





Abstract
The optimal timing of exogenous surfactant application to reduce pulmonary injury and dysfunction was investigated in a rat lung ischaemia and reperfusion injury model.
Lungs were subjected to flush perfusion, surfactant instillation, cold ischaemia (4°C, 4 h) and reperfusion (60 min). Animals received surfactant before (group 1) or at the end (2) of ischaemia, or during reperfusion (3) or not at all (4). Control groups included “worst case” without Perfadex and surfactant (5), “no injury” without (6) or with surfactant (7), and ischaemia with pre-ischaemic surfactant (8). Intra-alveolar oedema and blood–air barrier injury were estimated by light and electron microscopic stereology. Perfusate oxygenation and pulmonary arterial pressure (Ppa) were determined during reperfusion in groups 1 to 4.
Intra-alveolar oedema was almost absent in groups 1, 6, 7 and 8, pronounced in 2, 3 and 4, and severe in 5. Blood–air barrier injury was moderate in groups 1 and 8, slightly pronounced in 2, 3 and 4, extensive in 5 and almost absent in 6 and 7. Perfusate oxygenation was significantly higher in group 1 compared with groups 2 to 4. Ppa did not differ between the groups.
In conclusion, exogenous surfactant attenuates intra-alveolar oedema formation and blood–air barrier damage and improves perfusate oxygenation in the rat lung, especially when applied before ischaemic storage.
Although great efforts have been made to improve lung preservation in human lung transplantation, post-ischaemic primary graft dysfunction (PGD) is still a major problem in the early post-transplant period 1, 2. The main reason for PGD is ischaemia/reperfusion (I/R) injury, clinically manifesting within a spectrum from mild acute lung injury (ALI) to severe acute respiratory distress syndrome (ARDS). I/R injury is associated with increased short- and long-term morbidity and mortality 1, 3, 4. During I/R injury, the graft organ develops structural damage, such as interstitial and intra-alveolar oedema formation and loss of integrity of the blood–air barrier 5, 6. In addition, the surfactant system of the lung is severely affected by ischaemia and reperfusion, leading to the development of oedema and atelectases 7–11.
Several experimental 12–21 and clinical 22–24 studies give evidence that exogenous surfactant therapy successfully supplements the imbalanced endogenous surfactant system, serving to attenuate I/R injury and effectively improve lung preservation and graft function 11. The great advantage of exogenous surfactant therapy of the donor in human lung transplantation is the fact that PGD in this case can accurately be predicted and, thus, even be prevented, providing a promising approach for prophylactic surfactant therapy 11, 25, 26. However, there are no systematic studies comparing pre-ischaemic surfactant treatment with application during or after ischaemia in the same experimental setting. The current authors hypothesised that the timing of exogenous surfactant application in relation to the onset of ischaemia influences the structural preservation of the lung.
Therefore, the present study was performed in order to determine the optimal timing for exogenous surfactant treatment of the donor lung. Using an extracorporeal I/R injury rat lung model, a combined light and electron microscopic approach and design-based stereology 27, 28, the extent to which intra-alveolar oedema and injury of the blood–air barrier occurred was investigated.
MATERIALS AND METHODS
Experimental setting
A total of 40 male Sprague Dawley rats (mean±sd body weight 371±57 g) were used in the study. All animals received humane care and were treated according to the Guide for the Care and Use of Laboratory Animals 29 and in compliance with the current German and Swiss laws. The bioethical committee of the district of Thuringia, Germany approved the experiments.
After intraperitoneal administration of pentobarbital (12 mg per 100 g body weight), the trachea was exposed and the animals were intubated endotracheally. Mechanical ventilation was initiated, providing room air at a tidal volume of 5 mL, 40 breaths·min−1, positive end-expiratory pressure of 3 cmH2O (0.3 kPa), followed by a median laparotomy and systemic heparinisation. Following this, a bilateral longitudinal thoracotomy and puncture of the pulmonary trunk were carried out. Flush perfusion of the lung was initiated with 24–27 mL Perfadex® (60 mL per kg body weight) at 4°C, maintaining a perfusion pressure of 20 cmH2O (2.0 kPa).
