





Abstract
Endothelin receptor antagonists are used to treat idiopathic pulmonary arterial hypertension (IPAH), but human pulmonary arterial endothelin receptor expression is not well defined. We hypothesised that disease and treatment would modify normal receptor distribution in pulmonary resistance arteries of children.
Using immunohistochemistry and semiquantitative analysis, we investigated endothelin receptor subtypes A and B (ETA and ETB, respectively), and endothelial nitric oxide synthase (eNOS) expression in peripheral pulmonary arteries of tissue from untreated children with IPAH (n=7), following extended combined bosentan and epoprostenol therapy (n=5) and from normal subjects (n=5).
Clinical, haemodynamic and pathological abnormalities were severe and advanced in all IPAH cases. ETA was detected in pulmonary arterial endothelial cells of all normal and diseased tissue and cultured cells. Endothelial ETA, ETB and eNOS expression was reduced in patent, plexiform and dilatation lesions of untreated cases, but in treated cases, ETA and ETB were normal and eNOS increased. In smooth muscle, ETA expression was reduced in treated cases but ETB expression increased in all arteries of both treated and untreated cases.
In summary, ETA is expressed on human pulmonary arterial endothelium. In IPAH, combination treatment with bosentan and epoprostenol had a more marked influence on endothelin receptor expression of endothelial than smooth muscle cells.
- Endothelin receptor antagonists
- endothelin receptor A and B
- endothelium
- paediatric idiopathic pulmonary arterial hypertension
- peripheral pulmonary arteries
Idiopathic pulmonary arterial hypertension (IPAH) is a rare, incurable disorder occurring in both children and adults with a normally formed heart, characterised by irreversible occlusion of small intra-acinar pulmonary resistance arteries with development of plexiform lesions resulting in a sustained increase in pulmonary arterial pressure [1]. Death results from right heart failure. Treatment with prostacyclin, endothelin receptor antagonists and phosphodiesterase inhibitors aims to promote dilatation and reparative remodelling of the pulmonary arteries, and has improved survival and quality of life but is not curative [1]. The only therapeutic option for end-stage disease is lung transplantation.
The endothelin ET-1 is a potent vasoconstrictor and smooth muscle cell mitogen [2] that is important in the pathobiology of pulmonary arterial hypertension [3]. In humans with IPAH, plasma endothelin levels are elevated [4], endothelin-converting enzyme activity is enhanced [5] and lung expression of endothelin is increased [6]. Its action is mediated principally by two receptors, ETA and ETB [7]. Both mediate vasoconstriction of human smooth muscle cells whilst endothelial ETB receptors mediate vasorelaxation via endothelial nitric oxide synthase (eNOS) [8]. In experimentally induced pulmonary hypertension, the endothelin receptor antagonists diminish or abrogate endothelin-induced smooth muscle cell contraction, hypertrophy, hyperplasia and fibrosis [9–11].
Inflammation plays a prominent role in IPAH [12] and experimental blockade of ET-1 receptors inhibits activation of inflammatory pathways [13]. We have recently shown that the nonselective endothelin receptor antagonist bosentan, given with prostacyclin, leads to a significant reduction in the morphological evidence of endothelial cell activation in children with IPAH [12] as indicated by human leukocyte antigen (HLA)-DR expression. These beneficial changes were not, however, accompanied by evidence of reparative vascular remodelling [12].
In the present study, we hypothesised that treatment with bosentan, a nonselective endothelin receptor blocker, combined with intravenous epoprostenol, would result in modification of endothelin receptor expression by endothelium and smooth muscle in pulmonary arteries. We also examined endothelial eNOS expression since a treatment-associated improvement could be an indication of improved endothelial function [14]. Immunohistochemistry was used to compare the expression of ETA and ETB receptors in pulmonary resistance arteries within lungs from normal children and children with IPAH who had and had not received combination therapy with bosentan and epoprostenol. Receptor expression was also studied in endothelial cells cultured from the explanted lung. The alveolar capillary bed continues to be perfused, although to a greatly reduced degree because of upstream obstruction and occlusion of arterioles [15]. Therefore serial reconstructions were made to find the extent of ET-1 receptor expression along the remodelled route by which blood reaches the capillary bed.
