





Abstract
Numerous studies have been published on single aspects of pulmonary adenocarcinoma (ADC). To comprehensively link clinically relevant ADC characteristics, we evaluated established morphological, diagnostic and predictive biomarkers in 425 resected ADCs.
Morphology was reclassified. Cytokeratin-7, thyroid transcription factor (TTF)1, napsin A, thymidylate synthase and excision repair cross-complementing rodent repair deficiency complementation group-1 expression, anaplastic lymphoma kinase rearrangements as well as epidermal growth factor receptor (EGFR), V-Ki-ras2 Kirsten rat sarcoma viral oncogene homologue (KRAS) and v-Raf murine sarcoma viral oncogene homologue B1 (BRAF) mutations were analysed. All characteristics were correlated with clinical and survival parameters.
Morphological ADC subtypes were significantly associated with smoking history and distinct patterns of diagnostic biomarkers. KRAS mutations were prevalent in male smokers, while EGFR mutations were associated with female sex, nonsmoking and lepidic as well as micropapillary growth patterns. TTF1 expression (hazard ratio (HR) for overall survival 0.61, p=0.021) and BRAF mutations (HR for disease-free survival 2.0, p=0.046) were found to be morphology- and stage-independent predictors of survival in multivariate analysis. Adjuvant radio-/chemotherapy, in some instances, strongly impacted on the prognostic effect of both diagnostic and predictive biomarkers.
Our data draw a comprehensive picture of the prevalence and interplay of established histological and molecular ADC characteristics. These data will help to develop time- and cost-effective diagnostic and treatment algorithms for ADC.
Abstract
Morphological, diagnostic and predictive biomarkers, and clinical characteristics of pulmonary adenocarcinomas http://ow.ly/skRky
Introduction
As the leading cause of cancer related mortality, lung cancer is a major health issue in developed countries [1]. Nonsmall cell lung cancer (NSCLC) accounts for ∼80% of all cases; and ∼60% of NSCLC are adenocarcinomas (ADCs). ADC is a complex, heterogeneous disease showing various clinicopathological and molecular characteristics with significant prognostic and predictive impact [1–10]. In particular, mutations in V-Ki-ras2 Kirsten rat sarcoma viral oncogene homologue (KRAS), epidermal growth factor receptor (EGFR) and v-Raf murine sarcoma viral oncogene homologue B1 (BRAF), and translocations of the anaplastic lymphoma kinase (ALK) gene locus have been identified as oncogenic drivers of ADC with potential predictive value for targeted therapies. Selected patients treated with respective inhibitors have a significantly improved outcome compared with standard chemotherapy [3, 5]. Furthermore, thymidylate synthase (TS) and excision repair cross-complementing rodent repair deficiency complementation group 1 protein (ERCC1) were identified as putative predictive biomarkers for pemetrexed- and platinum-based therapies, respectively [11–14]. Most recently, exome and genome sequences of ADC have been mapped, revealing novel potential therapeutic targets [15, 16], which, however, have mostly not yet entered clinical decision making.
The majority of ADC patients present with inoperable tumour stages at initial diagnosis. Thus, only small biopsies or cytological specimens are available for diagnostic and predictive assessment; in up to a third of all cases, diagnostic immunohistochemistry is additionally required for reliable tumour subtyping [8]. To set up effective patient stratification and reliable treatment strategies in the limited tissue setting, linkage of histomorphological, immunohistochemical, molecular and clinical data is crucial to understand the interplay between all relevant parameters.
In order to comprehensively assess established diagnostic, prognostic and predictive ADC characteristics, their associations with each other and with patient outcome, we retrospectively analysed a Caucasian cohort of 425 subsequently resected ADCs with available clinical data for histomorphology, diagnostic immunomarkers, genetic alterations of KRAS, EGFR, BRAF and ALK, as well as protein expression of TS and ERCC1.
Patients and methods
Patients
Only invasive ADCs surgically resected between 2002 and 2008 with available clinicopathological data were included. Diagnoses and subtyping were made according to the 2004 World Health Organization classification for lung cancer [17] and the novel International Association for the Study of Lung Cancer (IASLC)/American Thoracic Society (ATS)/European Respiratory Society (ERS) classification [18]. The 7th edition Union for International Cancer Control (UICC)/American Joint Committee on Cancer TNM (tumour, node, metastasis) classification was applied. Overall survival and disease-free survival (DFS) were recorded. For DFS, an event was defined as any definite clinical or pathological evidence of local or distant recurrence.
