





To the Editors:
Nitric oxide (NO) is a free radical generated from l-arginine through the NO synthases (NOS). This molecule is produced within the respiratory tract and plays an important role in airway pathophysiology, exerting both beneficial and nonbeneficial effects 1, 2.
Because various pro-inflammatory mediators and lipopolysaccharides are capable of inciting inducible NOS (iNOS) expression 2, different airway inflammatory diseases are associated with increased NO release, which is detectable in exhaled gas, including asthma 3, bronchiectasis 4, allergic rhinitis 5 and upper respiratory tract infections 6. However, not all sources of the elevated exhaled NO (eNO) have been identified as yet. Interestingly, it has been suggested that iNOS expression and formation of peroxynitrite may play an important role in the pathogenesis of recurrent tonsillitis 7. To investigate whether recurrent tonsillitis is associated with increased levels of eNO, we measured oral eNO levels in adult patients with a history of frequent tonsillitis episodes.
The study group consisted of 32 nonatopic, nonsmoking patients with recurrent tonsillitis, scheduled for tonsillectomy (18 females; median (range) age 28 (18–50) yrs). All patients had a history of frequent episodes of tonsillitis over many years. All patients had received antibiotic treatment >1 month prior to surgery. Specific exclusion criteria were diseases that may affect eNO concentration, including asthma, rhinitis and sinusitis. Routine histological examination of tonsillectomy was performed for each of the cases.
A total of 35 nonatopic, nonsmoking healthy subjects (20 females; age 30 (18–49) yrs) were included in the control group. Oral eNO levels were measured in triplicate using the Niox Mino® analyser (Aerocrine AB, Solna, Sweden). The level of NO is expressed in ppb.
Statistical analysis was performed using the Mann–Whitney U-test. A p-value <0.05 was considered significant.
eNO levels were significantly higher in patients with recurrent tonsillitis (21.0 (6.0–50.0) ppb) than in normal controls (17.0 (5.0–26.0) ppb; p<0.05; fig. 1⇓). This suggests that recurrent tonsillitis may increase the level of NO in exhaled air. eNO can be a sensitive marker of inflammation in the respiratory tract but is not specific for asthma, as increased levels of oral eNO have been observed in other diseases, including infections of the upper respiratory tract 6. However, NO levels did not differ between healthy subjects and common cold patients, and were significantly lower in patients suffering from chronic sinusitis 8 as well as from acute sinusitis 9.
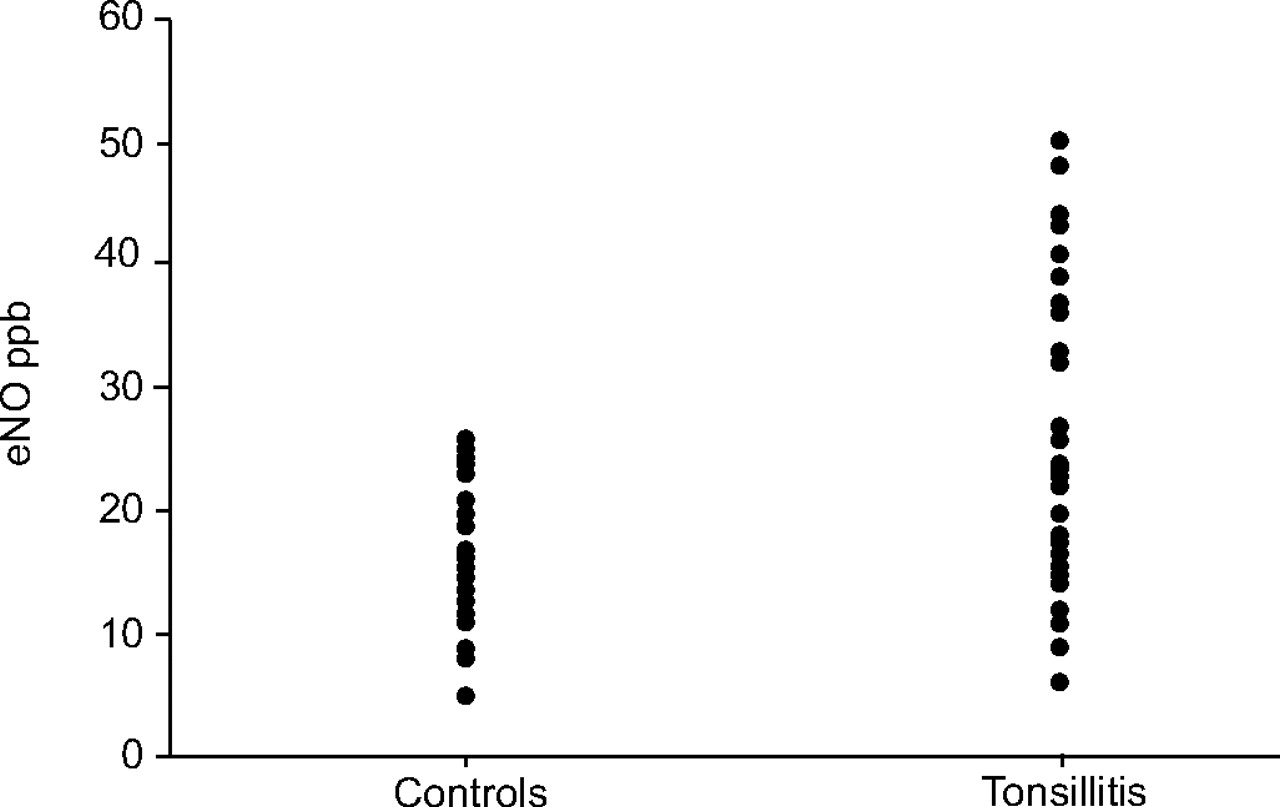
Exhaled nitric oxide (eNO) in patients suffering from recurrent tonsillitis and healthy subjects.
The present study was the first to show that, to the best of our knowledge, oral exhaled nitric oxide can be elevated in patients with recurrent tonsillitis, probably as a result of the increased production of nitric oxide formed by inducible nitric oxide synthase in tonsillar tissue resulting from inflammation. The potential inflammatory role of the l-arginine–nitric oxide pathway in the pathogenesis of chronic/recurrent tonsillitis and chronic adenotonsillar hypertrophy has been suggested 7, 10. An extended study to consider patients after the therapy (tonsillectomy) should be the subject of future investigations.
Statement of interest
None declared.
- © ERS Journals Ltd











{kind=link}