MATERIALS AND METHODS
Patients
There were 12 cases of IPAH (table 1), five treated with combined bosentan and epoprostenol therapy (referred to subsequently as “treated”) and seven “untreated”, four of these having only been given nifedipine, one with nifedipine in combination with sildenafil. Treated children received bosentan according to weight [17] over a mean (range) period of 20.78 (12.2–27.9) months and epoprostenol at a dosage of 43.5 (40–50) ng·kg−1·min−1 over a mean (range) period of 31.66 (16.8–45.2) months. Of the seven untreated children, six presented before the discovery/introduction of pulmonary hypertension-specific therapies and one soon afterwards, this child having been given sildenafil. This last patient died the day after being admitted to our pulmonary hypertension centre. The bone morphogenetic protein receptor 2 mutation status of all children was unknown.
Tissue
Six samples were taken at lung transplantation, three at post mortem and three were diagnostic lung biopsies. In addition, archival post mortem tissue was obtained from two children and three adults who had no cardiovascular abnormality. All samples were used with permission (Institute of Child Health and Great Ormond Street Hospital for Children REC 05/Q0508/49 and Huntingdon Local REC H00/531/T), and the explanted tissue was used with the explicit informed consent from the children’s parents.
Immunohistochemistry
Sections from all cases, normal and abnormal, were incubated with primary antibodies (supplementary table 1) and biotin-conjugated secondary antibodies, and visualised with diaminobenzidine. Specificity of staining was controlled with an inappropriate secondary antibody and/or by omission of the primary antibody. Colour and fluorescent images were acquired with Image-Pro using colour or monochrome digital cameras (MediaCybernetics, Bethesda, MD, USA).
Analysis of immunohistochemical staining
Slides were anonymised and the distribution of ETA (ab12977; Abcam, Cambridge, UK) and ETB (ab12980; Abcam) staining in pre- and intra-acinar pulmonary resistance arteries was assessed semiquantitatively in 12 IPAH and five normal cases. Sections were examined using a 40× objective lens, and arteries scored for presence or absence of both endothelial and smooth muscle staining (supplementary material). Endothelial damage, represented by discontinuities in eNOS expression, was assessed quantitatively in four normal children and adults, and four untreated and four treated children (supplementary material). The expression of ETA, ETB and eNOS in endothelial cells within obstructed arteries, plexiform lesions and dilatation vessels were evaluated. In all cases the percentage wall thickness of all respiratory bronchiolar pulmonary arteries was calculated [16].
Cells
Pulmonary arterial endothelial cells were isolated from second-generation intrapulmonary elastic arteries from one child with IPAH (supplementary material). Normal adult pulmonary arterial endothelial cells were purchased from TCS Cellworks (Buckingham, UK).
ETA and ETB expression in endothelial cells: immunofluorescent co-localisation
Co-localisation of ETA (ab12977) and ETB (ab12980) with the endothelial cell marker CD31 (Dako, Glostrup, Denmark) was studied in tissue from three untreated and three treated children with IPAH. Co-localisation with CD31 was also studied in cell monolayers from a child with IPAH and normal pulmonary arterial endothelial cells [12]. Control sections were incubated with anti ETA or ETB and an irrelevant secondary antibody.
Western blotting
Extracts from confluent monolayers of pulmonary arterial endothelial cells were electrophoresed and blotted to assess ETA and ETB expression using densitometry (supplementary material).
Serial reconstructions
Serial reconstructions were made of plexiform lesions from two untreated and two treated cases (2–4 lesions per case). Alternate serial sections were stained for endothelial and smooth muscle cell specific proteins and reconstructions made from micrographs taken with either a 4× or 10× objective lens.
Statistical analysis
Values obtained in arteries of normal lungs and those of children with untreated and treated IPAH were compared using ANOVA with Tukey’s pairwise comparisons. Kruskal–Wallis and Mann–Whitney tests were used to compare non-normally distributed data.
