





Abstract
Cough is one of the commonest reasons for medical consultation and acute cough associated with upper respiratory tract infections (URTIs) is a global problem. In otherwise healthy volunteers complaining of cough associated with symptoms of URTI, we aimed to assess objective and subjective measures of cough and their repeatability and perform power calculations for the design of future studies to test therapies.
We studied 54 otherwise healthy volunteers with acute cough (<3 weeks) (median age 22 yrs (interquartile range 21–26 yrs), 64% female, mean forced expiratory volume in 1 s 97.6±10.5% predicted). All subjects performed 24-h ambulatory cough monitoring and reported cough frequency and severity using visual analogue scales (VAS) on 2 consecutive days. Sample size calculations were performed for crossover and parallel group study designs.
Objective cough frequency was high (session 1: geometric mean 12.1 coughs·h−1 (95%CI 9.7–15.2)) and fell significantly (session 2: 9.0 coughs·h−1 (95%CI 6.9–11.6); p<0.001). Repeatability was higher for objective cough frequency (intra-class correlation coefficient (ICC)=0.94, p<0.001) than reported cough frequency (daytime VAS ICC=0.784, p<0.001). Crossover/parallel studies require <15 and <41 subjects per arm to detect a 50% reduction in cough frequency with 90% power, respectively.
Acute cough frequency is highly repeatable over any 48-h period, allowing small sample sizes to be used when investigating the effectiveness of novel anti-tussives.
Acute cough (<3 weeks duration) is generally caused by viral upper respiratory tract infection (URTI) [1], and cough is the commonest reason for which people seek medical attention [2–4]. On average URTIs affect adults two to four times a year [5–7] and evidence suggests that 93% of cases have an associated cough [8]. Acute cough is a global problem, costing the UK economy an estimated £979 million annually due to loss of productivity, healthcare costs and the purchase of over-the-counter (OTC) medications [9].
The mean duration of cough due to an URTI is 2.4 weeks [8, 10]; however, such figures rely on patient reporting of cough, a potential limitation when these measures often correlate poorly with objective quantification of coughing in several other conditions [11–14]. Although acute cough is usually self-limiting and transient, like chronic cough it significantly impairs quality of life [15], and may even precipitate chronic coughing [16].
Despite the magnitude of the problem of acute cough, few studies have assessed the effectiveness of available OTC cough medicines. Most studies suggest that current therapies are no more effective than placebo, hence they cannot be recommended [17]. This, together with increasing concerns about the safety of anti-tussives in children has led the Medicines and Healthcare Products Regulatory Agency and US Food and Drug Administration to introduce restrictions in their use [18–20].
The testing of existing and novel anti-tussive therapies has, until recently, been constrained by the lack of validated tools for the assessment of coughing. However, we have found, using custom-built digital recording equipment, that it is possible to record and objectively quantify cough sounds over 24-h periods in ambulatory patients [21]. The study of treatments for acute cough associated with URTI is often considered particularly difficult due to its transient nature, the requirement for large parallel-designed studies and significant placebo effects [22], but the studies upon which these perceptions are based have only measured cough over periods of up to 3 h [23, 24]. The objective measurement of acute cough over longer time periods in ambulatory patients may overcome some of these difficulties. Therefore, the aims of this study were to: 1) measure objective ambulatory cough frequency in otherwise healthy adults with acute cough and symptoms suggesting a URTI; 2) establish the short-term variability of acute cough associated with URTI symptoms; 3) understand the relationships between objective and subjective measures of cough; and 4) to perform power calculations for the design of future studies of novel anti-tussive agents.
MATERIALS AND METHODS
Subjects
Otherwise healthy adults complaining of a cough <3 weeks in duration and with a history of current or preceding symptoms suggestive of a viral URTI (i.e. at least one of rhinorrhoea, sneezing, post-nasal drip, nasal congestion, sore throat, hoarse voice, fever and headache) were recruited using poster advertisements. Current smokers and ex-smokers with a smoking history of >20 pack-yrs were excluded, as were those with abnormal spirometry (forced expiratory volume in 1 s (FEV1) <80% predicted or FEV1/forced vital capacity (FVC) <0.7). Subjects taking angiotensin-converting enzyme inhibitors, codeine or other anti-tussive medicines (including OTC treatments) were also excluded. All subjects provided written informed consent and the study was approved by the local ethics committee (Tameside and Glossop 08/H1013/81; Manchester, UK).
