





Abstract
Evidence-based recommendations on the clinical use of cardiopulmonary exercise testing (CPET) in lung and heart disease are presented, with reference to the assessment of exercise intolerance, prognostic assessment and the evaluation of therapeutic interventions (e.g. drugs, supplemental oxygen, exercise training). A commonly used grading system for recommendations in evidence-based guidelines was applied, with the grade of recommendation ranging from A, the highest, to D, the lowest.
For symptom-limited incremental exercise, CPET indices, such as peak O2 uptake (V′O2), V′O2 at lactate threshold, the slope of the ventilation–CO2 output relationship and the presence of arterial O2 desaturation, have all been shown to have power in prognostic evaluation. In addition, for assessment of interventions, the tolerable duration of symptom-limited high-intensity constant-load exercise often provides greater sensitivity to discriminate change than the classical incremental test. Field-testing paradigms (e.g. timed and shuttle walking tests) also prove valuable.
In turn, these considerations allow the resolution of practical questions that often confront the clinician, such as: 1) “When should an evaluation of exercise intolerance be sought?”; 2) “Which particular form of test should be asked for?”; and 3) “What cluster of variables should be selected when evaluating prognosis for a particular disease or the effect of a particular intervention?”
The purpose of this document is to present recommendations on the clinical use of exercise testing in patients with cardiopulmonary disease, with particular emphasis on the evidence base for the functional evaluation, prognosis and assessment of interventions. While the scope of the document is broad, consideration will focus only on those indices that have demonstrable predictive power. Supplemental references will therefore be included, where appropriate.
Exercise intolerance can be defined as an inability to complete a required physical task successfully. In one sense, therefore, everyone who exercises has, at some level(s), “exercise intolerance”. From a clinical perspective, the issue is whether a patient demonstrates intolerance to a task that normal subjects would find tolerable. However, exercise intolerance (often considered in terms of peak oxygen uptake (V′O2,peak)) in pulmonary and cardiac disease patients cannot be confidently predicted from physiological variables, determined at rest, such as forced expiratory volume in one second (FEV1), pulmonary diffusing capacity for carbon monoxide (DL,CO), ejection fraction (EF) or body mass index (BMI). It is necessary, therefore, to actually assess an individual's exercise intolerance and, where possible, establish its cause(s). This task-specificity imposes technical challenges: the requirement to be able to impose particular work-rate protocols in an accurate and reproducible fashion largely confines assessment to ergometric devices, such as cycle ergometers and treadmills. While these represent a less-than-ideal approximation to the realities of daily exercise, they provide a precise and controlled focus for assessing the appropriateness of the interaction among the contributing physiological support systems.
Cardiopulmonary exercise testing (CPET) should be considered the gold standard for evaluating the causes of exercise intolerance in patients with pulmonary and cardiac disease, and is based on the principle that system failure typically occurs while the system (e.g. muscle–energetic, cardiovascular or pulmonary) is under stress. CPET comprises the imposition of symptom-limited incremental exercise, commonly in combination with comprehensive breath-by-breath monitoring of cardiopulmonary variables (e.g. V′O2, pulmonary CO2 output (V′CO2), minute ventilation (V′E), cardiac frequency (fC)), perceptual responses (e.g. dyspnoea, leg discomfort) and, as needed, measurements such as exercise-related arterial oxygen desaturation, dynamic hyperinflation and limb-muscle strength. Thus, the support systems are “forced”, normally over their tolerable range, in a controlled way that allows key system responses to be expressed relative to an appropriate frame of reference (e.g. V′E being expressed relative to V′CO2) and indices of aerobic function (e.g. lactate threshold (θL), V′O2,peak) to be discriminated confidently. Previous European Respiratory Society and American Thoracic Society (ATS)/American College of Chest Physicians statements have provided useful recommendations on the standardisation of CPET in clinical practice 1–3.
While a wide variety of tests is available, each being more or less suitable as a stressor of a particular component of a patient's pathophysiology, the appropriateness of the integrated physiological-system response is best studied (certainly, for initial exercise evaluation) by means of a symptom-limited incremental test. This is typically established by means of a progressive increase in work-rate by a small fixed increment at a fixed frequency (e.g. each minute or less), in a “staircase” fashion, or when work-rate is increased incrementally under computer control as a smooth continuous ramp both with cycle-ergometry 1, 3–5 and, more recently, for the treadmill 6. However, high-intensity constant-load tests are also becoming widely used as, in many instances, they provide a sensitive discrimination of improved function consequent to an intervention.
System function can be well described through a range of appropriately selected responses to incremental and/or high-intensity constant-load exercise. These may represent values of variables at certain reference points within the tolerable range of the test or response profiles over selected regions of interest. Assessing the normality, or otherwise, of such system responses requires the investigator to select, and display appropriately, the cluster of response variables that are best reflective of the behaviour of the particular system(s). Discrimination of the magnitude and/or pattern of deviation from the normal response of the age-, sex- and activity-matched “standard” subject can then be attempted, and the magnitude or pattern of abnormality matched with that characteristic of the specific physiological system(s) that is/are dysfunctional. In some instances, appropriate normal values may not be readily available. In others, values may be modality-dependent (e.g. greater muscle mass involved in treadmill exercise results in a slightly higher V′O2,peak).
However, although there is widespread clinical use of CPET, it is not considered to provide a substantial improvement in primary diagnostic power (i.e. with respect to the basic category of abnormality) over more classical clinical tools such as spirometry and electro- and echo-cardiography. What CPET can do, however, is provide considerable “fine tuning” of these considerations, by: 1) revealing specific abnormalities that occur only when support systems are stressed by physical activity (e.g. dynamic hyperinflation in chronic obstructive pulmonary disease (COPD) or increased ventilatory response in chronic heart failure (CHF)); and 2) providing a functional frame of reference for assessing the efficacy of interventions targeted to ameliorate such abnormalities (e.g. bronchodilators for dynamic hyperinflation or vasodilators for heart failure).
With the more recent recognition that improved functional status following an intervention such as exercise training in patients with chronic lung disease does not always manifest itself in appreciable increases in classical performance indices such as V′O2,peak, the scope of CPET has been expanded to include laboratory-based high-intensity constant-load exercise paradigms performed to the limit of tolerance (tlim), which can provide a more sensitive frame of reference especially in the context of prognosis and intervention. Field-testing paradigms, such as timed and shuttle walking tests, are also becoming popular, often supported by measurements of variables such as arterial oxygen saturation (Sp,O2, used here in preference to the more conventional abbreviation Sa,O2, to reflect the fact that during exercise it is most commonly measured noninvasively using pulse oximetry), fC and exertional symptoms. What is perhaps not so widely recognised is that such tests can be viewed constructively in the context of the “power–duration relationship” for constant-load symptom-limited exercise. Finally, the use of CPET is becoming more widespread both prognostically and for the evaluation of interventions such as oxygen supplementation, exercise-based rehabilitation and drug therapies.
This document is therefore intended to provide the answers to three fundamental questions often faced by clinicians: 1) “When should an evaluation of exercise intolerance be sought?”; 2) “Which particular form of test should be asked for?”; and 3) “What cluster of variables should be selected when evaluating prognosis for a particular disease or the effect of a particular intervention?”. This is accomplished through critical evaluation of CPET outcomes in the context of diagnosis, prognosis and pertinent interventions, with the underlying physiological principles being presented in supplementary material online.