Clinical characteristics
Morphological, immunohistochemical, molecular and clinical datasets were available from 425 cases. Cases with single missing data points were not included in the specific analyses. Nine (2.1%) patients underwent wedge resection, two (0.5%) segmentectomy, 340 (80%) lobectomy, 11 (2.6%) bilobectomy and 63 (14.8%) pneumonectomy, accompanied by systematic lymph node dissection. 264 (62.1%) patients were male. Median (range) age at resection was 62.6 (38.3–84.8) years. 107 (25.2%) patients received adjuvant chemotherapy; 73 (48.7%) stage III/IV patients received adjuvant mediastinal radiotherapy. Adjuvant platinum-based chemotherapy or radiotherapy was administered, unless contraindications were present, according to the guidelines in effect at the time of resection and the clinical status of the patient. None of the patients received biomarker-based targeted therapies. Mean follow-up for patients alive at the end-point of overall survival analysis (n=246, 57.9%) was 48.2 months. Never-smokers were defined as having smoked <100 cigarettes in their lives; former and active smokers were designated as smokers. Clinicopathological characteristics of the patients included in the analyses are given in table 1.
Histomorphological evaluation
All conventional ADCs were subjected to pattern analysis according to the criteria of the IASLC/ATS/ERS classification as described previously in detail [9], recording the percentage of each histological component (lepidic, acinar, solid, papillary and micropapillary) in 5% increments. The predominant pattern was defined as the pattern covering the largest tumour area.
Tissue microarray construction and immunohistochemistry
For immunohistochemical analyses of diagnostic (cytokeratin (CK)7, thyroid transcription factor (TTF)1 and napsin A) and predictive immunomarkers (TS and ERCC1), a tissue microarray (TMA) described previously in detail [8] was used. Use of all tissues was approved by the local ethics committee of the University of Heidelberg, Heidelberg, Germany (No. 206/2005). After haematoxylin- and eosin-based selection of appropriate areas, a TMA machine (ATA 27; AlphaMetrix Biotech, Rödermark, Germany) was used to extract tandem 1.0-mm cylindrical core samples from tissue donor blocks. Immunohistochemical staining was performed by the tissue bank of the National Tumour Centre (Heidelberg, Germany), using commercially available antibodies. All standard routine diagnostic antibodies were applied according to quality-controlled protocols consistently tested in round-robin trials (www.nordiqc.org) and in an accredited setting. TMA slides were deparaffinised and pretreated with an antigen retrieval buffer. Subsequent steps were carried out in a staining machine (DAKO Autostainer; Hamburg, Germany). Expression of diagnostic immunomarkers was evaluated according to a dichotomous scoring scheme [8]. Nuclear and cytoplasmic TS and ERCC1 expression were analysed separately using the H-score (H=1×(% tumour 1 + (weak staining)) + 2×(% tumour 2 + (moderate staining)) + 3×(% tumour 3 + (strong staining))). For overall assessment of TS and ERCC1 expression, the highest nuclear and/or cytoplasmic H-score for the respective marker was noted. For further details on the antibodies used see table S1.
Molecular analyses
All cases were analysed for mutations in KRAS (exon 1), EGFR (exons 18–21) and BRAF (exon 15) by Sanger sequencing. Extraction of genomic DNA was performed after manual microdissection [10] by proteinase K digestion using a fully automated purification system (QIASymphony SP; Qiagen, Hilden, Germany). For reliable sequencing analyses [10], only microdissected tissue material with >40% tumour cell content was used. DNA content was measured using a spectrophotometer (NanoDrop; Thermo Scientific, Wilmington, DE, USA). For PCR amplification the following primers were used. EGFR: 5′-gctgaggtgacccttgtctc-3′ (exon 18 forward), 5′-acagcttgcaaggactctgg-3′ (exon 18 reverse); 5′-gctggtaacatccacccaga-3′ (exon 19 forward), 5′-gagaaaaggtgggcctgag-3′ (exon 19 reverse); 5′-catgtgcccctccttctg-3′ (exon 20 forward), 5′-gatcctggctccttatctcc-3′ (exon 20 reverse); 5′- cagagcttcttcccatgatga-3′ (exon 21 forward), 5′-cctggtgtcaggaaaatgct-3′ (exon 21 reverse); KRAS: 5′-gtgtgacatgttctaatatagtca-3′ (exon 1 forward), 5′-gaatggtcctgcaccagtaa-3′ (exon 1 reverse); BRAF: 5′-cctaaactcttcataatgcttgctc-3′ (exon 15 forward), 5′-ccacaaaatggatccagaca-3′ (exon 15 reverse). Direct sequencing of the PCR amplicons was performed for both strands on a 3500 Genetic Analyzer using the BigDye Terminator v1.1 Cycle Sequencing Kit (both Applied Biosystems, Life Technologies, Carlsbad, CA, USA).