After that, the superior and inferior caval veins and the left azygos vein were clipped. Heart and lungs were excised en bloc with clamped trachea and stored ex situ in 30–40 mL preservation solution for 4 h at 4°C (i.e. ischaemia time). Lungs were treated with instillation of the exogenous surfactant preparation poractant alfa (Curosurf®, 200 mg/kg body weight; a kind gift from Nycomed Pharma GmbH, Linz, Austria) according to the experimental setting. Before instillation of exogenous surfactant, the lungs were once inflated at a pressure of 23 cmH2O (2.2 kPa) in order to recruit potentially collapsed regions of the lung 30. Surfactant drawn up in a syringe in a volume of 4–5 mL air was then carefully instilled via the tracheal cannula. The alveolar recruitment procedure was performed again to make sure that surfactant reached the alveolar regions of the lungs and normal ventilation was restarted afterwards. Post-experimental visualisation of histological lung sections was used to confirm the even distribution of exogenous surfactant in the lung. Extracorporeal reperfusion was performed using the extracorporeal heart–lung circuit described in detail by Fukuse et al. 31. In short, the circuit consisted of a reservoir, a temperature probe (for perfusate temperature monitoring), a roller pump to raise the perfusate to the oxygenators, a blood filter and two membrane oxygenators. A perfusion pool was used at 80 cmH2O (7.8 kPa) and a preload pool at 5 cmH2O (0.5 kPa). Mechanical ventilation was performed with a small animal respirator. The perfusate consisted of Krebs–Henseleit buffer, supplemented with bovine erythrocyte concentrate (haematocrit of 38–40%) for 60 min under the same ventilation conditions as mentioned above, using a quattro head roller pump (Mod-Reglo-Digital; Ismatec, Zurich, Switzerland).
Animals were randomly assigned to eight different groups (five animals per group). Experimental groups included: group 1, which received initial surfactant instillation, flush perfusion, ischaemia and reperfusion; group 2, which was flush perfused, followed by surfactant instillation at the end of ischaemia, and reperfusion; group 3, which was flush perfused, then stored under ischaemia and finally reperfused while a bolus of surfactant was applied after 20 min of reperfusion; and group 4, which was flush perfused, stored under ischaemia and reperfused without receiving surfactant. Additional groups included: group 5, which was flush perfused with 0.9% NaCl solution, followed by ischaemia and reperfusion as “worst case” control; group 6 was fixed in situ immediately after flush perfusion before excision as “no injury” control; group 7 was treated with surfactant prior to flush perfusion and fixation; and group 8 received surfactant before flush perfusion, followed by ischaemia (fig. 1⇓).

Overview of the experimental protocol. ▾: surfactant instillation; ▪: flush with perfadex; ░: ischaemia (4 h at 4°C); □: reperfusion (60 min at 37°C); ▒: flush with NaCl.
Measurement of functional data
Pulmonary arterial pressure (Ppa) and oxygenation were recorded during reperfusion as described previously 5. Perfusate oxygenation, defined as the difference between oxygen tension of the perfusate collected from the left atrium after oxygenation and of the deoxygenated perfusate of the pre-load pool, was used to assess the capability of gas exchange. Ppa was determined by a pressure transducer (Statham; PVB Medizintechnik, Kirchseeon, Germany).
Fixation, sampling and tissue processing
Fixation, sampling and tissue processing were performed as previously described 27, 32, 33. The left lung was fixed by vascular perfusion of a fixative containing 4% paraformaldehyde and 0.1% glutaraldehyde in 0.2 M HEPES buffer. Afterwards, the main bronchus and artery were clamped and the left lung was excised and stored in 4°C cold fixative.