UTILITY OF CPET IN DIAGNOSIS AND FUNCTIONAL EVALUATION
What additional diagnostic and/or prognostic information can be expected to arise from CPET in a particular patient? CPET can: provide an objective measure of exercise capacity; identify the mechanisms limiting exercise tolerance; establish indices of the patient's prognosis; and monitor disease progression and/or the response to interventions. What CPET cannot uniquely do is affect diagnosis, except in very specific conditions, such as exercise-induced bronchoconstriction and arterial oxygen desaturation. In most instances, the patient to be studied will have already presented with a primary diagnosis. However, where CPET can be valuable is in differential diagnosis; for instance, profiles of judiciously selected cardiopulmonary and gas-exchange response can distinguish between pulmonary and cardiac limitations to exercise. The interpretative power of CPET can be strengthened by incorporating additional measurements. In a patient with a primary diagnosis of COPD, for example, these typically include habitual physical activity levels, body mass and composition, muscle strength, exercise-related arterial desaturation, dynamic hyperinflation and exacerbation of symptoms. Importantly, CPET should be viewed as a key adjunct to a previous comprehensive medical evaluation comprising a medical history and examination and, depending on what is suspected, other complementary tests and measurements (e.g. haematocrit, biochemistry, resting electrocardiogram, chest radiography, arterial blood-gas analysis, resting pulmonary function testing). The nature and extent of the medical evaluation prior to exercise testing should be focused on narrowing the range of suspected diseases.
Exercise intolerance
Measurement of V′O2,peak (see section 1.1 and fig. 1⇓, both in supplementary material) is highly reproducible in healthy asymptomatic subjects who are well motivated during the exercise test. This has also been shown to be the case in situations where exercise is symptom-limited 7–10, which is important in contexts such as disability benefits claims or exercise prescription when a patient complains of breathlessness or exercise intolerance. In certain diseases, such as COPD and CHF, where it is preferable that the index of exercise intolerance relates more closely to activities of daily living, walking tests such as the 6-min walking test (6-MWT) 11, 12 are commonly used. As is the case for CPET, reproducibility requires that standardised procedures are adopted.
Causes of exercise intolerance
The causes of exercise intolerance can broadly be classed as “central” (“Could, but won't”) and “peripheral” (“Would, but can't”). The classical criterion for defining exercise intolerance and classifying degrees of impairment is V′O2,peak standardised by body mass 13. As factors such as habitual physical activity, age, sex and height influence V′O2,peak (see supplementary material, 1.1) and distance walked on the 6-MWT (6-MWD) 14–16, it is recommended that the normalcy (or otherwise) of exercise capacity be judged relative to reference values for matched healthy populations, taking into account not only body mass but, in certain conditions, also fat-free mass (see supplementary material, 1.1). Values >1.96 times the sd should be considered abnormal with a confidence of 95%.Values <40% predicted indicate severe impairment 17.
CPET in the identification of the causes of exercise intolerance
There are several CPET response patterns that are not disease-specific but nonetheless point to particular sites of system dysfunction, thereby narrowing the differential diagnosis (c.f. fig. 2⇓ in supplementary material). The absence of these response patterns can be taken as evidence against a significant involvement of these systems in exercise limitation. Although the exact mechanisms of exercise limitation in individuals without known disease are difficult to establish, ventilatory limitation is usually unlikely as there is still a significant breathing reserve at peak exercise (see supplementary material, 1.6) 17. Furthermore, a decreased arterial carbon dioxide tension (Pa,CO2) at end-exercise implies respiratory compensation for metabolic acidosis (see supplementary material, 1.3 and 1.5) as, despite some widening of the alveolar–arterial oxygen difference (PA−a,O2), arterial oxygen tension (Pa,O2) and Sp,O2 are not appreciably different from resting values 18. With good subject effort, if V′O2,peak is above the lower limit of the 95% confidence interval (i.e. “normal” V′O2,peak) and the subject indicates that either dyspnoea or leg fatigue was the reason for stopping exercise, then the subject is frequently deemed to have a normal exercise tolerance. This scenario would effectively exclude significant COPD or interstitial lung disease (ILD) 19, 20, CHF 21 and pulmonary vascular disorders (PVD) 22 as causes of the exercise intolerance. However, while the finding of a normal V′O2,peak may be helpful in providing reassurance to the patient and in limiting subsequent testing, it is important to recognise that normal in this context actually means “what is to be expected for relatively sedentary subjects” (i.e. characteristic of the group from which the normal value derives). So a normal V′O2,peak in a subject with a high activity level, or one who has previously been highly fit, should not necessarily be viewed as reflecting the absence of an abnormality.
For patients with unexplained exercise intolerance for whom initial test results (e.g. spirometry and echocardiography) are non-diagnostic, CPET may represent a useful tool in identifying whether the exercise intolerance is due to abnormalities in the oxygen transport pathway (extending from atmospheric air to the mitochondria in muscle), deconditioning or psychological factors (hyperventilation, panic, anxiety syndromes, etc.). Response patterns may not be diagnostic of specific aetiology but, together with previous medical evaluation, they can help to direct further diagnostic testing 4, 23–26.
Abnormal oxygen delivery
This term encompasses several heterogeneous conditions that have in common a reduced systemic oxygen delivery (i.e. the product of cardiac output and arterial oxygen content) during exercise, relative to metabolic demands. These are characterised by a low V′O2,peak and low θL (see supplementary material, 1.1 and 1.3). fC reserve is also frequently low, although if symptoms force the patient to quit early, fC reserve will be high (see supplementary material, 1.4). In most cases, peak O2 pulse is low and the fC–V′O2 slope is steep 27–29 and, with significant systolic or diastolic heart failure, the O2 pulse plateaus early in the test (see supplementary material, fig. 4⇓) 30. The finding of O2 pulse increasing normally until a point and then decreasing, with a corresponding increase in the fC–V′O2 slope, is relatively specific to coronary artery disease 31.
Ventilatory limitation to exercise
Ventilatory limitation at peak exercise, which is usually observed in obstructive lung diseases (see fig. 6 in supplementary material) and may also be seen in restrictive lung diseases, is judged to occur when V′E/maximum voluntary ventilation (MVV) exceeds 85% 17, particularly if respiratory compensation for metabolic acidosis is not evident, i.e. Pa,CO2 being increased 32 or normal with a high dead space fraction of the breath (dead volume/tidal volume; VD/VT). A low breathing reserve may also be seen in endurance ahletes and fit elderly people, for whom V′O2,peak is above the normal age-matched range (see supplementary material, 1.6).
Abnormal ventilatory control
It is important to emphasise that the profile of ventilatory response to exercise cannot be predicted from resting lung function; it must be measured. The appropriate frame of reference for V′E is V′CO2 (see supplementary material, 1.5), and it will emerge that the V′E–V′CO2 slope and the ventilatory equivalent for CO2 (V′E/V′CO2) at θL are important in diagnosis, prognosis and evaluation of interventions. Abnormal ventilatory control during exercise is defined as an inappropriately high (hyperventilation, i.e. low carbon dioxide tension (PCO2) set-point) or low (hypoventilation, i.e. high PCO2 set-point) V′E–V′CO2 slope. The defect may be primary (i.e. not attributable to any specific disease or known mechanism) or secondary (i.e. secondary to hypoxia, or other influences in respiratory or cardiac diseases that can stimulate V′E).