To identify cases with ALK rearrangements, all cases were screened using immunohistochemistry using a sensitive antibody for the detection of ALK-positive NSCLC [19]. Positive cases were subjected to fluorescence in situ hybridisation (FISH) using a break-apart probe (Vysis, Abbott Laboratories, Abbott Park, IL, USA) as described previously [6]. Only cases with FISH-confirmed ALK rearrangement were considered ALK-positive.
Statistics
Correlation of categorical biomarkers with clinicopathological data was performed using Fisher’s exact test, Chi-squared test and Chi-squared test for trends as indicated. Semi-quantitatively evaluated biomarkers (ERCC1 and TS) were compared with clinicopathological data using Mann–Whitney U-tests and Kruskal–Wallis tests. Overall survival and DFS were estimated using the Kaplan–Meier method, with a log-rank test to probe for significance. Hazard ratios (HRs) for univariate and multivariate survival analyses were calculated using the Cox proportional hazard model. All statistical analyses were performed using SPSS Statistics 20 (IBM, Ehningen, Germany). p<0.05 was considered significant.
Results
Distribution of pathological, diagnostic and molecular biomarker characteristics in pulmonary ADC
The final cohort consisted of 416 (97.9%) conventional and nine (2.1%) invasive mucinous ADCs. Of the conventional ADCs, 30 (7.5%) were lepidic, 176 (43.9%) acinar, 21 (5.2%) papillary, 25 (6.2%) micropapillary and 149 (37.2%) solid predominant. In 15 cases, the existing archival tissue was not sufficient for a reliable morphological reclassification.
Concerning the diagnostic biomarkers, 96.7%, 87.6% and 75.5% of ADC cases expressed CK7, TTF1 and napsin A, respectively.
ALK translocations were identified in six (1.4%) cases. KRAS, EGFR and BRAF mutations were detected in 160 (37.6%), 66 (15.5%) and 17 cases (4%), respectively.
Double mutations (mutation 1/mutation 2) occurred as KRAS/KRAS (n=8, 1.9%), EGFR/EGFR (n=6, 1.4%), KRAS/EGFR (n=6, 1.4%) and EGFR/BRAF (n=2, 0.5%). One out of six ALK translocated ADCs showed an additional KRAS mutation. Mean H-scores for ERCC1 and TS were 57.9 and 45.5. For further details on the distribution of clinicopathological characteristics, see table 1.