The total lung volume was determined by fluid displacement. Then the lungs were embedded in agar and sectioned from apex to base using a tissue slicer into 9–12 tissue slices of 3 mm thickness. Systematic uniform random sampling was used to obtain representative tissue blocks for stereological analysis 27. Every other slice was used for light (LM) or transmission electron microscopy (TEM), respectively. For TEM, small specimens were sampled from the lung slices by overprojection of a transparent uniform point grid on each slice. Whenever a point hit a lung slice a tissue sample was taken at the given location and stored in the fixative for ≥24 h.
For LM, the slices were postfixed in osmium tetroxide, washed again in sodium cacodylate and distilled water, immersed in half-saturated aqueous uranyl acetate overnight, dehydrated in ascending acetone concentrations and embedded in glycol methacrylate resin (Technovit 7100®; Heraeus Kulzer, Wehrheim, Germany) overnight. From the embedded tissue blocks, sections of 1 μm thickness were cut, mounted on glass slides and stained with methylene blue.
For TEM, the tissue blocks were postfixed in osmium tetroxide, stained en bloc in half-saturated aqueous uranyl acetate, dehydrated in an ascending acetone series and, finally, embedded in an epoxy resin (Araldite®; Serva Electrophoresis, Heidelberg, Germany; polymerisation: 5 days at 60°C). Ultra-thin sections of 40–70 nm thickness were obtained from the tissue blocks and stained with lead citrate and uranyl acetate using Ultrostainer (Leica, Bensheim, Germany).
Stereological analysis
Design-based stereological methods were used to analyse the lung samples and obtain the quantitative data 27, 28, 34.
LM analyses were carried out using an Axioscope light microscope (Zeiss, Oberkochen, Germany) and a computer-assisted stereology system (CAST 2.0; Olympus, Ballerup, Denmark). Systematic uniform random sampling produced representative test fields for further estimations, and a point grid with defined number of test points was projected onto the slices. Subsequently the volume densities (Vv) were estimated by counting the points hitting a structure, (Pstr), and the points hitting the reference space, (Pref), with Vv(str/ref) equal to Pstr/Pref. Following this, the volume densities were converted to the total lung volume by multiplication with the reference volume, according to equation 1. 
TEM was performed using an EM 900 (Zeiss, Oberkochen, Germany), supplemented with a digital camera (Megaview III; Soft Imaging System, Münster, Germany) and an image analysis software (AnalySIS 3.1; Soft Imaging System). Systematic uniform random sampling was applied to the ultra-thin sections, and digital micrographs were taken at a final magnification of ×20,000 whenever a test field included thin parts of the blood–air barrier. A test system consisting of parallel line segments and points was superimposed. By point and intersection counting, the arithmetic mean barrier thickness (τ̄) of the alveolar epithelium, interstitium and capillary endothelium was estimated according to equation 2, in which lT is the length of a test line, Pb is the number of points hitting a barrier profile and Ib is the number of intersections of the test lines with the reference surface of the barrier 27, 28: 
In order to obtain further information about the extent to which the blood–air barrier was affected, semiquantitative characterisation of the barrier was also performed. Three different categories were defined as follows. 1: normal, with the alveolar epithelium and capillary endothelium presenting normal electron-dense ultrastructure and a thin interstitium; 2: swollen, with swelling of endothelial and/or epithelial structures in one or more parts of the blood-air barrier; 3: fragmented, with disruptions of alveolar epithelium and/or capillary endothelium and denudation of the basement membrane. Therefore, a blood–air barrier integrity index was estimated. The surface area fractions of normal, swollen and fragmented alveolar epithelium were estimated by relating the number of intersections of one category to the total number of intersections with the blood–air barrier 5.
The sampling and counting was designed to obtain between 100 and 200 uniformly randomly distributed counting events per lung for each parameter. This ensures that the total observed variability is dominated by the biological variability between animals and not by the variability due to the stereological procedure 34.
Statistics
Data are given as mean±sd. Stereological data were analysed as follows: according to the overall hypothesis of the study, comparison of the experimental groups 1–4 was performed using Kruskal–Wallis one-way ANOVA on ranks. If p<0.05, those groups that contributed to the overall intergroup differences were isolated by the all pairwise multiple comparison procedure (Student–Newman–Keuls method). Control groups were compared with the corresponding experimental group (i.e. group 5 versus group 4, group 6 versus group 7, and group 8 versus group 1) by the Whitney–Mann U-test. Functional data between groups were analysed by one-way ANOVA, and subsequently Tukey B or Tamhane test. Differences between groups were considered statistically significant at p<0.05.