RESULTS
Resistance arteries of normal children and adults
Endothelium
In all the normal paediatric and adult samples examined, the endothelium of muscular pre- and intra-acinar pulmonary resistance arteries stained positively for both ETA and ETB (figs 1 and 2). More labelling of ETA and ETB receptors was present in peripheral than in conduit arteries. In all samples, endothelial eNOS expression was strong and was unbroken in mean±sem 90.2±7% of arteries (fig. 3).

Immunohistochemical staining for the endothelin receptors ETA and ETB, visualised by diaminobenzidine (brown), in sections counterstained with haematoxylin. Adjacent sections of representative pulmonary respiratory bronchiolar artery (pulmonary resistance artery accompanying a respiratory bronchiolus) of a) a normal child, and of b) untreated and c) treated children with idiopathic pulmonary arterial hypertension. d) Untreated and e) treated plexiform lesions. Images at low and higher magnification; scale bars=50 μm in low- and 20 μm in high-magnification images.

Histograms of semiquantitative assessment of expression of the endothelin receptors ETA and ETB in a) endothelium and b) smooth muscle tissue sections of two normal children and three adults, and those with idiopathic pulmonary arterial hypertension (seven untreated and five treated). **: p<0.01.

Endothelial nitric oxide synthase (eNOS) expression in pulmonary respiratory bronchiolar arteries and plexiform lesions of normal children, and untreated and treated children with idiopathic pulmonary arterial hypertension (IPAH). An endothelial cell not expressing eNOS (#) is visible only in the untreated child. Scale bar=20 μm.
Since pulmonary arterial endothelial ETA expression had not previously been reported by immunohistochemistry in pulmonary arteries of the human lung, we used three different anti-ETA antibodies to confirm staining specificity: ab12977, AER-001A (Alomone Labs, Jerusalem, Israel) and an anti-ETA (53D) kindly provided by A.P. Davenport (University of Cambridge, Cambridge, UK) (table 2).
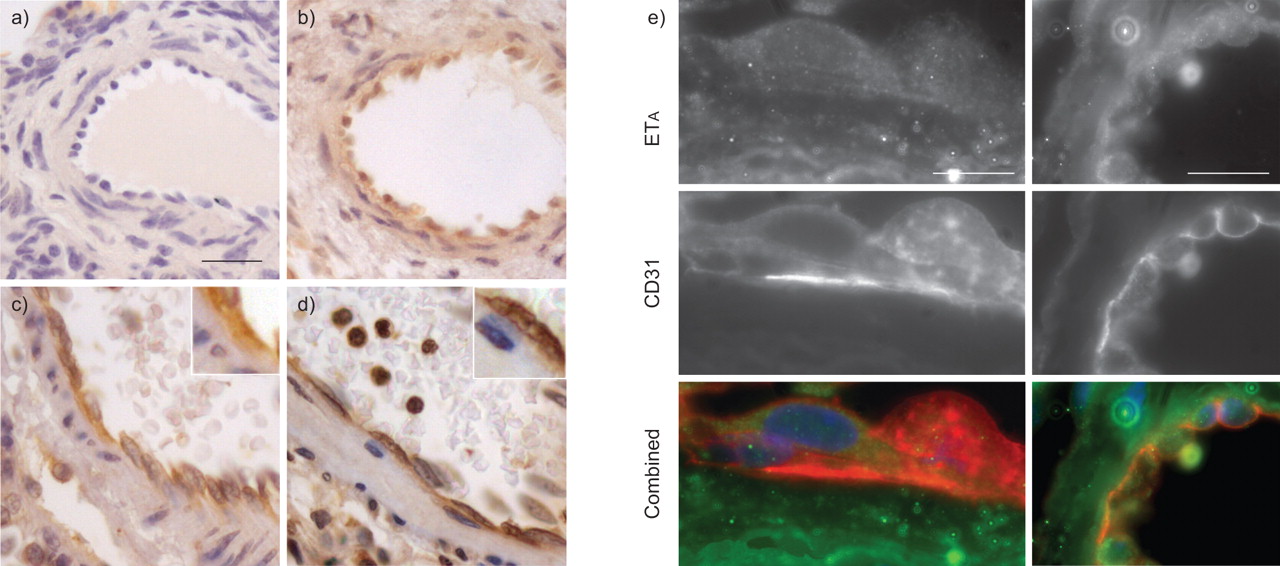
All antibodies showed positive staining of the endothelium in normal resistance arteries (fig. 4a–d). These antibodies were directed against different intracellular and extracellular regions of the ETA molecule but all gave a similar staining pattern in all specimens. Immunofluorescent co-localisation of ETA staining with the endothelial marker protein, CD31, confirmed ETA expression on endothelial cells (fig. 4e). Furthermore, Western blots of extracts of cultured normal adult pulmonary arterial endothelial cells showed a single strong ETA band at 47 kDa (fig. 5).