Association of selected clinical and morphological parameters
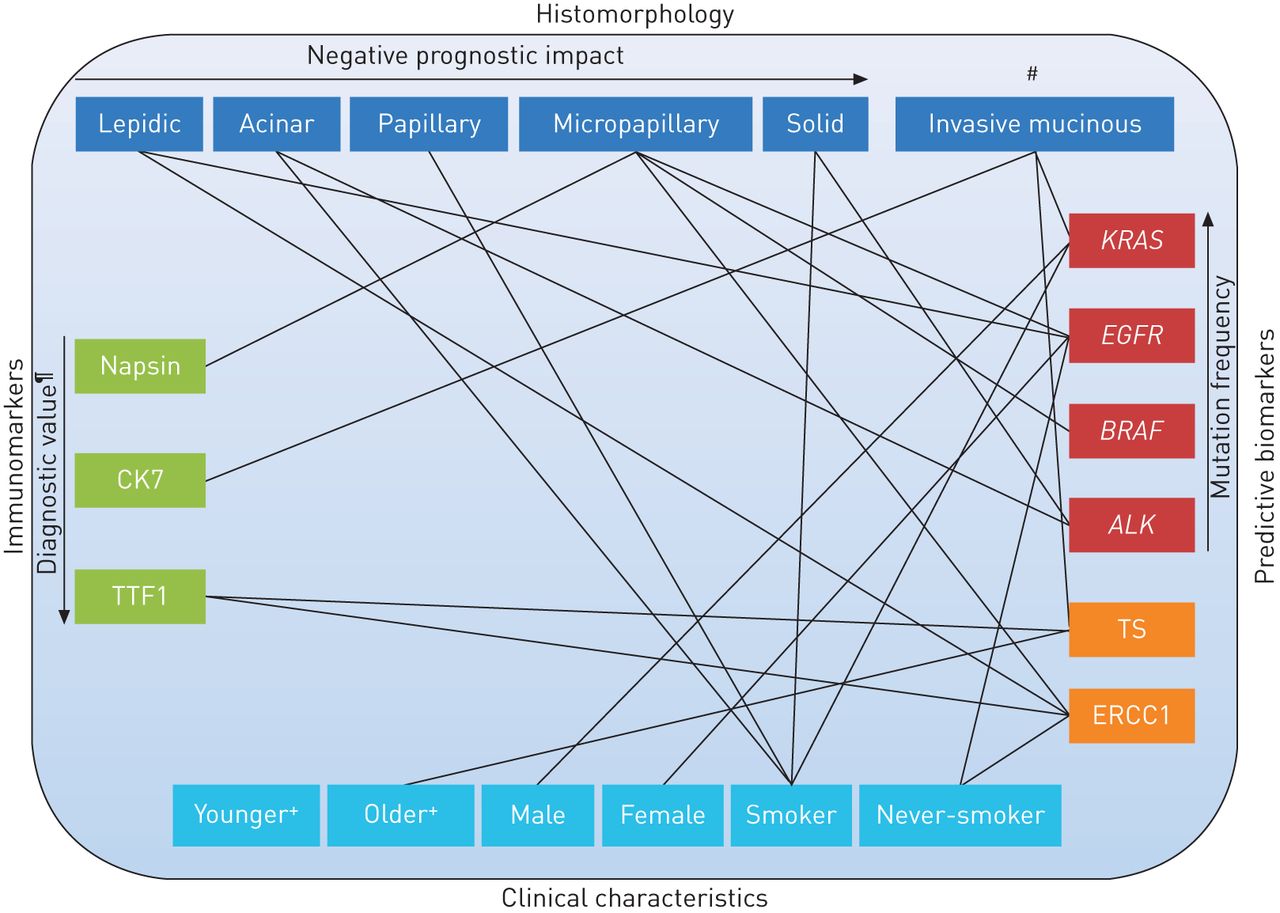
Distribution of UICC stages and TNM classification parameters significantly differed when compared with the dominant growth pattern. Furthermore, predominant histomorphology correlated with smoking status; acinar (91.2% of cases), solid (95.7% of cases) and papillary (89.5% of cases) tumours were significantly more likely to occur in smokers or ex-smokers than lepidic (69.2% of cases) or micropapillary (81% of cases) predominant ADCs (p<0.001). For a comprehensive overview of further findings, compare figure 1 and table 1.

Interplay between clinicopathological variables, and diagnostic and predictive biomarkers in pulmonary adenocarcinoma. Lines indicate a positive association of the respective parameters. CK: cytokeratin; TTF: thyroid transcription factor; KRAS: V-Ki-ras2 Kirsten rat sarcoma viral oncogene homologue; EGFR: epidermal growth factor receptor; BRAF: v-Raf murine sarcoma viral oncogene homologue B1; ALK: anaplastic lymphoma kinase; TS: thymidylate synthase; ERCC1: excision repair cross-complementing rodent repair deficiency complementation group 1 protein. #: prognostic impact to be determined; ¶: compare with Warth et al. [8]; +: patients were classified as being younger or older than the mean.
Association of diagnostic and predictive biomarkers with clinical parameters
Apart from TTF1, whose expression was significantly more prevalent in tumours with low pathological tumour (pT) stages (p=0.035), there were no significant associations of the other diagnostic immunomarkers (CK7 and napsin A) with staging parameters (table 1).
EGFR mutations were significantly more frequent in tumours of female patients, while KRAS mutations were more frequent in males (table 1 and fig. 2). TS expression was significantly higher in tumours of older patients. ERCC1 expression was significantly higher (p=0.023) in tumours associated with smoking history. Of note, smoking history was also associated with higher rates of KRAS mutations (p=0.003) and lower rates of EGFR mutations (p=0.001); the other analysed biomarkers showed no significant association with smoking (table 1).