Study design
Subjects attended the Translational Research Facility (University Hospital South Manchester, Manchester, UK) on three consecutive days. At the first attendance a medical history was collected, spirometry performed according to American Thoracic Society/European Respiratory Society standards [25] and, assuming the inclusion and exclusion criteria were met, subjects were fitted with an ambulatory cough monitor and provided with a symptom diary (session 1). Subjects attended again 24 h later; the cough monitor batteries and memory card were replaced and another symptom diary provided (session 2). The final visit occured a further 24 h later, when the cough monitor was removed and symptom diaries collected. OTC medicines were not permitted during the study period.
METHODS
URTI symptoms
At the initial visit the presence and onset of rhinorrhoea, sneezing, post-nasal drip, nasal congestion, sore throat, hoarse voice, fever and headache was documented. Subjects also reported when the cough started and the colour, frequency and volume of any sputum.
Objective cough frequency
Two 24-h ambulatory cough sound recordings were performed using a custom-built device with lapel and chest wall microphones (Vitalojak; Vitalograph Ltd, Maids Moreton, UK). The numbers of explosive cough sounds per hour [26] were counted by a single trained person (K. Sunger) using an audio editing package (Adobe Audition 3.0; Adobe, San Jose, CA, USA). We have validated this technique against cough counting from video recordings [27], and found excellent agreement between trained observers [14, 28, 29]. To facilitate manual counting, silences and low-level background noises were removed by validated, custom-written software [30]. Subjects documented the times they went to bed and got up for each recording session; these defined the periods for the day and night cough rates.
Subjective cough measures
Visual analogue scales (VAS, 100 mm) were used to assess each subject's perception of the cough. For each 24-h session subjects recorded: 1) cough frequency (0 mm: no cough, 100 mm: worst cough); 2) severity (0 mm: no cough, 100 mm: severe cough); and 3) difficulty falling asleep due to coughing (0 mm: not at all, 100 mm: couldn't sleep).
Analysis
Analyses were performed using SPSS version 15.0 (SPSS Inc, Chicago, IL, USA) and SAS version 9.2 (SAS Institute Inc., Cary, NC, USA). The primary end-point, 24-h cough frequency, was positively skewed and therefore log transformed to allow parametric analysis; for other variables non-parametric tests were applied. Repeatability between sessions was assessed using intra-class correlation coefficients (two-way, random effects). Spearman's correlation coefficients were calculated for the relationships between cough measures.
As daytime cough frequency was highly repeatable and greater than at night, the daytime cough frequency data were used to estimate variance parameters corresponding to parallel group and crossover designs. Two generalised linear mixed models were fitted to the total daytime cough count using PROC GLIMMIX (SAS Institute, Inc.). Each model had a fixed effect for recording session, used length of daytime recording as a log offset term and assumed the responses followed a negative binomial distribution (log link function). The crossover design model had an additional random subject effect term fitted on the linear predictor. The corresponding variance parameter estimates were used to obtain the standard error of a treatment effect under simple future parallel and crossover study designs. This standard error was used to compute the power of detecting a 50% reduction in cough rate on active treatment relative to the cough rate on placebo (two-sided test, α=5%). Since the standard error of the treatment effect (and hence power) also depends upon the placebo response, several power curves were derived to cover a range of plausible future placebo response rates. For further details see the online supplementary material.
RESULTS
Subject characteristics
54 subjects completed the study (fig. 1). Subjects had a median age of 22 yrs (interquartile range (IQR) 21.0–25.8 yrs), median body mass index 23.2 kg·m−2 (IQR 21.0–27.4 kg·m−2) and 64% were female. Spirometry showed a mean FEV1 of 97.6±10.5% pred and FEV1/FVC ratio of 0.85±0.08. Two subjects were excluded with airflow obstruction, although we acknowledge that the FEV1/FVC ratio may underdiagnose airflow obstruction in a small percentage of young adults [31].