Immunohistochemical labelling for the endothelin-1 receptors, ETA and ETB, in normal muscular pulmonary arteries. a) Absence of endothelial staining when incubated with anti-ETA pre-incubated with control peptide antigen (AER-001A; Alomone Labs, Jerusalem, Israel). b) Endothelial staining visible following incubation of an adjacent section of the same artery with the same antibody without peptide block. c and d) Similar staining for anti ETA using c) ab12977 (Abcam, Cambridge, UK) and d) 53D (a gift from A.P. Davenport, University of Cambridge, Cambridge, UK) on adjacent sections. Insets show endothelial staining at ×2 magnification. Scale bar=20 μm. e) Immunofluorescent co-labelling demonstrates endothelial expression of ETA in terminal bronchiolar pulmonary resistance arteries of two children with idiopathic pulmonary arterial hypertension (left: treated; right: untreated). Overlay images of ETA staining (green) and the endothelial marker CD31 (red) show that both are detectable on the endothelium. Scale bars=10 μm.

Representative Western blots of extracts from duplicate cultures of one normal and one idiopathic pulmonary arterial hypertension (IPAH) endothelial cell isolate. 10 μg protein was loaded in each lane. The blot was sequentially stained for the endothelin receptors ETA and ETB, with β-actin as a loading control. ETA and ETB expression was similar in normal and IPAH cell extracts.
Resistance arteries of children with IPAH
The morphological findings were severe in all 12 cases, whether the tissue was obtained at biopsy, post mortem or transplantation. They showed a similar increase in the percentage medial thickness (table 1), and all showed plexiform lesions and dilatation lesions, indicating severe Heath and Edwards grade IV disease or more.
Children not receiving treatment
Endothelium
Semiquantitative analysis showed that ETA expression on the endothelium of all patent, dilated and obstructed arteries, and within plexiform lesions was weaker in untreated children with IPAH than in normal arteries (figs 1b and 2; table 2). ETB expression was slightly but not significantly weaker than normal in untreated children (figs 1a and 2; table 2). eNOS expression was weak in all arteries and only 20.9±6.3% of arteries had a continuous eNOS-positive endothelium (p<0.001 compared with normal; fig. 3), indicating endothelial dysfunction or damage.
Smooth muscle
In untreated children, medial smooth muscle ETA expression in patent arteries was similar to normal (figs 1b, 1d and 2; table 2), but was weak or absent in dilated and obstructed arteries and plexiform lesions (fig. 1d). By contrast, ETB expression was significantly increased in the medial smooth muscle of all the arteries (figs 1b and 2; table 2).
Children receiving treatment with bosentan and epoprostenol
Endothelium
Both ETA and ETB expression was similar to normal, and was significantly greater in all patent, dilated and obstructed arteries, and plexiform lesions of treated than untreated children (figs 1c, 1e and 2; table 2). Similarly, eNOS expression increased in all arteries (fig. 3; table 2). In patent arteries, the proportion of vessels having an unbroken eNOS-positive endothelium had increased, being greater than in untreated cases and similar to normal: 90.6±6.4% (p<0.001 compared with untreated cases; fig. 3; table 2).