In primary hyperventilation, there is a marked hyperventilation at rest with metabolic compensation being more or less complete. The hyperventilation is maintained during exercise, i.e. with abnormally large increases in V′E and an elevated V′E–V′CO2slope 33–35. However, as an increased V′E–V′CO2 slope can reflect an increased VD/VT as well as a reduced PCO2 set-point, simultaneous Pa,CO2 monitoring is needed to rule out the former. Pa,CO2 typically remains depressed during exercise 35, although there have been reports that Pa,CO2 may increase towards normal levels when exercise is intense enough for automatic mechanisms of control to override the presumed corticogenic drive 4. In some patients, exercise-induced bronchoconstriction (EIB) may be the cause of exercise hyperventilation 36. In addition, in subjects with normal coronary arteries, hyperventilation during exercise has been associated with ECG changes resembling ischaemia 37.
Secondary hyperventilation during exercise (with a reduced Pa,CO2) is proposed to result from hypoxaemia-induced stimulation of peripheral (carotid) chemoreceptors, cardiopulmonary mechanoreceptor activity (ILD, PVD) and/or muscle mechano- or chemoreceptor activation (e.g. CHF) 20, 22, 38–43.
Primary hypoventilation is defined as an abnormally low increase in V′E relative to V′CO2 (i.e. reduced V′E–V′CO2 slope) with CO2 retention in the absence of a recognisable pulmonary disease 44–46. Secondary hypoventilation is frequently observed in COPD 19, 32, and may also be seen in advanced ILD 20 and neuromuscular diseases 47. It is important to point out that when exercise hypoventilation occurs in COPD and ILD, V′E may, seemingly paradoxically, be higher than normal at a given V′CO2 despite CO2 retention; this reflects the influence of an elevated VD/VT.
Pulmonary gas exchange abnormalities
The efficiency of pulmonary gas exchange is conventionally judged by the magnitude of PA−a,O2, and knowledge of how this changes during exercise can be useful in evaluating the severity of many lung and heart diseases. The behaviour of PA-a,O2 during exercise cannot be predicted from resting lung function; it has to be measured. Normally Pa,O2 does not decrease during exercise and PA-a,O2 at peak exercise remains below 2.66–3.99 kPa (20–30 mmHg) 48, 49. A PA-a,O2 >3.99 kPa (30 mmHg) at peak exercise is defined as abnormal and is commonly accompanied by arterial desaturation (i.e. Sp,O2 <88%). Pa,O2 ≤7.32 kPa (55 mmHg) is usually considered clinically significant, and may limit exercise tolerance with the potential to endanger the subject. This is seen in most patients with ILD and PVD, in many patients with moderate and severe COPD 50–54, and less frequently in patients with intracardiac left-to-right shunting or chronic heart failure 4. Interestingly, it can also be seen in elite endurance athletes (see supplementary material, 1.8).
Muscle metabolic dysfunction
There are many sites within skeletal muscle metabolic pathways whose dysfunction can result in exercise intolerance (reduced V′O2,peak and θL), ranging from routes of substrate delivery and utilisation to energy transformations themselves. The detection of such impairments is beyond the scope of conventional CPET and relies on interventions such as muscle biopsy and noninvasive muscle nuclear magnetic resonance spectroscopy and imaging (the interested reader is referred to 55–58 for further discussion).
As one of the more commonly affected processes is mitochondrial oxygen consumption, in general terms, the exercise response pattern is similar to that for conditions grouped under the heading of abnormal oxygen transport. In the absence of evident cardiopathy, anaemia or carboxyhaemoglobinaemia, muscle myopathic disease is suggested. However, milder forms of myopathy as well as significant muscle deconditioning (see later) may be difficult to differentiate from mild cardiovascular disease. Patients with metabolic myopathies may also present with muscle pain during or after exhausting exercise 41, 43, 59 or with cramps during exercise (myoadenylate deaminase deficiency) 60.
Deconditioning
Patients with a sedentary lifestyle may complain of exercise intolerance. Unless the sedentarity is marked, V′O2,peak may be normal or only mildly decreased. A cardinal sign of deconditioning is a leftward shift and steepening of the fC–V′O2 relationship and a shallower O2 pulse profile (see supplementary material, 1.4), although peak fC can be normal (if care is taken to motivate the subject during the test) with consequently little or no fC reserve. Because of the low V′O2,peak, there is usually significant breathing reserve. Pa,O2and VD/VT responses are normal. Deconditioning is often difficult to distinguish from mild heart disease, but if the medical history shows no evidence of disease, it is reasonable attribute the exercise intolerance solely to deconditioning.
Excessive perception of symptoms
In some individuals with exercise intolerance, the only finding is a disproportionate or exaggerated perception of symptoms (e.g. dyspnoea, leg effort) with no evident physiological abnormality 61. This condition constitutes a problem in clinical practice often requiring further explanation. CPET is a valuable tool in this regard, providing the clinician with evidence that the patient-perceived symptoms are not due to significant cardiovascular or respiratory disease. It is rare that either healthy subjects or patients with chronic disease score their symptoms (i.e. dyspnoea, leg fatigue) higher than 7 on the Borg 10-point scale, especially at peak exercise 62, although in patients with chronic disease the ratios of symptom score/V′O2 and symptom score/V′E may be increased 23, 63.
Poor effort
The assumption underlying CPET is that test termination signifies the expression of physiological system limitation. In rare cases, however, the end-point may be reflective of poor effort (“Could, but won't”), as, for instance, with malingering 4. Thus, poor effort is evident in a low V′O2,peak with a high fC reserve and breathing reserve. The lactate threshold may not be reached, or may be normal rather than low. Breathing pattern is likely to be atypically irregular (see supplementary material, fig. 2⇓, panel 7), leading to erratic fluctuations in end-tidal and arterial PCO2 (see supplementary material, fig. 2⇓, panel 6).
Differential diagnosis
Exercise testing has been proven to be useful for: distinguishing between normal and abnormal responses to exercise; differentiating between cardiovascular and pulmonary causes of exercise intolerance 1, 64–68; and identifying disorders of pulmonary gas exchange, certain muscle diseases and psychological disorders 4, 23–25.
Algorithms based on key measurements can be helpful in the identification of the causes that limit exercise tolerance. However, they may fail in the evaluation of early or mild disease as well as combined disease (i.e. cardiac–pulmonary). Furthermore, although several differing interpretative algorithms have been developed, none have been clinically validated. Notably, in one study of 130 consecutive, clinically indicated cardiopulmonary exercise tests that were performed with radial and pulmonary artery catheters in place 69, a widely used, noninvasive cardiopulmonary exercise test diagnostic algorithm 4, unmodified, showed a sensitivity for pulmonary vascular limitation (defined as pulmonary vascular resistance at maximum exercise >120 dynes·sec·cm-5) of 79%, a specificity of 75% and an accuracy of 76%. With some adjustments of branch-point threshold values, specificity and accuracy improved to 88% and 85%, respectively.
CPET response profile in specific diseases
This section considers whether specific patterns of response abnormality have diagnostic power for particular pulmonary (COPD, ILD, primary pulmonary hypertension (PPH), cystic fibrosis (CF)) and cardiac (CHF) diseases.