Summary of the recruitment of subjects. URTI: upper respiratory tract infection; ACE: angiotensin-converting enzyme; OTC: over-the-counter; FEV1: forced expiratory volume in 1 s; FVC: forced vital capacity; % pred: % predicted.
Reported URTI symptoms
Of the reported coryzal symptoms, 79.3% had rhinorrhoea, 72.4% sneezing, 70.0% post-nasal drip, 84.5% nasal congestion, 72.4% sore throat, 44.8% fever and 55.2% headache. The median reported duration of coughing at study entry was 4 days (IQR 3.0–7.0 days) and coughing started a mean 1.4±2.2 days after the cold started. 63.8% of subjects described a productive cough and, of these, 97.3% coughed up sputum daily and 2.7% weekly. 71.1% coughed up a teaspoon, 24.3% a tablespoon and 2.7% a cupful of sputum daily. 35.1% described the sputum as green, 27% yellow, 8.1% clear, 5.4% white and 24.3% did not know the colour.
Measures of acute cough
Objective cough frequency
A comparison of the measures of cough on both study sessions are summarised in table 1. Objective cough frequencies fell significantly from study session 1 to 2, a median of -2.4 coughs·h−1 (IQR -7.8– -0.1 coughs·h−1) and -28.2% (IQR -42.6− -1.2%) from baseline; see online supplementary figure E1 for a Bland–Altman plot. Considering daytime and night-time separately, only daytime cough frequency fell significantly; a median of -3.8 coughs·h−1 (IQR -11.2− -0.2 coughs·h−1) and -28.0% (IQR -44.3− -2.7%) from baseline. There were no significant correlations between the 24-h cough rate on either session 1 or 2 and the reported time since the cough or cold started. The difference in daytime cough rates between study sessions was also unrelated to the reported time since the cough started (r=0.05, p=0.72) or the cold started (r=0.18, p=0.18) (fig. 2).

Change in daytime objective cough frequency on study session 1 and 2 in relation to reported onset of a) cough symptoms and b) coryzal symptoms. Note log10 scales on both y-axes.
Cough rates in females were not significantly different from those in males for 24-h cough frequency (geometric mean 13.7 coughs·h1 (95% CI 10.2–18.4) versus 9.8 coughs·h (95% CI 6.8–14.1); p=0.15) or day (p=0.17) or night (p=0.21). Also, there was no apparent effect of age on cough frequency (r=0.4, p=0.79).
There was a marked diurnal variation in cough with substantially higher frequency during the day than overnight for both sessions (p<0.001 and p<0.001, respectively). Figure 3 shows the median cough frequency across all subjects at each time-point during the first 24-h recording period. It is notable that cough frequency in individuals was quite variable from hour to hour, although, interestingly, the profiles of these variations tended to be similar for the two sessions (fig. 4).

Hour-to-hour variability in cough counts for first 24-h monitoring period. Median counts are shown and error bars represent the interquartile range.

Examples of hour-to-hour variability in cough counts over both 24-h monitoring periods in two individual subjects with a) low cough rate (male aged 22 yrs, 2 days since cold onset, productive cough) and b) high cough rate (female aged 21 yrs, 2 days since cold onset, productive cough).
Subjective cough measures
Daytime cough frequency VAS followed a similar pattern to objective cough frequency but also showed a significant change at night-time; see online supplementary figures E2 and E3 for Bland–Altman plots. In contrast, VAS measures of cough severity and sleep latency did not significantly change between sessions.
Relationships between cough measures
There were significant weak–moderate-positive correlations (r=0.28–0.59) between objective cough rates and VAS measures for each study session (see online supplementary table E2 for details).
Repeatability of cough measures between study sessions
The intra-class correlation coefficients for the measures of cough are shown in table 2, suggesting that objective measures of cough are highly repeatable between the study sessions, especially daytime and 24-h cough frequency.