Smooth muscle
In treated children, ETA expression in the medial smooth muscle in all patent arteries was significantly reduced compared with both normal and untreated children (figs 1c and 2; table 2), but was unchanged in dilated and obstructed arteries and plexiform lesions. By contrast, ETB expression in all arteries of the treated cases was high and similar to that in the untreated cases (figs 1c, 1e and 2; table 2).
ETA and ETB expression by cultured endothelial cells
Monolayers of normal, adult pulmonary arterial endothelial cells and pulmonary arterial endothelial cells isolated from a treated child had a similar appearance and showed positive immunostaining for ETA in all cell extracts (fig. 6). Western blots revealed both an ETA band at 47 kDa and an ETB band at 60 kDa (fig. 5). There was no significant difference in either the ETA or ETB content between normal and IPAH endothelial cells (mean±sd density for ETA: normal 204.1±28.3, IPAH 218.2±27.1; ETB: normal 180.0±47.3, IPAH 210.9±25.5). These findings are in accord with the immunohistochemical studies of the arterial wall in the treated children.

Immunofluorescence staining for the endothelin receptors ETA and ETB at the surface of pulmonary arterial endothelial cells derived from a normal adult and a child with idiopathic pulmonary arterial hypertension (IPAH) who had been treated with bosentan and epoprostenol. Control cells were incubated with ETA and an irrelevant secondary antibody. There is no detectable difference in staining between the cell lines. Scale bar=10 μm.
Influence of bosentan and epoprostenol on the pathology of plexiform lesions
We found that plexiform lesions were present along a greater length of the arterial pathway in treated than in untreated cases, 30±9.7% being found more proximally in treated pre-acinar arteries compared with 1.1±1.1% in pre-acinar arteries in the untreated cases (p<0.01).
Serial reconstruction of pathways around arterial obstruction to the capillary bed
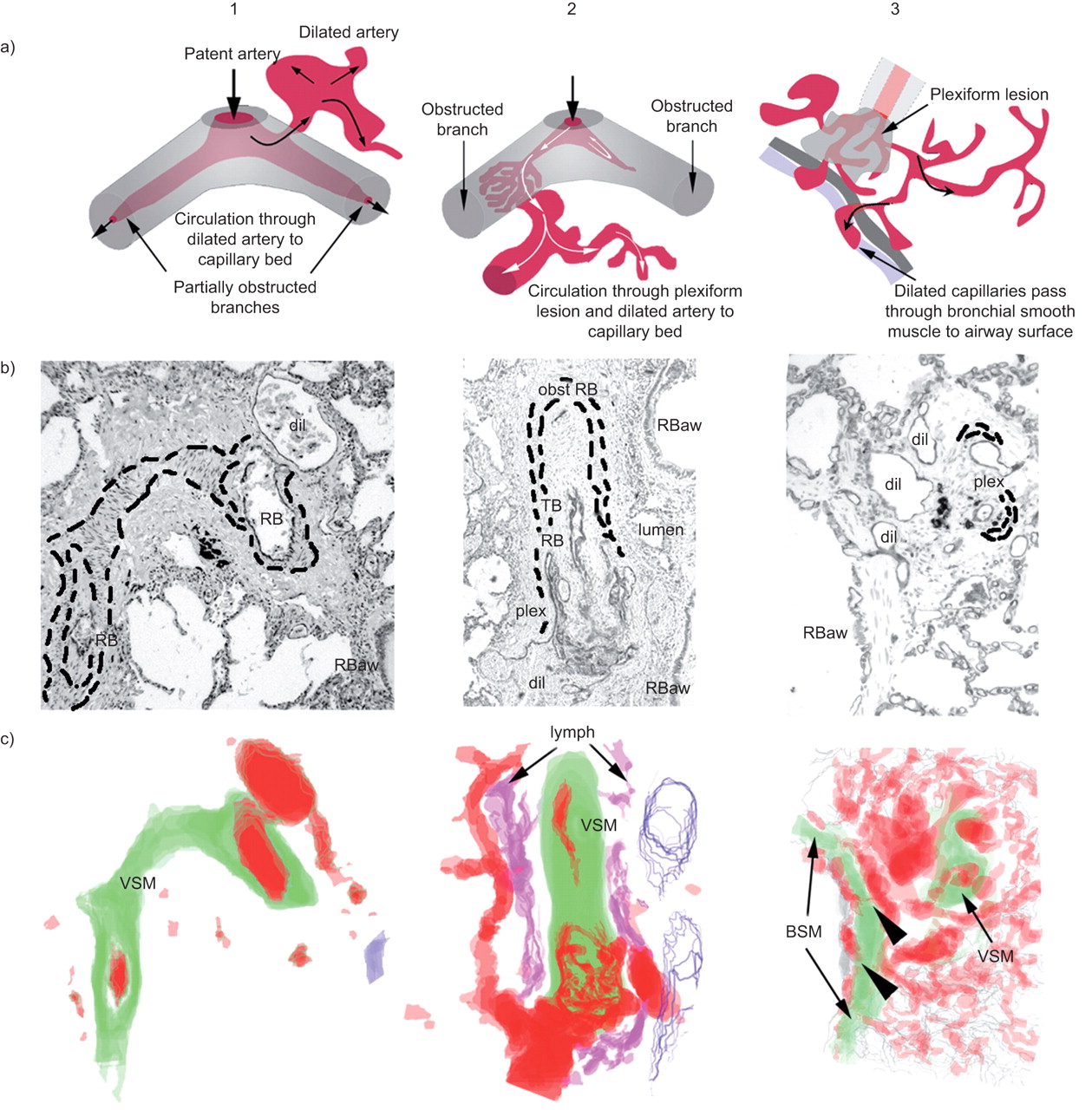