Chronic obstructive pulmonary disease
While the response to incremental exercise may have certain characteristic features, the diagnosis of COPD patients, except in rare exceptions, requires no more than clinical history and spirometry. Exercise testing in such patients, however, is increasingly used for the objective measurement of exercise capacity and for the identification of the causes limiting exercise tolerance that can be eventually be ameliorated or even corrected by specific interventions (e.g. bronchodilators, supplemental oxygen, rehabilitation). In COPD patients, exercise intolerance is multifactorial in origin. Recognised contributory factors include, alone or in combination, exertional symptoms (e.g. dyspnoea, leg fatigue), reduced ventilatory capacity, development of dynamic hyperinflation, peripheral muscle dysfunction and O2 transport abnormalities. These factors are highly interdependent and occur in variable combinations that differ from patient to patient. Importantly, exercise intolerance cannot be predicted in the individual patient from indices of pulmonary and cardiac function at rest 70–73. V′O2,peak obtained with CPET is the best available index of aerobic capacity in COPD, provided that the subject has attained his or her limits (see supplementary material, 1.1), and its measurement is also reasonably reproducible in COPD 74–76.
Ventilatory limitation, ventilatory requirement and dynamic hyperinflation
In the vast majority of COPD patients, CPET reveals that exercise tolerance is largely limited by the combination of a reduced ventilatory capacity and an increased ventilatory requirement, which exacerbates dyspnoeic sensation. In addition, a heightened perception of leg effort may be a limiting factor in a substantial number of patients, particularly during cycle-ergometer exercise 63, 77. Importantly, the development of dynamic hyperinflation has been recognised as an important limiting factor responsible for the development of intolerable dyspnoea during exercise (fig. 1⇓; see supplementary material, 1.7) 78. The increased ventilatory demand in flow-limited patients during exercise gives rise to air trapping and dynamic hyperinflation 32. The extent of dynamic hyperinflation depends on the degree of expiratory flow limitation, the shape of the maximal expiratory flow–volume loop, the prevailing V′E, the breathing pattern at that level of V′E, and the degree of resting lung hyperinflation. The decrease in inspiratory capacity (IC) often occurs in association with an increased Pa,CO2 32, 79 or a reduced VT 80, which strongly suggests that respiratory mechanics are reaching their functional limit. However, the extent of the reduction in IC with exercise in COPD is variable. In a population of 105 patients with moderate-to-severe COPD, IC at end-exercise was reduced by 20% of its already-reduced resting value 81, as exemplified in figure 1⇓. In another smaller group of 27 severe COPD patients, a similar reduction was found at the end of high-intensity exercise 80. Similar changes have also been reported in severe COPD 82.
Other ventilatory abnormalities frequently observed in COPD during exercise are a high V′E for a given V′CO2, due to the variable contribution of an increased VD/VT and a reduced PCO2 set-point because of arterial hypoxaemia and premature metabolic acidosis.
Arterial oxygen desaturation during exercise
The detection of O2 desaturation is an important indication for CEPT in COPD patients since neither the occurrence nor the severity of desaturation during exercise can be predicted readily from resting pulmonary function 73, 83. Only in cases when high DL,CO is accompanied by a high resting Sp,O2 (i.e. ≥95% at sea level) does DL,CO have an elevated negative predictive value 84, but in a large retrospective study, overall sensitivity and specificity, determined by receiver operating curve analysis, were both 75% with a cut-off point of 62% pred for DL,CO 85.
Arterial desaturation during exercise is a common feature of advanced COPD 53, 54. While desaturation may occur with any type of intense leg exercise, walking either on a treadmill or freely along the ground elicits more hypoxaemia than cycle-ergometry 54, 86–88. Any of the standardised walk tests is suitable for diagnosing desaturation 11.
Exercise-induced bronchoconstriction
EIB, defined as a fall in post-exercise FEV1, should be suspected in any patient who presents with wheezing, cough, chest tightness or dyspnoea during or shortly after exercise. In adults, a challenge test is indicated: in making a diagnosis of EIB in asthmatic patients with a history of breathlessness during or after exertion, particularly in those complaining of symptoms after exercise in spite of presumably adequate treatment; and to determine the effectiveness and optimal dosing of medications prescribed to prevent EIB 83, 89, 90.
Comparisons of exercise challenges for EIB with histamine and methacholine challenges in asthmatic patients show that exercise challenges are consistently less sensitive but more specific than chemical challenges in detecting EIB 91–97. Many asthmatics (∼30%) with mild bronchial hyperresponsiveness to chemical stimuli have negative responses to exercise challenges, but there are individuals who have positive responses to exercise challenges and negative responses to histamine or methacholine challenges 98. Taken together, this information suggests that a positive exercise challenge outcome is relatively specific in identifying clinical asthma, but is somewhat insensitive to the presence of clinically relevant mild bronchial hyperresponsiveness. In this regard, the sensitivity–specificity profile of exercise challenge response resembles that of a histamine or methacholine provocative concentration causing a 20% fall in FEV1 of 1 or 2 mg·mL-1 99.
For practical reasons, running on a treadmill is usually preferred for the detection of EIB in children. This enables the use of the muscles most often used in play and other common physical activities, whereas cycling may lead to muscular fatigue at a lower absolute work rate. It has been shown in children that running provokes EIB more easily than cycling, and free running more than running on a treadmill in a laboratory 100. Running for 6–8 min provokes a greater decrease in post-exercise FEV1 than running for shorter or longer periods, recognising that running on a motor-driven treadmill is particularly useful and easy to standardise 101.
EIB is thought to be caused by increased heat and/or water loss due to increased ventilation during exercise 102, 103. Standardisation of these factors is thus important in exercise challenge testing. It is recommended that exercise testing for EIB be performed at room temperature (20–22°C), with a relative humidity of ∼40%. When exercise testing is used to monitor EIB with repeated measurements, these environmental factors should be kept constant.
Choice of work-rate is essential to the outcome of EIB testing 104, 105. Furthermore, the widespread use of inhaled steroids in the treatment of asthma reduces the response to exercise 106, 107. In order to obtain the highest possible sensitivity level, the work-rate should be kept high. The 1999 ATS guidelines recommend that the work-rate should be 80–90% of the calculated maximum 90, and even higher levels, up to 95% of calculated maximum, may be advantageous 105.
In addition to diagnosing EIB, the reduction in FEV1 after standardised exercise may be considered as a measure of nonspecific bronchial hyperresponsiveness 108 and used to evaluate the severity of asthma, as well as the effects of therapy 107. When an extra stimulus is added to the exercise test, by combining running on a treadmill with the inhalation of dry cold air at -20°C, the sensitivity of the test is markedly increased while simultaneously maintaining a high degree of specificity 109.
For other measures of indirect bronchial responsiveness, the sensitivity of exercise testing for EIB is rather low 110, especially in children treated with inhaled steroids 107. This is understandable, as one of the main goals for treating asthma in childhood is the mastering of EIB. In children not treated with inhaled steroids, the sensitivity of the test is higher and comparable to that of methacholine or histamine bronchial provocation 111. However, the specificity of the EIB test for the diagnosis of asthma is high 109, 110. By adding inhalation of cold air during the test, the sensitivity may be increased while maintaining the specificity 109. Exercise load should be kept high to maintain the sensitivity 105.
Interstitial lung disease
ILD represents a broad and heterogeneous group of disorders, which display some common response patterns to exercise. As in other pulmonary conditions, exercise intolerance is multifactorial, but intolerable exertional symptoms, restrictive mechanics and severe gas-exchange derangements are often the primary contributors. Concomitant cardiovascular abnormalities and peripheral muscle dysfunction may also contribute 20. Ventilatory response patterns typical of ILD have been well described: a reduced ventilatory capacity with reduced breathing reserve (albeit not as much as in COPD), an increased V′E–V′CO2 slope, and a characteristically high breathing frequency and low VT at any given level of V′E.