Distributions of common oncogenic driver mutations according to stage and sex in 425 pulmonary adenocarcinomas. a) Stage I–II total (n=275); b) stage I–II male (n=167); c) stage I–II female (n=108); d) stage III–IV total (n=150); e) stage III–IV male (n=97); stage III–IV female (n=53). KRAS: V-Ki-ras2 Kirsten rat sarcoma viral oncogene homologue; EGFR: epidermal growth factor receptor; BRAF: v-Raf murine sarcoma viral oncogene homologue B1; ALK: anaplastic lymphoma kinase.
ALK translocations and EGFR, KRAS and BRAF mutations were not significantly associated with staging parameters (table 1 and fig. 2).
Association of diagnostic and predictive biomarkers with morphological characteristics
Napsin expression was significantly associated with predominant histomorphological pattern (fig. S1) (p<0.001), with micropapillary carcinomas showing the highest expression rate, while solid and lepidic carcinomas were more likely to be negative. KRAS mutations were more frequent in invasive mucinous ADCs, while no other types of the analysed driver mutations were found in this ADC subtype (table 1). Of all analysed molecular alterations, only EGFR mutation frequency was significantly different with respect to growth pattern, with lepidic and micropapillary predominant ADCs showing higher EGFR mutation rates (table 1), mainly due to differences in the frequency of exon 19 mutations (fig. S2). ALK translocations were exclusively seen in acinar and solid predominant ADCs (fig. S2) and BRAF mutations were predominantly found in micropapillary but not in papillary or lepidic predominant ADCs (table 1 and fig. 1).
Association of diagnostic and predictive biomarkers with each other
Both TS and ERCC1 expression were significantly higher in TTF1-positive ADCs (p=0.026 and p=0.007, respectively) (table 1). Furthermore, higher expression levels of ERCC1 and TS were associated with ALK translocations and wild-type KRAS (ERCC1 p=0.005 and 0.008, respectively, and TS p=0.075 and 0.049, respectively) (fig. S3).
Prognostic value of diagnostic and predictive biomarkers in pulmonary ADC
TTF1 and napsin A expression were associated with prolonged survival with a stronger prognostic value for TTF1 (table 2). Furthermore, TTF1 expression was a stage- and pattern-independent predictor of overall survival (HR 0.61, p=0.021). The survival effect was specifically evident in patients without adjuvant chemotherapy (table S2). TS expression was a significant predictor of better patient survival for overall survival and DFS (table S3 and fig. S4). However, when survival impact of TS expression was adjusted for stage and dominant histomorphological pattern in a Cox regression model, TS failed to show independent impact on patient survival (overall survival HR 0.82, p=0.233 and DFS HR 0.73, p=0.073). The presence of BRAF mutations was a negative prognostic factor for DFS (p=0.009) but not for overall survival (fig. S5). Interestingly, although overall no significant differences in survival were noted, patients with EGFR mutations receiving adjuvant chemotherapy clearly showed an improved outcome compared to patients without such therapy (table S3). A comprehensive overview of the strength of prognostic associations of all morphological, clinical and molecular biomarkers is given in table 2 and in figure 3.

{kind=link}
{kind=link}
{kind=link}
Spider web diagrams depicting the hazard ratios (HR) from univariate survival analysis of the analysed parameters including older age (HR reference: younger age), male sex (female sex), smoker (never-smoker), stages II–IV (stage I), pT2–4 (pT1), pN1–3 (pN0), M1 (M0), acinar, papillary, micropapillary and solid predominant pattern (lepidic predominant), cytokeratin (CK)7-positive (CK7-negative), thyroid transcription factor (TTF)1-negative (TTF1-positive), napsin-negative (napsin-positive), excision repair cross-complementing rodent repair deficiency complementation group 1 protein (ERCC)1-negative (ERCC1-positive), thymidylate synthase (TS)-negative (TS-positive), no anaplastic lymphoma kinase (ALK) translocation (ALK translocation), epidermal growth factor receptor (EGFR) mutation (EGFR wild-type), V-Ki-ras2 Kirsten rat sarcoma viral oncogene homologue (KRAS) mutation (KRAS wild-type) and v-Raf murine sarcoma viral oncogene homologue B1 (BRAF) mutation (BRAF wild-type) for a) overall and b) disease-free survival. *: p<0.05, statistically significant.