In both treated and untreated children, where partial or complete obstruction of the axial arterial pathway occurred, the circulation of blood was maintained through vessels that originated as branches of the axial artery arising proximal to the obstruction. These branches were continuous peripherally with the capillary bed (fig. 7, columns 1 and 2). In two reconstructions, a plexiform lesion was present within the lumen of the axial pulmonary artery proximal both to the obstruction and to the origin of dilated arteries (fig. 7, columns 2 and 3), and vascular pathways were continuous through the plexiform lesion to the dilated arteries and the capillary bed beyond (fig. 7, column 2). In treated children, there was extensive abnormal capillary vascularisation of the walls of respiratory bronchioles (fig. 7, column 3), which was continuous with plexiform lesions. In all children with IPAH, dilated lymphatics (fig. 7, column 2) were frequently observed around partially and completely obstructed terminal and respiratory bronchiolar pulmonary arteries, but in no case were they found to connect with either pulmonary arteries or capillary plexus.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Serial reconstructions displaying the origins of dilatation vessels in idiopathic pulmonary arterial hypertension. a) Diagrams derived from reconstructions obtained from photomicrographs as in b) in which alternate sections are stained for CD31. dil: dilated vessels; RB: respiratory bronchiolar artery; RBaw: respiratory bronchiolar airway; obst RB: obstructed respiratory bronchiolar artery; TB: terminal bronchiolar artery; plex: plexiform lesion; interrupted lines indicate margins of medial smooth muscle. c) Stacked overlays of photomicrographs of serial sections. Red: vessel lumen; blue: airway epithelium; green: smooth muscle (arterial medial layer (VSM) and airway smooth muscle (BSM)); purple: associated lymphatics in column 2 (lymph). Arrowheads: connections between dilated vessels and abnormal vascularisation at the surface of the respiratory bronchiolus.