RESULTS
Perfusate oxygenation and pulmonary arterial pressure
Perfusate oxygenation was significantly higher in group 1 than in groups 2–4 at 20, 40 and 50 min. It was also significantly higher than groups 2 and 4 at 30 min, and showed a tendency to be higher than group 3 at 30 min. There were no significant differences in perfusate oxygenation between groups 2–4 at any point in time. The mean Ppa was similar in groups 1–4 and did not show any significant difference at any point in time (fig. 2⇓).
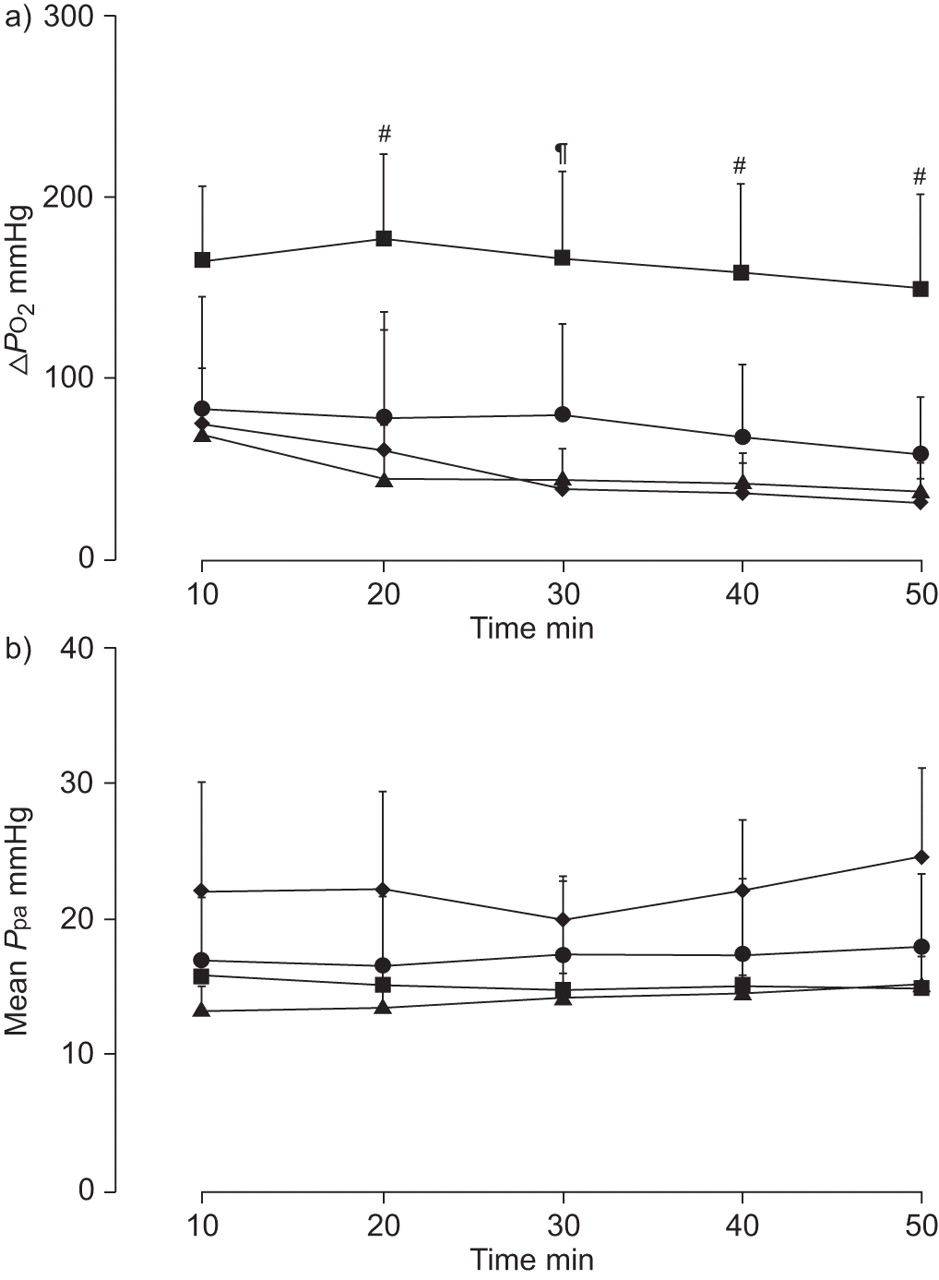
Perfusate oxygenation (ΔPO2) and mean pulmonary arterial pressure (Ppa). ▪: group 1; ▴: group 2; •: group 3; ♦: group 4. #: p<0.05 versus groups 2–4; ¶: p<0.05 versus groups 2 and 4. 1 mmHg = 0.133 kPa.