Discussion
Although a wealth of details on clinical, morphological and molecular biomarkers in pulmonary ADC has been published, comprehensive studies covering all clinical and pathological characteristics relevant for current routine diagnostic setting are so far lacking. Here, we demonstrate that several specific clinical, histomorphological, immunohistochemical and molecular parameters are tightly linked or occur almost mutually exclusively, which may have significant impact on the development of rational, tissue-sparing diagnostic algorithms as well as an optimised patient stratification.
The past decade in lung cancer research was dominated by large-scale molecular approaches to identify prognostic and predictive markers for personalised medicine. Up to now, however, only EGFR mutations and ALK translocations have been successfully translated into the diagnostic setting; several other potential biomarkers have failed to achieve this goal. Molecular characterisation and subsequent clinical trials underlined that morphological features (e.g. squamous versus nonsquamous) are crucial for therapy selection. Today, it is known that the group of pulmonary ADCs is more heterogeneous than expected, with diverse biological behaviour and prognosis. Therefore, reclassification of ADCs based on histomorphology [18] was a logical and essential step with highly significant prognostic and, probably, predictive value [9]. With this novel and largely reproducible [20, 21] tool, linkage of the different ADC histotypes to diagnostic and predictive biomarkers as well as clinical characteristics is essential for a comprehensive interdisciplinary classification of ADC in the future [18]. Furthermore, different therapeutic targets were found to be associated with each other, implying combined inhibitory strategies for optimised treatment algorithms. For example, ALK translocations were found to be associated with TS expression [22], EGFR mutations were reported more frequently in ERCC1-negative tumours [23] and EGFR inhibitors are known to downregulate TS [24, 25]. Moreover, novel agents like lapatinib, a dual EGFR and Her2 tyrosine kinase inhibitor (TKI), crizotinib (ALK/c-Met inhibitor) or sorafenib (multikinase inhibitor) are directed against more than one target and may thus successfully prevent tumour escape mechanisms. Acquired resistance to targeted therapies is also closely linked to specific molecular alterations [26]. Hence, combined treatment approaches require correlative prevalence data of the respective predictive biomarkers.
ERCC1 and TS are involved in DNA synthesis and repair and their loss of expression was considered as predictive for response to platinum-based [27] and pemetrexed-based [28] chemotherapies, respectively. However, in addition to the potentially negative predictive value of both proteins, high expression levels have also been reported to be associated with an improved outcome [27, 29–31], which was confirmed, at least for TS, by this study. This is explained by the hypothesis that by preventing mutagenesis, DNA repair not only prevents cancer but also inhibits molecular events related to tumour progression. Thus, high expression of the respective markers may indicate an improved outcome in untreated patients by identifying tumours that have only slowly progressed at the molecular level [32], which is also reflected by our finding that high TS and ERCC1 expression levels were more prevalent in early tumour stages (table 1). The association of TS expression with invasive mucinous ADCs, TTF1 positivity, older age and ALK translocations [22], but also the resulting TS downregulation by TKI [24, 25] might be used for the stratification of patients towards combined therapies with pemetrexed.
Several studies have reported the predictive value of ERCC1 for platinum-based chemotherapy, including the International Adjuvant Lung Cancer Trial (IALT) on 761 NSCLC tumours [11]. However, subsequent studies indicate that this association might be specifically prominent in squamous cell carcinoma but not in ADC [33] (A. Warth, personal communication). In our ADC cohort, ERCC1 expression was also associated with reduced survival in those patients receiving adjuvant platinum-based chemotherapy; however, these differences failed to reach statistical significance, which might indicate a comparably small predictive value of this marker but, conversely, might also be attributed to the relatively small sample size in this subcohort. Most recently, Friboulet et al. [34] reported that they were not able to validate the predictive effect of immunostaining for ERCC1 in several large NSCLC cohorts, including the cohort from the IALT trial, which might be due to the fact that commercially available antibodies, including the one used in this study, do not seem to specifically detect the unique functional ERCC1 isoform. Thus, the suggested predictive value of ERCC1 might be disputed until more specific antibodies allow for a validation of the predictive effect of ERCC1 expression.