DISCUSSION
This study has shown for the first time that ETA receptors are expressed on the endothelium of human peripheral pulmonary arteries, in normal and IPAH lungs, and in cultured pulmonary artery endothelial cells. In children with IPAH, endothelial ETA, ETB and eNOS expression was reduced in the untreated patients but not in those on combination therapy (a nonselective endothelin receptor antagonist plus epoprostenol). In vascular smooth muscle, ETA expression was reduced in treated children while ETB expression was increased to as great an extent in treated as in untreated children. We had to consider whether the presence of bosentan could mask the binding and localisation of antibodies to the receptors, but since the ET-1 receptor antagonists bind to the second transmembrane domain of receptor sites and endothelin antibodies typically bind to the C-terminus, which is a different domain, this seemed highly unlikely [18]. Serial reconstruction of peripheral arterial pathways indicated that progressive occlusion was associated with the formation, or recruitment, of more proximal bypass branches to supply the alveolar capillary bed, often via plexiform lesions, all of which retained an endothelium expressing ETA, ETB and eNOS.
Previous failure to visualise pulmonary endothelial ETA is probably explained by the use of thick cryosections (20–30 μm) in competitive radioactive ligand binding techniques [19]. ETA receptors have now been found in humans in the endothelium of the aorta [20], cerebral arteries [21], the cornea [22] and colon [23]. In human pulmonary endothelium, the ETA receptor is predominantly intracellular and thought to mediate ET-1-stimulated increase in intracellular calcium [20], which may enhance further ET-1 release [24]. ET-1 is pro-inflammatory [25], and activation of ET-1 receptors on endothelial cells results in increased permeability [26] and enhanced neutrophil adhesion and migration [27]. In pigs and hamsters, the ETA receptor is associated with activation of inflammation [28, 29]. Aberrant ET-1-induced cell proliferation and/or survival is implicated in the pathogenesis of many malignancies [30, 31]. Thus, the endothelial ETA receptor may be particularly important in pulmonary vascular disease characterised by impaired endothelial barrier function and excessive endothelial proliferation that has been likened to a malignant process [32].
Endothelial expression of both endothelin receptor subtypes was reduced in the untreated children with IPAH and was significantly greater, similar to normal, in the treated children. This may reflect a reduction in endothelial damage and dysfunction, which is indicated by the normal eNOS immunostaining pattern, in the treated cases. The greater than normal ETB expression in treated children could be adaptive and compensatory [33], but whether this would have helped preserve pulmonary clearance of endothelin and increase vasodilatation is very uncertain, since bosentan may well have blocked all receptor activity. The greater endothelial eNOS expression is more likely to be due to the epoprostenol therapy than to the activity of the ETB receptors. Long-term epoprostenol given as monotherapy has been shown to improve endothelial function, as judged by an improvement in the net balance between pulmonary ET-1 clearance and release and the coagulation profile [34]. In the present study, it is obviously impossible to dissect how the administration of bosentan and/or prostacyclin might have influenced endothelial function.
In the smooth muscle cells, the current study findings suggest that treatment had no effect on the heightened expression of ETB receptors, but did reduce ETA expression. An earlier in vitro autoradiographic study showed a two-fold increase in endothelin receptor density on the smooth muscle cells of pulmonary hypertensive patients but could not, using this technique, show predominance of either subtype [35]. Other investigators, however, have reported a preferential increase in ETB receptors in pulmonary arteries of pulmonary hypertensive scleroderma patients [36]. Although both receptor subtypes mediate ET-1-induced contraction [37] and promote proliferation [35], achieving a reduction in only ETA expression could be beneficial. Indeed, the observed reduction in endothelial ETA receptor may indicate a maintained reduction in ET-1 release from these cells [20].
In addition to receiving a nonselective endothelin receptor antagonist, our patients were also receiving a continuous epoprostenol infusion. Conflicting effects of nonselective bosentan/epoprostenol treatment may result in modification of endothelial function. The expression of endothelin receptors is important in its own right and also because of the potential interaction between the endothelin and prostacyclin signalling pathways. ETB receptor stimulation in pulmonary arterial smooth muscle cells reduced agonist-stimulated intracellular cyclic AMP (cAMP) levels, consistent with the negative coupling of ETB receptors to adenyl cyclase [35]. The ETA-mediated stimulation of cAMP-dependent protein kinase A activity in vascular smooth muscle cells as profoundly as isoproterenol, resulting in promotion of cell hypertrophy [38]. Conversely, prostacyclin inhibits ET-1 release from endothelial cells [39], and the prostacyclin analogue cicaprost inhibited ET-1 release from human pulmonary arterial smooth muscle cells [40]. Thus, prostacyclin inhibition of endothelin release may contribute to the antiproliferative effect of the prostacyclin analogues. A continuous prostacyclin infusion also improves the net balance between pulmonary endothelin clearance and release in patients with IPAH [41], which may be particularly important in bosentan-treated patients who experience an increase in the level of plasma endothelin [42].
