are shown. Spearman's correlation coefficient for sputum smear and duration of treatment = -0.552 (p<0.01).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time to detect tuberculosis in liquid culture (TTD-TB) versus treatment duration in smear group 4 patients. Line of best fit (——) and 95% confidence intervals (▒) are shown. Spearman's correlation coefficient for TTD-TB and treatment duration = 0.801 (p<0.01).
DISCUSSION
In 2003, New Zealand adopted guidelines similar to those published by the USA Centers for Disease Control and Prevention. The guidelines advocate respiratory isolation for patients with pulmonary TB until appropriate therapy has been established, clinical improvement has occurred and three sputum samples on separate days have become smear negative 2–4. Other authorities recommend isolation for 14 days after starting effective treatment 16. It often takes many weeks for patients with severe PTB to become sputum smear negative. Smears can remain positive long after sputum cultures have become negative, and some patients remain smear positive for many weeks despite a dramatic reduction in viable organisms 9, 17. Thus, there are strong grounds for suspecting that the AFB smear is a poor measure of infectivity after effective treatment has started. Despite this, there has been no recent information to help resolve dissatisfaction with the present guidelines 1, 18.
Although TTD-TB is useful in predicting TB treatment outcome and detecting nonresponders 19, to the current authors’ knowledge it has not previously been used to estimate the time required in respiratory isolation. In the present study, it has been demonstrated that TTB-TB correlates well with pre-treatment sputum smear grade and with duration of treatment. The current authors believe it is logical to end respiratory isolation once the TTD-TB of sputum from smear positive patients has increased to that of smear negative patients. Unfortunately, an individual patient's TTD-TB cannot be used to determine the duration of respiratory isolation due to the delay in obtaining TTD-TB results: these are only known once the cultures become positive. Therefore, group TTD-TB results (with allocation to a particular group based on the highest pre-treatment sputum smear grade) are used in making the recommendations that follow.
New recommendations for the duration of respiratory isolation
The recommendations for patients at low risk of drug resistance or with proven drug susceptible isolates are shown in table 3⇓. Patients were grouped according to clinical indicators and the pre-treatment sputum smear grade. For patients with nonextensive, noncavitatory disease, each group's treatment period required to increase the median TTD-TB to ≥14 days was used to decide when isolation should end. With TB treatment, TTD-TB rapidly increased in smear group 1 and 2 patients to that of smear negative patients who had received no treatment. This is interpreted as showing that it is safe for patients with smear grades 1 and 2 to receive treatment with only 1 week in respiratory isolation, provided the clinical situation is appropriate, and the risk of drug resistance is low. Similarly, group 3 patients could be released from isolation after 14 days of treatment (fig. 1⇑). The results of drug susceptibility testing should be available at this time. A median of 25 days of treatment was required in smear group 4 patients to achieve a TTD-TB ≥14 days. The current authors believe it is reasonable for a group 4 patient with a susceptible isolate and disease which is not severe radiologically, who has improved clinically and is no longer coughing, to be discharged after 25 days of respiratory isolation.
Recommended duration of isolation# for patients with pulmonary tuberculosis at low risk for drug resistance or with known susceptible isolates¶ based on pre-treatment sputum smear grade
Patients with extensive PTB or cavitatory PTB have a greater bacterial load and are more infectious than cases with lesser radiological disease 20. Therefore, it is recommended that a more conservative approach is used in this group. For such cases, it may be appropriate to base the duration of isolation on the duration of treatment required for 90% of the group to achieve a TTD-TB of 14 days. This was 28 days in group 3 and 42 days in group 4 patients (figs 1⇑ and 2⇑). There were eight (31%) out of 26 smear group 3 patients and 17 (21%) out of 81 smear group 4 patients who were considered to have severe disease on radiological or clinical grounds.
Impact of new recommendations for the duration of respiratory isolation: number of days of isolation saved
To measure the reduction in respiratory isolation that would have occurred in the present study population, the duration of hospital stay was compared with the duration of isolation based on the current authors’ new recommendations. Duration of hospital stay was used as a surrogate for total duration of respiratory isolation. However, some patients were isolated at home because they met criteria that made this appropriate 2. Thus, duration of hospital stay underestimates the actual duration of respiratory isolation.
Most patients in the present study would have had significant reductions in respiratory isolation had the current authors’ recommendations been in use, although 26 (18%) out of 143 patients would have required a median (IQR) of 5 (3–7) days extra of isolation. The current authors estimate that 1,516 days of respiratory isolation could have been saved in 143 patients (table 4⇓); even when the patients who would have required a longer duration of isolation are taken into account. The most significant potential for reduction in duration of isolation was found in patients with severe or extensive disease. In smear group 3, 201 days would have been saved in eight such patients, compared with a reduction of only 124 days in the remaining 18 patients. In smear group 4, 424 days would have been saved in 17 patients with severe or extensive disease, compared with 545 days in the remaining 64 patients.
Reduction in the duration of respiratory isolation in patients with sputum smear-positive pulmonary tuberculosis using a newly proposed system based on time to detect tuberculosis in liquid culture data
The main weakness of the present study is that it does not directly address infectivity. The assumption has been made that smear-positive patients (on treatment) who have a TTD-TB of >14 days are no more infectious than smear-negative patients who have the same TTD-TB. The current authors note that the present guidelines make a similar assumption based on sputum smear status 2–4. The validity of the present recommendations for respiratory isolation could be tested by a prospective study that utilises the recommendations and measures the incidence of TB in close contacts of infectious cases.
Of possible concern is the fact that, in the current authors’ model, sputum specimens from many patients would remain culture positive when released from isolation. However, further isolation until sputum smears become negative does not ensure culture conversion 21. Thus, the suspicion is that culture conversion, like smear conversion, is a relatively blunt instrument for determining infectious potential in many cases, and that infectious potential ends before smear and culture conversion. Indeed, previous studies have suggested that most transmission of infection occurs before the diagnosis of TB has been made 22, 23.
Prolonged isolation comes at a considerable cost to individuals as well as to healthcare providers, and the rationale for this has been seriously questioned 1, 18. While the need for three smear-negative sputum specimens before removal from isolation is an appropriate measure for the control of outbreaks of multidrug-resistant TB, its use is questionable in other settings. In the present study it has been shown how TTD-TB could be used to estimate when sputum smear-positive patients will have the same infectious risk as smear-negative, culture-positive patients, provided the isolate is susceptible to standard first-line agents and patients are cough free. TTD-TB can be used to guide the decision about when it is safe to stop respiratory isolation. The current authors recommend that this includes raising the TTD-TB criterion for ending isolation for subjects with initially severe pulmonary disease to the duration of treatment required for 90% of the particular smear group to achieve a TTD-TB of >14 days (rather than median TTD-TB of that group).
In conclusion, the new recommendations are based on clinical indicators and the pre-treatment sputum smear grade. They enable the duration of respiratory isolation to be predicted early in the treatment course (albeit with the caveat that satisfactory clinical and/or radiological improvement occurs). The current authors believe that this approach would considerably reduce the number of days of respiratory isolation. Using time to detect tuberculosis in liquid culture, isolation may end before sputum becomes smear negative, with considerable benefits to patients and healthcare providers.
- Received October 8, 2006.
- Accepted May 9, 2007.
- © ERS Journals Ltd
References