EGFR mutations have been reported to accumulate in young, female, Asian and never-smoking patients. However, most of the studies published to date reported on selected cohorts in the context of clinical trials. In the herein-analysed unselected Caucasian cohort, we could confirm the predominance of female sex and, in addition, found a higher prevalence in lepidic and micropapillary predominant ADCs. Age was not associated with differences in the prevalence of EGFR mutations. In contrast, others found a higher prevalence of EGFR mutations in older patients and an association to acinar-predominant ADCs [35]. These differences might be explained by different ethnic backgrounds of the respective cohorts. In any case, morphological criteria seem to be helpful if a pre-selection of patients for EGFR mutation testing is desired.
Although no specific targeted therapies exist so far, KRAS mutations are perceived as a potential negative predictive factor for TKI-based ADC treatment and a prognostic factor for surgically resected early-stage ADC [36, 37]. However, there is also evidence that KRAS mutations, which are more prevalent in males, smokers and invasive mucinous ADCs [15, 35, 38] (fig. 2), are not an a priori negative factor for TKI administration [39]. Agents targeting downstream effectors of the KRAS pathway may provide treatment options for this large ADC subgroup. Patient stratification for KRAS mutation testing could be performed based on the above outlined characteristics.
In first trials, BRAF inhibitors showed apparent antitumour activity in NSCLC [40] and specific BRAF mutations also rendered tumours responsive to dasatinib [41]. BRAF mutations were reported to be associated with female sex and smoking. Furthermore, BRAF-mutated tumours have been suggested to belong to an aggressive histotype, characterised by micropapillary features and shorter DFS and overall survival [42, 43]. We could confirm an association of BRAF mutations with micropapillary-predominant ADC and a significant correlation of BRAF mutations with worse DFS, but not the proposed association to female sex or smoking.
Among the diagnostic markers, TTF1 was most recently reported as an independent predictor of survival [44], which was confirmed by our study. Others also described an independent prognostic effect for napsin A and an association of napsin A expression with the presence of EGFR mutations in an Asian ADC cohort [45]. However, we could only see borderline associations of napsin A with survival parameters and no significant association with EGFR mutations. Again, these differing findings might be attributed to differences with respect to ethnic background and underlines the need for reliable prevalence data of large ADC cohorts from various geographical regions.
One limitation of this study is its retrospective nature. The assessment of multiple clinicopathological characteristics necessarily results in small groups for comparison and thus hampers multivariate analyses in some instances. Furthermore, predictive biomarkers are usually not analysed using resection specimens but in advanced tumour stages or recurrent tumours where only sparse tissue is available. Although TMA-based assessment of immunomarkers may largely reflect the biopsy constellation, we cannot exclude a slight prevalence shift of the molecular alterations compared to the daily routine setting.
Considering the growing number of clinically relevant biomarkers, the establishment of not only tissue-sparing diagnostic algorithms but also the development of time- and cost-effective multitesting platforms for molecular alterations with respective implementation into routine diagnostics seems to be mandatory in order to fulfil the requirements of evidence-based decision making within the context of personalised treatment of lung cancer. Novel subgenomic massive parallel sequencing (MPS) strategies, which allow for a comprehensive mutational screen of tumour material in just one sequencing run are especially promising in this regard. However, prior to widespread routine diagnostic use, each of the MPS technologies applied must be adapted to the specific needs in lung cancer diagnosis; specifically, the robustness of the respective methods must be shown on small bronchial biopsy samples and paraffin embedded material.
Taken together, this is the first large-scale study covering in parallel established morphological, diagnostic and predictive biomarkers as well as clinical characteristics of pulmonary ADC. The herein presented data of a largely unselected Caucasian cohort not treated with biomarker-based targeted therapies may form a basis for the development of rational diagnostic stratification algorithms for the selection of appropriate therapies and may also serve as a source of prevalence data for the design of clinical trials.
Acknowledgments
J. Schmitt, A. Brüntgens, C. Hofherr, W. Schmitz, M. Karipidis, M. Viole (Institute for Pathology, Heidelberg, Germany) and C. Stolp (Thoraxklinik Heidelberg, Heidelberg, Germany) are acknowledged for their excellent support of this study.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Support statement: Parts of this study were supported by the LungSys Consortium (grant reference number 0316042B) and a research grant by Novartis.
Conflict of interest: Disclosures can be found alongside the online version of this article at www.erj.ersjournals.com
- Received January 30, 2013.
- Accepted July 10, 2013.
- ©ERS 2014
References