Qualitative LM and TEM
The lung tissue in all LM and TEM sections showed only few atelectatic areas and small amounts of erythrocytes left in capillaries and alveolar lumen, whereas most blood vessels were opened widely. Groups treated with surfactant instillation (i.e. groups 1–3, 7 and 8) presented similarly abundant amounts of surfactant in the alveoli compared with the untreated groups, verifying that the applied substance effectively reached its intended destination. The no injury control group (6) showed normal parenchymal lung structure and free airspaces without intra-alveolar oedema or erythrocytes. In general, these structural findings clearly indicate that the perfusion fixation of the lung tissue was performed successfully, leaving only very few structural alterations that might be due to the experimental procedure (fig. 3⇓).

Light micrographs showing lung histology in groups 1 (a), 2 (b), 3 (c), 4 (d), 5 (e), 6 (f), 7 (g) and 8 (h). Surfactant treatment before ischaemia and reperfusion (a) diminished intra-alveolar oedema (Ed) formation and extravasation of erythrocytes (Ery; compare b–e), resulting in a structural preservation close to the no injury control groups without (f) and with (g) surfactant (Surf). Scale bars = 100 μm.
In the ischaemia and reperfusion treated groups (1–5), pronounced evidence for ultrastructural injury could be detected. The extent of injury depended on whether, and when, surfactant was applied. In the non-ischaemia groups 6 and 7, lung ultrastructure was widely intact and signs of injury were missing. Group 8, which was exposed to ischaemia but not to reperfusion, showed moderate lung damage due to ischaemic conditions (fig. 4⇓).

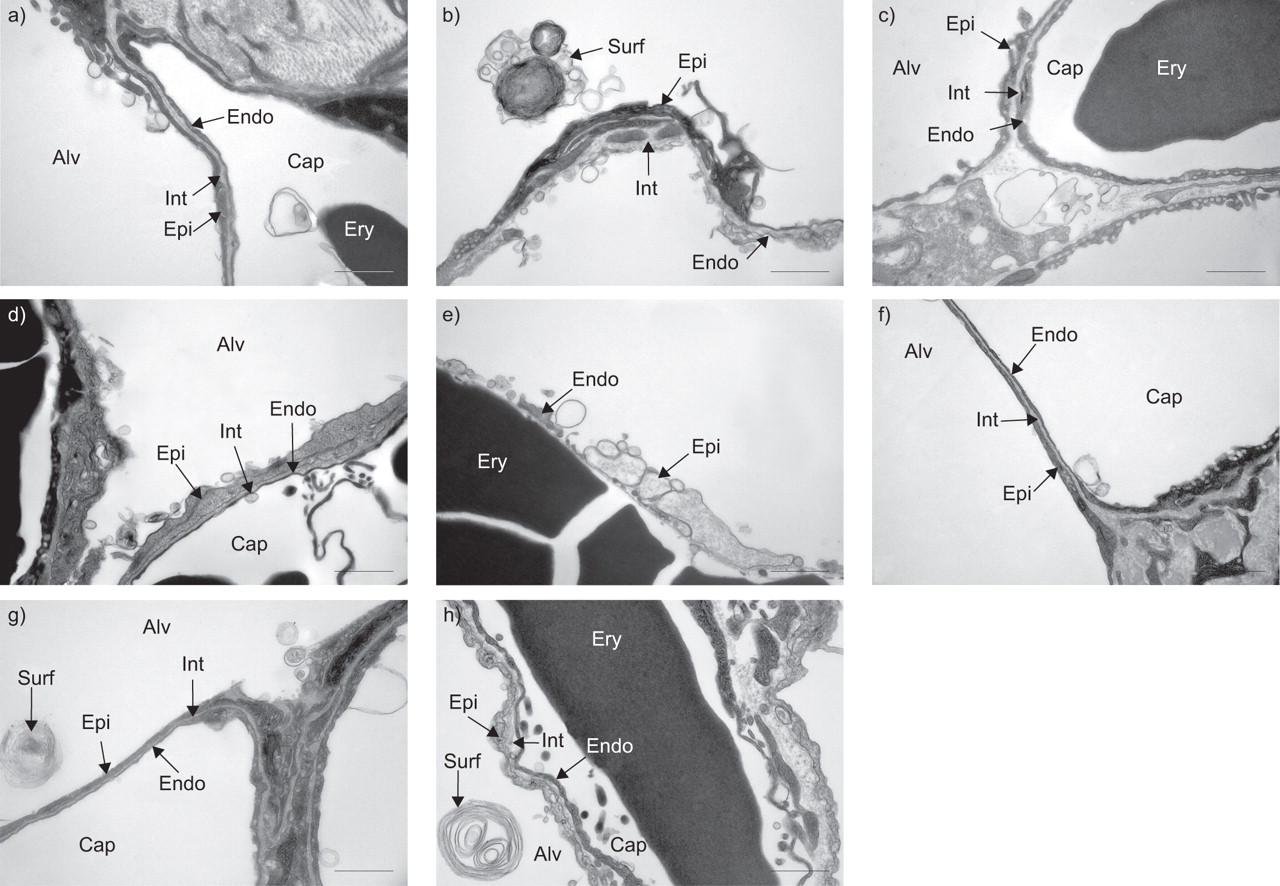