V′O2,peak has been shown to be reproducible in ILD 112, 113 and is therefore a useful means to objectively measure exercise capacity, as is the case in COPD. Again, as for COPD, there are certain exercise response characteristics that are suggestive of ILD, although the diagnosis of ILD is rarely made with exercise testing. Pulmonary gas-exchange abnormalities during exercise may be the only physiological alteration evident in ILD 114, 115.
Abnormalities in respiratory mechanics
Exercise tolerance in patients with ILD is mostly limited by restrictive lung mechanics. Thus, there is a reduced ability to increase VT and thence V′E in response to the metabolic demands of exercise, consequent to a flattening of the lung compliance (volume–pressure) curve 116. Also, the resting IC and inspiratory reserve volume (IRV) are frequently reduced. With exercise, end-expiratory lung volume (EELV) encroaches progressively onto the upper flatter regions of the already-flatter compliance curve, with further exacerbation of elastic load. Thus, VT “saturates” early and there is resultant tachypnoea with exaggerated tidal airflow excursions (see supplementary material, fig. 2⇓, panel 7). A few small studies have indicated that IC remains largely unaltered throughout exercise in ILD, even in patients who exhibit expiratory flow limitation 117. Avoidance of further encroachment of VT on the expiratory reserve volume (ERV) would be expected to attenuate expiratory flow limitation over lower lung volumes. However, failure to decrease EELV during exercise (as occurs in healthy subjects) may have negative consequences with respect to work-sharing between the inspiratory and expiratory muscles.
Expiratory flow limitation has been described in some patients with ILD and may reflect airway obstruction as a result of smoking or airway involvement in the disease process 116, 117. The lack of dynamic hyperinflation during exercise in these patients may reflect the already diminished IC at rest, such that patients may reach a critically reduced IRV and terminate exercise before air-trapping can occur.
Dyspnoeic intensity during exercise in ILD patients has been shown to correlate both with the increasing VT/IC ratio and with the increased inspiratory effort/displacement ratio (a crude index of respiratory neuromechanical dissociation) 118.
Arterial oxygen desaturation
As in COPD, arterial desaturation during exercise in ILD cannot be predicted on the basis of resting lung function. Most patients with moderate or severe pulmonary fibrosis show arterial desaturation during exercise 51, 52, 119. Measuring the work-rate at which desaturation emerges may be of interest for patient counselling on demanding physical activities or for deciding the prescription of ambulatory oxygen therapy.
Cardiac function
Cardiovascular function is abnormal in many patients with ILD. During exercise, patients with ILD usually have elevated fC with reduced stroke volume 120, 121, and an elevated pulmonary artery pressure is common in advanced ILD 122, 123. Finally, clear cardiac involvement is evident in ∼5% of patients with sarcoidosis during exercise 124.
Pulmonary vascular diseases
In patients with chronic PVDs, such as PPH, pulmonary hypertension associated with collagen–vascular diseases, chronic thromboembolic disease and pulmonary vasculitis, exercise tolerance is usually markedly reduced 22, 69, 125–127. This is mostly due to the increased pulmonary vascular resistance that prevents the normal increase in cardiac output during exercise 22. Patients complain of intolerable dyspnoea on exertion, associated with an increased ventilatory response; typically this happens even during light physical activities and in the absence of abnormalities in resting pulmonary function. Resting DL,CO may be reduced, particularly in more severe disease, but not invariably in mild-to-moderate disease 128. The typical pattern of exercise response consists of a reduced V′O2,peak, θL and peak O2 pulse, a normal or slightly reduced breathing reserve, a high V′E/V′CO2(i.e. >34 at θL) with a high VD/VT and an increased PA−a,O2 22, 69, 125. This pattern was shown to be 88% specific in distinguishing patients with pulmonary vascular resistances >120 dynes·sec·cm-5 from those with lower values in a series of 130 patients referred because of unexplained exertion dyspnoea and fatigue 69.
In most cases, CPET can be performed safely in patients with PPH for functional and prognostic evaluation 22, 69, 125, 127. However, exercise testing may not be indicated, or should be approached very cautiously, in patients with recent history of syncope or arrhythmias, and/or when signs of right-heart failure are present 129.
Oxygen transport abnormalities
During exercise, patients with PVD demonstrate significant O2 transport abnormalities: decreased V′O2,peak and V′O2–work-rate slope (see supplementary material, 1.2) and premature θL. Recent research in patients with PPH has confirmed that reductions in V′O2,peak not only reflect a reduced ability to deliver and utilise oxygen at the tissue level 22 but also that it is a reproducible measurement 130.
Ventilatory and gas-exchange abnormalities
Patients with PVD usually display a low V′E and a normal breathing reserve at peak exercise. In the majority of PVD patients, a significant feature is the increased V′E at any given V′CO2, relative to normal 22, 69, 125. This reflects the increased physiological dead space consequent to reduced pulmonary perfusion, and is reflected in the widening of PA−a,O2 during exercise 22, 50, 69, 125. A right-to-left shunt may also contribute to the arterial desaturation during exercise in a proportion of patients with coexistent patent foramen ovale 131. Usually, Pa,CO2is low at rest and does not fall further during exercise. This is thought to reflect hypoxaemic stimulation of carotid chemoreceptors and possibly also vagal reflex activation via stretch receptors in the pulmonary circulation 132.
The excessive V′E at low absolute work-rates may also reflect the influence of a premature lactic acidaemia (i.e. θL is low, presumably because of cardiac impairment and/or coexistent deconditioning). The breathing pattern tends to be more rapid and shallow than normal. This pattern appears not to reflect restrictive lung mechanics, although little is known about respiratory mechanics during exercise in PVD. Animal studies suggest this tachypnoea may result from activation of vagally innervated mechanoreceptors in the right atrium, pulmonary vasculature and pulmonary interstitium 133.
Chronic heart failure
Exercise intolerance in CHF is complex and multifactorial 134 and, as for pulmonary disorders, resting indices of cardiac function (e.g. EF) fail to predict peak exercise capacity 135. Cardiovascular factors are believed to be predominant in this regard and relate to impairment in the cardiac pump with an inability to increase cardiac output appropriately in response to the increased metabolic demands of exercise. However, abnormalities in locomotor muscle circulatory function have also been well described, including abnormal vasoregulatory control 136. Consistent with this view is the demonstration from large population studies that leg discomfort is the most common exercise-limiting symptom in CHF 63.
Cardiovascular abnormalities
CPET has proved very useful in the detection and quantification of cardiovascular abnormalities during exercise in CHF. The characteristic findings are a reduced V′O2,peak and θL, a steeper HR–V′O2 relationship with a reduced fC reserve at peak exercise and a shallower profile (or even flattening) of the O2 pulse increase with increasing V′O2 (see supplementary material, 1.4 and fig. 4⇓) 64, 137. The following can also be observed: an increased V′E–V′CO2 slope over the moderate-intensity domain (i.e. up to θL) 4, 138–140; periodic breathing at rest and during the early phase of exercise; and expiratory airflow limitation at peak exercise. It should be noted that the previously mentioned alterations are not sufficiently specific for CHF, however; they are observed, for instance, in patients with pulmonary vascular disorders 22, 69, 125.
V′O2,peak has been found to be reproducible in CHF patients 141, 142. A normal V′O2,peak virtually excludes CHF 21. Exercise testing plays a minor role in the diagnosis of heart failure, but pulmonary gas-exchange data obtained during exercise provide important information on a patient's functional capacity and distinguish cardiovascular from pulmonary limitations during exercise 1, 2, 64–68.