Relationships between changes in cough measures
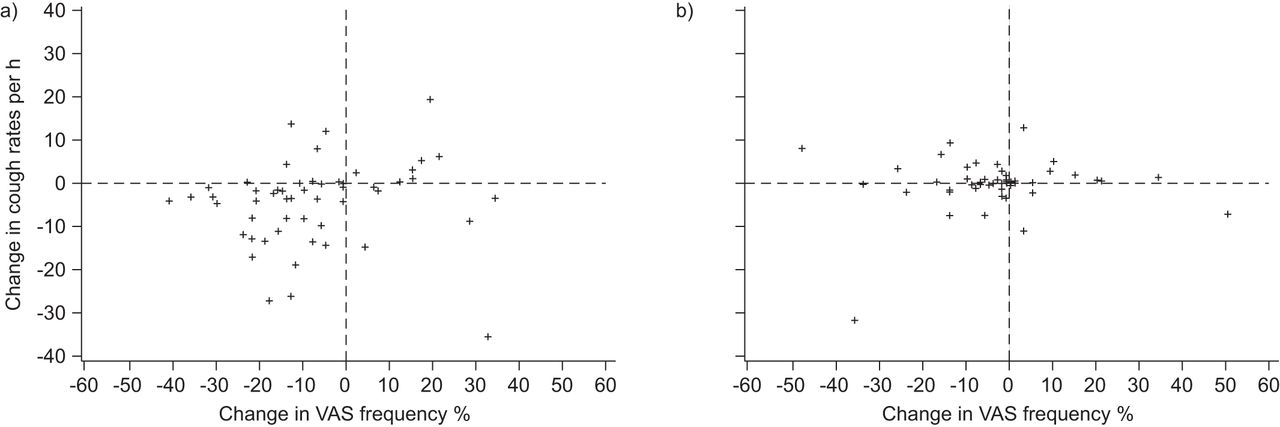
Figure 5 shows the relationships between the differences in objective cough counts and cough frequency VAS from session 1 to session 2. For daytime (fig. 5a), there was only a very weak linear relationship between objective and subjective estimates of change in cough (r=0.29, p=0.03), although the majority of subjects do appear in the left lower quadrant, i.e. both measures recorded an improvement in cough. Overnight however, most individuals cluster around the centre of the plot with little change in either measure (fig. 5b), suggesting very poor concordance between the subjective and objective changes, and no linear relationship (r=0.02, p=0.90).

Relationship between differences in objective cough frequency and cough visual analogue scale (VAS) from study session 1 to 2 for a) daytime and b) night-time.
Sample sizes for future study design in acute cough
The relationships between sample sizes and power to detect a 50% reduction in daytime cough frequency (over placebo) for both crossover and parallel group studies are shown in figures 6a and b, respectively. The influence of different placebo effects are also shown; for example, if the placebo response rate was mean 5 coughs·h−1, the green line displays the power to detect a 2.5 coughs·h−1 reduction against the total number of subjects, whereas if the placebo cough rate was 25 coughs·h−1, the yellow line displays the power to detect a 12.5 coughs·h−1 reduction.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Sample size calculations in acute cough for both a) parallel- and b) crossover-designed studies. Graphs display the balance between power and the total number of subjects required to detect a 50% reduction in cough frequency over placebo, calculated for a range of plausible cough rates on placebo therapy. Note that for parallel designs (a), each treatment arm would require half the number of subjects shown.
DISCUSSION
This is the first study to investigate 24-h objective cough frequency and its repeatability in otherwise healthy subjects complaining of an acute cough associated with URTI symptoms. Cough frequency was high and demonstrated significant variability between subjects. Although objective cough frequency fell significantly from session 1 to 2, it was highly repeatable, especially compared with VAS ratings of cough frequency, severity and sleep latency. Furthermore, changes in objective cough frequency were poorly predicted by changes in the cough frequency VAS ratings. Power calculations based on this data suggested that even considering sizeable placebo effects, anti-tussive efficacy could be observed in small numbers of subjects, especially if the characteristics of the medicine being tested allows for crossover-design studies.
It is interesting to note that the average cough frequency in acute cough was comparable to that which we have previously reported in patients presenting to a specialist clinic with chronic cough (>8 weeks duration) [11, 26] and in excess of rates observed in conditions such as chronic obstructive pulmonary disease [12], asthma [13] and cystic fibrosis [14]. This raises the possibility that similar mechanisms drive both acute and chronic coughing and one study has indeed suggested that one-third of chronic cough patients report their cough being initiated by an URTI [16]. Unlike in chronic cough [32], we did not observe any significant influence of age or sex on objective cough frequency in this study population, but the sample size may have been insufficient to detect these effects. This is, however, consistent with the finding that males and females with an acute cough have similar cough-specific quality-of-life scores, in contrast with chronic cough, where females have worse scores than males [15].