Electron micrographs showing blood–air barrier ultrastructure in groups 1 (a), 2 (b), 3 (c), 4 (d), 5 (e), 6 (f), 7 (g) and 8 (h). Surfactant treatment before ischaemia and reperfusion (a) diminished swelling and fragmentation of the components of the blood–air barrier (compare b–e), resulting in a structural preservation close to the no injury control groups without (f) and with (g) surfactant. Alv: alveolar lumen; Cap: capillary lumen; Ery: erythrocyte; Epi: alveolar epithelium; Int: interstitium; Endo: capillary endothelium; Surf: intra-alveolar surfactant. Scale bars = 1 μm.
Intra-alveolar oedema formations as well as extravascular accumulations of erythrocytes and blood–air barrier damage were found to a variable extent, but clear differentiation between groups required a formal quantitative, i.e. stereological approach.
Stereology
In order to quantify intra-alveolar oedema formation at the LM level, the volumes of oedema fluid, V(ed,lung), and intra-alveolar erythrocyte accumulation, V(ery,lung), were added to the total volume of intra-alveolar oedema, V(eryed,lung) (mL per lung). This parameter showed that intra-alveolar oedema formation appeared only slightly in groups 1 (0.01±0.01 mL) and 6 (0.01±0.04 mL), was pronounced in groups 2 (0.07±0.08 mL), 3 (0.03±0.03 mL) and 4 (0.20±0.23 mL), and was severe in group 5 (0.64±0.36 mL). In groups 7 and 8 no intra-alveolar oedema or erythrocytes were found (0.00±0.00 mL). Peribronchovascular oedema formation was estimated by the ratio of wall to luminal space of nonparenchymal vessels and airways, with groups 2–5 having a higher wall/lumen ratio than the other groups. However, these findings were not significant (table 1⇓).