As an objective measure of the patient's global aerobic capacity, V′O2,peak offers advantages over other indices, such as the traditional New York Heart Association classification of functional impairment in CHF based upon a patient's symptoms rather than on objective criteria, in assessing the severity of CHF 143. Because of the close relationship between V′O2,peak and the maximal cardiac index, grading severity by V′O2,peak provides an excellent measure of disease severity. The exercise capacity of patients with heart failure, based on V′O2,peak and θL, can be divided into four classes 13. However, although widely used, this classification can be criticised because it fails to consider age, sex and weight differences. Despite this, stratification of ambulatory heart failure patients using Weber's classification has improved the ability to identify those with the poorest prognosis, and who should be considered for heart transplantation 144. Guidelines for V′O2,peak as a criterion for cardiac transplantation 144, 145 categorise patients for heart transplant according to V′O2,peak (in mL·kg-1·min-1) as follows. Accepted indication: <10; probable indication: <14; inadequate indication: >15.
Ventilatory abnormalities
In recent years, exaggerated ventilatory responses to exercise have repeatedly been reported in CHF patients 138–140. V′O2,peak is generally reduced, reflecting the reduced symptom-limited peak V′O2, and the breathing reserve at peak exercise is normal or decreased. V′E at any given V′CO2 is typically increased. Contributory factors include: premature metabolic acidaemia (reflecting reduced O2 delivery and/or utilisation) 146, 147; increased physiological dead space 4; increased sympathetic system activation via mechano- or pressor-receptor stimulation in the exercising muscles 148–152 and, possibly, contributions from cardiopulmonary vagal and sympathetic reflexes 132, 153, 154. Several studies have shown that breathing pattern in CHF is more rapid and shallow than in healthy controls at any given V′E 4, 155, 156.
A few studies have measured respiratory mechanics during exercise in CHF 157, 158 Reduced static lung compliance has been described at rest, even in oedema-free patients 159. Increased airways resistance and hyperresponsiveness have also been reported, even in nonsmokers, which may reflect mucosal oedema 160. Recent data from the literature suggest that, despite breathing reserve usually being normal, CHF patients may develop expiratory airflow limitation at peak exercise and that this is the cause of exertional dyspnoea 158. Patients who have resting expiratory flow limitation have been shown to demonstrate significant dynamic hyperinflation in exercise when ventilatory demands are increased 157. The tachypnoeic breathing pattern responses may also reflect inspiratory muscle weakness, although the role of the latter in CHF remains conjectural. Dynamic hyperinflation during exercise in CHF would be expected to be associated with “high-end” mechanics, as in restrictive lung diseases.
Periodic fluctuations in V′O2 and V′CO2 at rest and at low work-rates may be observed in patients with CHF, particularly in the more severe cases 161–163. The cause is unclear but might reflect periodic fluctuations in pulmonary perfusion and/or ventilation.
Congenital heart diseases
As early as 1982, American Heart Association guidelines were published for the use of exercise testing in children with cardiovascular diseases 164. Subsequently, a treadmill protocol for children with congenital cardiac disorders, characterised by slow increases in both speed and inclination, has been developed 165. Fredriksen et al. 166 compared the level of fitness, as reflected by V′O2 peak, in 196 healthy children and 187 children with congenital heart diseases (CHD) and found that children with CHD had lower values that declined after the age of 12–13 yrs. McManus and Leung 167 discussed how exercise testing could be optimised for diagnostic purposes in children with various heart diseases and recommended not only the measurement of V′O2, but also that the assessment of V′O2and V′E kinetics may help to discriminate between pulmonary, cardiovascular and deconditioning causes of exercise limitation. V′O2,peak and the slope of the V′O2–work-rate relationship have been used to evaluate improvements in exercise tolerance after heart surgery 168, 169. The use of exercise testing in assessing the long-term prognosis of children with CHD has not been reported.
UTILITY OF EXERCISE TESTING IN PROGNOSTIC EVALUATION
CPET variables, as well as 6-MWD (table 1⇓) have proven useful in the prognostic evaluation of patients with pulmonary and cardiac diseases (e.g. COPD, ILD, PPH, CF, CHF, candidacy for transplantation and for thoracic surgical procedures), and these are now a main indication for exercise testing in these patient groups. From the available literature, exercise tolerance (V′O2,peak, 6-MWD) and other CPET variables (V′E–V′CO2 slope, θL, Sp,O2) seem to be better predictors of prognosis than resting lung function and cardiac function.
Exercise tolerance is well recognised as a good predictor of mortality in healthy subjects, across ages ranging from young adults to elderly 170–173. This also appears to be the case in a wide range of pulmonary and cardiovascular disease states. CHF currently provides the best instance of the establishment of a comprehensive cluster of CPET-based prognostic variables.
The purpose of this section is to consider prognostic value of CPET-related and other exercise tests in establishing the prognosis of patients with chronic respiratory and cardiac diseases. Data are available concerning the value of exercise indices in COPD, ILD, PVD, CF and CHF. Several other disease conditions for which CPET-based variables may provide good prognostic value fall outside the scope of the present discussion and are not discussed here.
Chronic obstructive pulmonary disease
Traditionally, FEV1 and age have been regarded as the most important predictors of mortality in COPD 174. Other resting indices have been found to predict the prognosis of these patients, the most important being BMI 175, 176, IC/total lung capacity (TLC) ratio 177, arterial hypoxaemia during sleep 178, pulmonary artery pressure 179, mixed venous partial pressure of oxygen (PO2) 180 and the degree of functional breathlessness 181.
In the past few years, COPD has come to be viewed as a systemic disorder in which many extrapulmonary aspects in addition to airflow limitation can influence survival. Skeletal muscle dysfunction is among these 182–184. Therefore, there has been some focus on the prognostic value of correlates of exercise tolerance. The utility of CPET in evaluating disability and impairment in COPD patients has been established. However, the relationship between survival and CPET responses is not yet well established.
V′O2 peak
In COPD patients, Oga et al. 185 reported that V′O2,peak is the most significant predictor of 5-yr mortality. In particular, V′O2,peak <654 mL·min-1 was associated with 60% mortality at 5 yrs and V′O2,peak 793–995 mL·min-1 was associated with 5% mortality at 5 yrs (fig. 2⇓).
Recently, Hiraga et al. 186 conducted a large retrospective study focused on the prognostic value of many CPET variables, including directly measured Pa,O2. They confirmed the prognostic value of V′O2,peak, reporting a 5-yr mortality of 62% for V′O2,peak <10 mL·min-1·kg-1. However, the severity of exercise-induced hypoxaemia evaluated by the slope of the Pa,O2–V′O2 relationship (ΔPa,O2/ΔV′O2 or “Pa,O2 slope”) was the independent prognostic factor most closely associated with the survival time. In particular, a Pa,O2 slope <-80 mmHg·L-1·min-1 was associated with an elevated mortality risk, with <20% survival at 5 yrs.
Timed walking tests
The earliest data regarding the ability of field tests to predict mortality refer to post-rehabilitation outcomes of patients with advanced pulmonary disease. Gerardi et al. 187 concluded that the post-rehabilitation 12-min walking test distance was the strongest predictor of survival up to 3 yrs post-intervention in individuals with predominantly moderate-to-severe COPD, independent of the cause of death. This observation was later confirmed by Bowen et al. 188, using the 6-MWT. A recent study 189 focused on the decline of 6-MWD over 2 yrs in COPD patients; the authors of that study found that the magnitude of change in the group that survived was significantly lower than in nonsurvivors. Very recently, the 6-MWT distance was integrated in a grading system called BODE (Body mass index, airflow Obstruction, Dyspnoea, Exercise capacity), formulated to categorise and predict outcome in patients with COPD. In a cohort of 625 patients, Celli et al. 190 have prospectively validated the BODE index as a good predictor of death from any cause and from respiratory causes after correction for coexisting conditions. The authors reported that the index was a significantly better predictor of mortality than FEV1 alone.