The serial reconstructions showed that the patients maintained on continuous i.v. epoprostenol and bosentan for >3 yrs had an extensive collateral circulation, bypassing the vascular obstructions through vessels arising from the axial pathway immediately proximal to the obstruction, and being continuous with an extra-alveolar capillary bed at the surface of the bronchial epithelium and the alveolar capillary bed. Comparison of treated and untreated cases suggests that, with treatment, increased longevity was associated with the centripetal progression of disease from the most peripheral intra-acinar arteries to the small pre-acinar vessels, and associated with a significant increase in diameter of the plexiform lesions [12]. The current findings suggest a cycle of obstruction and angiomatoid proliferation, followed by the dilatation of more vessels, possibly supernumerary arteries, proximal to the obstruction. These changes could be considered as adaptive, ensuring continued perfusion of the capillary bed, but the mechanisms initiating and maintaining the process are unknown. The progression of an angiomatoid endothelial tumour process would give similar histological findings [43]. The obstructive changes are consistent with physiological studies showing a reduction in alveolar–capillary surface area in patients with IPAH [15]. ETA and ETB expression on the endothelial and intimal smooth muscle cells within plexiform lesions and dilatation arteries mirrored that seen in the unobstructed peripheral arteries. Together with eNOS, activation of these receptors could help regulate blood flow through these abnormal vascular channels.
The presence of endothelin receptors in obstructed arteries and plexiform lesions may be important in the context of the cancer hypothesis of pulmonary vascular disease. ETA activation induces vascular endothelial growth factor production by increased hypoxia-inducible factor-1α, and triggers activation of signalling pathways linked to tumour cell proliferation, apoptosis protection, invasiveness and angiogenesis [44]. Endothelin receptor antagonists are considered potential anti-cancer agents and may be having a comparable beneficial effect in established pulmonary vascular disease [45].
We found no evidence of reparative remodelling toward a normal arterial architecture in these children, and smooth muscle cells derived from three of the treated children reported here have, in vitro, abnormally high replication rates [46]. The extent to which the drugs directly affect the vasculature is uncertain. Clinical experience indicates that cardiac output is increased, and this would increase lifespan and allow the pulmonary vascular abnormalities to progress and increase in severity. The findings presented here suggest that prostacyclin and bosentan may prolong life in these children, either directly or indirectly, by enhancing abnormal peripheral arterial connections to the capillary bed. Clarification of the endothelin signalling pathways in pulmonary vascular disease, and of the interaction between them and the prostacyclin pathways, is crucial to improving therapy with medicines that directly and indirectly influence these pathways. Our findings suggest that selective ETA antagonists may be beneficial as endothelial ETA in obstructed arteries and plexiform lesions may offer a novel therapeutic target, beneficial endothelial ETB function being preserved. Bosentan did not reduce vasoconstrictor ETB receptors on the smooth muscle.
Thus, current ET-1 receptor antagonist and prostacyclin therapy may have greater effects on endothelium than on vascular smooth muscle of peripheral pulmonary arteries. These are descriptive studies and have to be viewed in that context. However, the observations presented here should aid the design of hypothesis-generated functional studies at the cellular level in humans, which should ultimately improve the care of children with IPAH.
Footnotes
This article has supplementary material available from www.erj.ersjournals.com
Statement of Interest
Statements of interest for N. Davie and S.G. Haworth can be found at www.erj.ersjournals.com/site/misc/statements.xhtml
- Received October 26, 2010.
- Accepted February 15, 2011.
- ©ERS 2011
REFERENCES