As might be anticipated for a viral illness, cough rates significantly dropped from session 1 to session 2, in keeping with cough resolving rapidly [8]. Whilst it is not possible to determine the mechanisms underlying the fall in cough frequency from this study, it is important to appreciate that objective cough frequency was still highly repeatable. This may seem contradictory, but the drop in cough rate was consistent across the range of cough frequencies at session 1, and the rank order of the patients (in terms of cough rates) remained very similar for session 2; therefore, although the absolute cough rates fell, the variability in cough frequency within subjects (between sessions 1 and 2) was much less than the variability between subjects (within each session), resulting in high intra-class correlation coefficients and repeatability. This finding has important implications for future trial design, suggesting that crossover studies utilising objective cough frequency measures are feasible over a 48-h period. Such a study design would only be appropriate for short-acting agents with rapid onset/offset and equal efficacy in patients, irrespective of their baseline cough rates; such characteristics are, however, likely to be desirable in a therapy for acute cough. It is also noteworthy that the reported onset date of the cough or cold symptoms did not predict the objective cough frequency, suggesting that the trajectory of objective cough counts in viral illness is highly variable. Within the 3-week time window for acute cough, it is therefore unnecessary to target patients with any particular reported symptom duration for recruitment.
The importance of the placebo effect in the treatment of acute cough has been frequently highlighted, and may be responsible for up to 85% of the efficacy of some cough medicines [24]. These large effects have generally been found under laboratory conditions, monitoring cough over just 15-min periods. Such conditions might be expected to exaggerate placebo effects compared with monitoring over 24 h in a subject's own environment. Nonetheless, when performing power calculations from this data we included a wide range of placebo means (representing potential outcomes of small and large placebo effects) and still found sample sizes to be relatively small.
For our power calculations, we estimated that an improvement of 50% in objective cough frequency may be required for patients to appreciate an improvement in their cough. Studies with effective medicines are needed to clarify this issue; however, in chronic cough patients undergoing reflux monitoring with a naso-gastric catheter a fall of one-third in objective cough frequency was accompanied by a significant improvement in cough VAS, suggesting that this change was perceived as an improvement [33]. In the absence of data specific to acute cough, we estimated that a slightly larger change (i.e. 50% fall) might be necessary for an improvement in coughing to be appreciated; however, this figure may differ significantly across conditions.
This study has some limitations. First, our study population was mainly young adults, and therefore it remains to be determined whether cough frequencies may be different in older adults with URTI symptoms. Epidemiological data would suggest that the incidence of URTI tends to be inversely correlated with age and that the sample we studied (adults in their early 20s) are representative of the age group most frequently affected by URTI episodes (apart from children) [34, 35]. Secondly, our sample contained more females than males. It is known that more females present to general practice with coughs secondary to URTI [34], which may also explain the excess of females presenting for inclusion in this study. Indeed other studies of treatments for acute cough have often recruited a similar proportion of females [36–38]. Finally it remains to be seen whether limiting recruitment to patients earlier in the natural history of colds has any significant impact on the variability and repeatability of cough frequency.
In summary, this study shows that acute cough rates are comparable to those found in chronic cough and highly repeatable over any 48-h period. These findings have significant implications for the testing of novel anti-tussive agents, demonstrating that objective cough frequency monitoring is a more powerful tool than subjective measures of acute cough, reducing the number of subjects required and making crossover designs possible.
Acknowledgments
We wish to acknowledge the contribution of all the volunteers who took part and also the funding provided by GlaxoSmithKline.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Support Statement
The study was funded by GlaxoSmithKline and the Medical Research Council. J. Smith is funded by a Clinician Scientist Fellowship from the Medical Research Council.
Statement of Interest
Statements of interest for W.M. Powley, R. Murdoch and J.A. Smith, and for the study itself can be found at www.erj.ersjournals.com/site/misc/statements.xhtml
- Received November 1, 2011.
- Accepted June 11, 2012.
- ©ERS 2013
REFERENCES