The pre-operative value of exercise tests as an outcome measure in lung-volume reduction surgery (LVRS) has been explored. Szekely et al. 191 reported that a 6-MWD <200 m before or after pulmonary rehabilitation is an excellent pre-operative predictor of unacceptable post-operative mortality at 6 months, with a specificity of 84%. Similarly, a randomised controlled study by Geddes et al. 192, to evaluate the effect of LVRS in patients with emphysema, indicated that a pre-operative shuttle walk test (SWT) distance <150 m was a predictor of high peri-operative mortality. Interestingly, in the National Emphysema Treatment Trial 193, exercise capacity was used to identify the subgroup of patients for whom LVRS has the most favourable survival and cost-effectiveness compared with medical therapy. This important trial reported that patients with a pre-operative peak work-rate <25 W for females and <40 W for males who also had predominantly upper-lobe emphysema manifest significant improvements in survival and functional outcomes at 3 yrs, compared with medical treatment.
Risks of peri-operative complications are often stratified by V′O2,peak. A value below a threshold of 15 mL·min-1·kg-1 indicates a significant risk of complications. Data on field exercise tests are limited, however. For patients with COPD, a 6-MWD of 250 m would correspond approximately to this threshold. Kadikar et al. 194 retrospectively observed the sensitivity and specificity of the 6-MWT to predict death in 145 patients who had undergone lung transplantation; a distance <400 m appeared be an appropriate marker for listing patients for transplant. For LVRS, the threshold for a successful outcome has been reported to be ∼150 m for the SWT 192 or 200 m for the 6-MWT 191.
Interstitial lung diseases
In patients with ILD, CPET may be particularly useful in detecting exercise-related ventilatory and gas-exchange abnormalities (e.g. arterial desaturation and an elevated ventilatory requirement) early in the course of the disease when resting lung-function measurements appear to be normal. Perhaps more importantly, arterial desaturation and other CPET indices have proven useful in predicting the prognosis of patients with ILD.
Arterial oxygen desaturation
A large study conducted by King et al. 195 focused on developing a clinical–radiological–physiological (CPR) scoring system that predicts survival in patients with ILD with biopsy-proven usual interstitial pneumonia (UIP). Pa,O2 at peak exercise was found to be a significant independent predictor of survival, accounting for as much as 10.5% of the maximum CPR score in the completed model. Lama et al. 52 reported that exercise-induced desaturation <88% during the 6-MWT was strongly predictive of mortality in patients with ILD and biopsy-proven UIP.
V′O2,peak and V′E/V′CO2
A retrospective study of 41 patients with a clinical diagnosis of idiopathic pulmonary fibrosis reported that Pa,O2 slope, V′O2,peak, O2 pulse at peak exercise and V′E/V′CO2 at peak exercise are significant predictors of survival 196. Interestingly, among the above indices, Pa,O2 slope was correlated most closely with the survival rate.
The present authors know of no studies regarding the prognostic value of pre-operative exercise indices in relation to survival after lung transplantation in ILD patients.
Primary pulmonary hypertension
PPH is a relatively rare condition associated with high mortality. In recent years, new drugs have been used (e.g. prostacycline, bosentan), aimed at reducing the degree of pulmonary hypertension, although lung transplant remains the only definitive cure. In the past, invasive techniques (i.e. right-heart catheterisation with measurement of pulmonary artery pressure and cardiac output) have been used to assess the severity of PPH, the response to interventions and the timing of transplant. More recently, exercise testing (often considered unacceptably hazardous in the past) has been used to define disease severity and prognosis.
V′O2,peak
Wensel et al. 127 studied the prognostic value of V′O2,peak in patients with PPH. They reported that PPH patients with V′O2,peak ≤10.4 mL·min-1·kg-1 have a 50% risk of early death at 1 yr and 85% at 2 yrs, whereas patients with V′O2,peak >10.4 mL·min-1·kg-1 have a 10% risk of early death at 1 yr and 30% at 2 yrs. In addition, they reported that patients who had both V′O2,peak ≤10.4 mL·min-1·kg-1 and peak systolic blood pressure <120 mmHg had a very poor survival rate at 12 months (23%), whereas patients with one or none of these risk factors had better survival rates (79% and 97%, respectively; fig. 3⇓).
6-MWD and arterial desaturation
In PPH patients, 6-MWT performance correlates well with V′O2,peak. Again, there appears to be some prognostic value for the 6-MWT. Patients walking <332 m had a significantly lower survival rate than those walking further. In particular, in the short-distance group the survival rate at 20 months was 20%, compared with the long-distance group in which there was a 90% survival rate 197. Exercise-induced hypoxaemia as measured by pulse oximetry during the 6-MWT was observed to be significantly predictive of mortality in patients with PPH 198.
Cystic fibrosis
Many variables have been examined and some have proven to have a good predictive value for prognosis in CF patients. Indices of pulmonary function at rest, in particular FEV1 (as % pred or as the magnitude of its deterioration over time) have been shown to be good predictors of mortality. FEV1 along with Pa,O2, Pa,CO2, age and sex are the major indices used to classify the severity of CF and for referral for lung transplantation 199–202.
There are, however, differences in clinical outcome among CF patients with similar resting functional indices. Other factors have therefore been explored, such as malnutrition (e.g. low BMI) and recurrent infections of the respiratory tract with polyresistant pathogens (e.g. Pseudomonas spp., Burkholderia cepacia) 203–206.
Physical activity is regarded as particularly important in children with CF and assessment of physical fitness as an important measure of prognosis. The degree of fitness will (in addition to the level of physical activity) depend upon the progression of the pulmonary part of the disorder 207–209.
V′O2 peak and ventilatory indices
Many studies have confirmed that the value of V′O2,peak is equal or superior to that of resting tests in the stratification and prognostic evaluation of patients with CF. Nixon et al. 203 followed 109 CF patients, age of 7–35 yrs, for 8 yrs after initial exercise testing and calculated survival rates. Patients with the highest levels of aerobic fitness (V′O2,peak ≥82% pred) had a survival rate of 83%, compared to 51% and 28% for patients with middle (V′O2,peak, 59–81%) and lowest (V′O2,peak ≤58% pred) fitness levels, respectively. After adjustment for other risk factors, patients with higher aerobic fitness levels were more than three times as likely to survive as patients with lower fitness levels. Stanghelle et al. 210 showed comparable findings in their 8-yr follow up of 8–16-yr-old CF boys. Moorcroft et al. 211 have found that V′O2,peak, peak work-rate, V′E,peak and V′E/V′CO2 at peak exercise are all significant predictors of mortality. In contrast to previous studies, however, they found FEV1 to be a better predictor than exercise measures.
Arterial desaturation and walking distance
Balfour-Lynn et al. 212 compared a 3-min step test with a 6-MWT and found both useful in the assessment of exercise tolerance in children with CF, whereas Selvadurai et al. 213 and Pouessel et al. 214 validated a shuttle test in CF children and found this a useful test.