Light microscopic results of stereological analysis
A blood–air barrier integrity index was determined for each group (fig. 5⇓), indicating that the alveolar epithelium was moderately swollen in groups 1 (1.80±0.14) and 8 (1.72±0.07), fragmented/swollen in groups 2 (2.20±0.35), 3 (1.98±0.15) and 4 (2.17±0.20) and almost normal in groups 6 (1.26±0.03) and 7 (1.33±0.08). Estimation of the arithmetic mean thickness of the blood–air barrier, τ̄(bab), resulted in the same sequence of groups, with groups 1 (367±44 nm) and 8 (400±71 nm) showing similarly moderate effects, groups 2 (518±83 nm), 3 (404±88 nm) and 4 (524±92 nm) with pronounced swelling, followed by group 5 being affected most (646±165 nm). In groups 6 (358±22 nm) and 7 (358±30 nm) no swelling of the blood–air barrier was present. The arithmetic mean thickness of the interstitial space, τ̄(int), of group 5 showed a significantly increased swelling compared with all other groups. Moreover, all groups exposed to ischaemia (i.e. groups 1–5 and 8) presented considerable swelling of the blood–air barrier, as distinct from the non-ischaemia groups (6 and 7) without swelling (table 2⇓).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Fraction of normal (□), swollen (▓) and fragmented (▪) surface of the blood–air barrier. Surfactant treatment before ischaemia and reperfusion (group 1) resulted in a decreased fraction of fragmented blood–air barrier surface (compare groups 2–5). The fraction of swollen blood–air barrier surface is comparable to the same treatment without reperfusion (group 8). Only mild swelling was present due to the experimental procedure (groups 6 and 7).
Electron microscopic results of stereological analysis
Altogether, the results of the present study demonstrate that surfactant instillation attenuates ultrastructural injury in lungs subjected to ischaemia and reperfusion, especially when applied prior to the period of ischaemia.
DISCUSSION
In human lung transplantation, I/R injury-caused PGD is a dreaded complication, remaining a significant cause of short- and long-term morbidity and mortality 1, 3, 4. The clinical manifestation of I/R injury includes oedema formation, an increase in Ppa and hypoxaemia and ranges from mild ALI to severe ARDS 1, 10. Several studies have identified the important role of surfactant alterations in transplantation-related I/R injury of the lung 8, 9, 35–40. Accordingly, exogenous surfactant therapy has been applied successfully in experimental 12–21 and clinical 22–24 studies. It is, therefore, considered a potentially promising therapy for the mitigation of severe lung I/R injury, although the optimal surfactant preparation and mode of therapy still need to be determined 26, 41.
In lung transplantation, surfactant can be given before organ retrieval, i.e. it is one of the few situations in which it can be applied prophylactically 11. Previous experimental studies have indicated beneficial effects of surfactant treatment for graft lung function, especially when applied before ischaemia 12, 16. In addition, experimental evidence has shown that improvement of the endogenous surfactant system via application of keratinocyte growth factor successfully decreases transplantation-associated I/R injury in rats 42. A recent clinical study has also suggested that exogenous surfactant therapy of donor lungs before retrieval protects post-transplantation surfactant function 23. However, there are no systematic studies comparing pre-ischaemic surfactant treatment with application during ischaemia or during reperfusion in the same experimental setting. Moreover, the structural correlate of successful surfactant therapy is not known. Therefore, the aim of the present study was to systematically define the optimal time point for exogenous surfactant instillation in I/R injured lungs using a combined LM and TEM and stereological approach. An established extracorporeal rat lung I/R injury model was used in the study, including the whole sequence of transplantation-related events, namely flush perfusion, cold ischaemic storage and subsequent reperfusion 5, 8, 9. A limitation of this model is that it is not a real transplantation model. Therefore, effects resulting from the interaction between donor and host cannot be investigated. Perfadex® was used as preservation solution for its proven efficacy in previous studies 6, 43, 44, except for in one group, which was flush perfused with NaCl to induce severe I/R injury. With regard to the surfactant preparation, it was decided that Curosurf® derived from porcine lung tissue would be used, which contains the hydrophobic surfactant proteins B and C, and which is routinely applied for the treatment of neonatal respiratory distress syndrome 45. In the analysis, the current authors focused on the stereological estimation of intra-alveolar oedema formation and the ultrastructural integrity of the blood–air barrier, as well as perfusate oxygenation and pulmonary arterial pressure. It has been previously shown by quantitative stereological assessment that the degree of ultrastructural injury is functionally relevant in lung I/R injury as it closely correlates with post-ischaemic lung function 5, 8, 9. Additionally, impaired oxygenation is one of the main features of PGD 1; therefore, improvement of perfusate oxygenation levels, as observed after pre-ischaemic surfactant therapy, strongly confirms the stereological data in the current study.
Intra-alveolar oedema formation is a hallmark of I/R injury, resulting in an increased barrier thickness for pulmonary gas exchange. According to Fick's law of diffusion, the development of intra-alveolar oedema reduces the oxygenation capacity of the lung. The current authors used design-based stereological methods in order to quantify the degree of oedema formation in its preserved micro-organisation and localisation within the organ. These parameters are more sensitive indicators for impaired lung function and better correlate with the respiratory capacities of the organ than the wet-to-dry ratio 5, 9, 46. This high sensitivity is important since, in the present study, the amount of intra-alveolar oedema is rather low. A previous direct structural–functional correlation study demonstrated that with a volume fraction of >3%, intra-alveolar oedema formation becomes functionally relevant 46. In the present study, only the two reperfused groups that did not receive surfactant had an intra-alveolar oedema volume fraction >3% of the parenchymal volume: group 4 (3.6%) and group 5 (7.9%; table 1⇑). In addition, the perfusate oxygenation is significantly better in group 1 than in groups 2–4, which strongly underlines the stereological data. Accordingly, the present study shows that exogenous surfactant therapy, especially when applied pre-ischaemically, effectively attenuates intra-alveolar oedema formation, and so contributes to improved lung preservation and the prevention of I/R injury.
I/R injury also leads to disintegration of the blood–air barrier, including swelling of the interstitium and swelling or fragmentation of epithelial and endothelial cells 5, 6. Estimation of the arithmetic mean barrier thickness by electron microscopy yields information on the extent of interstitial, as well as epithelial and endothelial, oedema formation 6. The estimation of a blood–air barrier integrity index, as an established method for quantifying the ratio of normal, swollen and fragmented parts of the blood–air barrier, provides important information on the degree of lung damage 5, 6. Based on this approach, the present results suggest that pre-ischaemic surfactant instillation is superior to application during or after ischaemia with respect to the attenuation of blood–air barrier injury (fig. 5⇑); however, these data do not reach statistically significant levels.
In conclusion, the present study provides quantitative morphological and functional evidence that surfactant application significantly attenuates ischaemia/reperfusion injury by reducing intra-alveolar oedema formation and blood–air barrier injury and improving perfusate oxygenation. This observation was most pronounced when surfactant was administered before the onset of ischaemia, a finding that offers a rationale for pretreatment of the donor lung with surfactant in lung transplantation in order to improve lung preservation quality.
Support statement
This work was funded by the Deutsche Forschungsgemeinschaft (DFG Oc 23/8-1 and Wa 738/8-1).
Statement of interest
A statement of interest for this study can be found at www.erj.ersjournals.com/misc/statements.shtml
Acknowledgments
The authors gratefully acknowledge the technical assistance of S. Freese, H. Hühn, S. Kosin and S. Wienstroth (Dept of Anatomy, University of Göttingen, Göttingen, Germany), and V. Gaschen, B. Haenni and B. Krieger (Institute of Anatomy, University of Bern, Bern, Switzerland).
- Received February 15, 2008.
- Accepted October 23, 2008.
- © ERS Journals Ltd
References