In field test studies, the indices most commonly used for patient evaluation are the distance walked, the lowest Sp,O2 and fC 215. Some authors have found that V′O2,peak in patients with CF was correlated with 6-MWD, with the correlation coefficient increasing if age, weight, FVC, FEV1 and DL,CO were added to the prediction equation 216, 217. However, other authors have found no correlation between distance covered in a 12-MWT and survival 202. Other authors reported that an elevated breathing reserve at θL (defined as V′E at θL divided by the MVV) is associated with an increased risk of death in CF patients awaiting lung transplantation 218. The utility of this breathing reserve index rests on the fact that it combines a resting measure of lung function with a measure of exercise capacity that does not depend on patients attaining the point of symptom limitation.
Chronic heart failure
Exercise testing in cardiac patients has been used extensively to confirm the clinical suspicion of coronary ischaemia and, perhaps more importantly, to establish prognoses 219, 220. Guidelines for the indications and interpretation of exercise testing in patients with coronary artery disease are available 68.
More recently, CPET has been increasingly used to assess the degree and mechanism of exercise intolerance in patients with heart disease. V′O2,peak, θL, V′E/V′CO2 and other physiological variables have been used as measures of functional status in patients with CHF. Perhaps more importantly, several studies have been published on the usefulness of CPET measurements in the prognostic evaluation of CHF patients. What is not entirely clear, however, is how β-adrenergic blockade therapy, through effects on indices such as V′O2,peak and V′E–V′CO2 slope, may alter prognostic prediction in CHF. However, Peterson et al. 221 and O'Neill et al. 222 have recently reported the prognostic value of peak V′O2 to be unaffected with β-blockade in CHF, although the latter authors have suggested that the 14 mL·kg-1·min-1 cut-off for cardiac transplantation may require re-evaluation in this setting.
V′O2,peak
V′O2,peak has consistently demonstrated prognostic significance in CHF 223, 224, with lower V′O2,peak predicting higher mortality and the need for heart transplant. Mancini et al. 225 reported that V′O2,peak >14 mL·min-1·kg-1 is associated with 94% survival at 1 yr and 84% survival at 2 yrs; while patients with V′O2,peak ≤14 mL·min-1·kg-1, who were rejected for transplant for noncardiac reasons, had survival rates at 1 and 2 yrs of 47% and 32%, respectively. Kleber et al. 226 reported a better prognosis at 30 months for patients with V′O2,peak >45% pred. Szlachcic et al. 227 reported that V′O2,peak <10 mL·min-1·kg-1 is associated with 77% mortality at 1 yr, while in patients with V′O2,peak >10 mL·min-1·kg-1 mortality rate at 1 yr is ∼20%. More recently, Gitt et al. 138 reported that CHF patients with V′O2,peak ≤14 mL·min-1·kg-1 (or ≤50% pred) had a three-fold increased risk of death at 6 months 138. Arena et al. 228 confirmed that V′O2,peak <14 mL·min-1·kg-1 conveyed a poor prognosis (sensitivity 84%; specificity 48%). In some of the previously-mentioned studies 138, 227, 228, it was observed that the combination of CPET variables, particularly V′O2,peak and V′E–V′CO2 slope, better identifies patients at high risk of early death from CHF than V′O2,peak alone (see below).
There is now a general consensus that patients with V′O2,peak <14 mL·min-1·kg-1 should be considered for heart transplantation, as originally stated in the report of the 24th Bethesda Conference 145.
Lactate threshold
Because of the poor cardiovascular adaptation, the development of lactic acidaemia in patients with CHF occurs prematurely early in the course of an incremental exercise test. Some authors prefer to use θL values, rather than V′O2,peak, to assess patients’ functional status instead of V′O2,peak because (in contrast to θL) the latter is highly effort-dependent. However, only one study has examined the prognostic value of θL in CHF patients: Gitt et al. 138 demonstrated that θL <11 mL·min-1·kg-1 is associated with a mortality risk ratio at 6 months of 2.7 (similar to the risk ratio of 2.9 for V′O2,peak ≤14 mL·min-1·kg-1).
V′E/V′CO2at θL and V′E–V′CO2 slope
Evidence has been provided about the utility of V′E/V′CO2 measurements in patients with CHF. Unless there is a concomitant lung disease that worsens the alveolar ventilation/perfusion ratio, an increase in V′E/V′CO2 usually reflects an impairment in lung gas diffusion and/or the development of pulmonary hypertension during exercise. As emphasised earlier, Pa,CO2 should be measured to rule out the possibility that an increased V′E/V′CO2 and /or V′E–V′CO2 slope reflects hyperventilation.
There has been recent interest in using the V′E–V′CO2 slope, in addition to V′O2,peak, to assess the prognosis of patients with CHF 138–140, 227, 229–232. As described in the supplementary material (section 1.5), normal values for the V′E–V′CO2 slope are in the region of 23–25 (i.e. below the respiratory condensation point). A V′E–V′CO2 slope >130% pred is associated with a 1-yr mortality rate >40% 226. In a study of 470 patients, an abnormal elevation in the peak V′E/V′CO2 ≥44.7 was the strongest predictor of death during a 1.5-yr follow-up 232. A V′E–V′CO2 slope >34 has been shown to be a better predictive index for early death (6 months) from CHF than V′O2,peak 138. An elevated ventilatory response to exercise can reflect decreased ventilatory efficiency (increased VD/VT), and is predictive of outcome in patients with preserved exercise capacity. In another study of 123 patients with a V′O2,peak ≥18 mL·min-1·kg-1, the 3-yr survival was significantly lower in those with a peak V′E/V′CO2 ≥34 (57% versus 93% for V′E/V′CO2 ≤34) 140. A V′E–V′CO2 slope >34 is a significantly better predictor of both 1-yr cardiac-related mortality and 1-yr cardiac-related hospitalisation than V′O2,peak 228.
Walking tests
The utility of the 6-MWT has been examined in mild-to-moderate 233 and more severe 234 CHF patients. Both studies associated a distance <300 m with a reduced medium- to-long-term overall survival and reduced event-free survival. In more severe CHF patients, baseline 6-MWT distance was a strong independent predictor of mortality and hospitalisation at 1 yr 235. The feasibility of the SWT for selection for heart transplantation has been documented; a distance of >450 m equates to a V′O2,peak for treadmill walking >14 mL·min-1·kg-1 236.
Combinations of variables
Gitt et al. 138 examined the prognostic value of CPET variables, alone or in combination in a large cohort of CHF patients. They reported that θL <11 mL·min-1·kg-1 and V′E–V′CO2 slope >34 combined better identified patients at high risk for early death than V′O2,peak (≤14 mL·min-1·kg-1 or ≤50% pred) alone or in combination with θL (<11 mL·min-1·kg-1) or with V′E–V′CO2 slope (>34).
In studies that used multivariate Cox regression analysis, V′E–V′CO2 slope appears to be the most powerful predictor of event-free survival, followed by V′O2,peak (table 2⇓) 138, 226, 228.
UTILITY OF EXERCISE TESTING IN DEFINING RESPONSES TO INTERVENTIONS
CPET variables as well as distance covered during walking tests have proven to be useful in clinical trials evaluating interventions in patients with pulmonary and cardiac diseases (e.g. COPD, ILD, CF, PPH, CHF). This is now the main indication for exercise testing in these patient groups. CPET variables, as well as distance covered during walking tests, have proven to be useful in individual prescription of pulmonary rehabilitation and O2 supplementation (by exercise testing pre- and post-intervention), and also for prescription of exercise training. These are now main indications for exercise testing in these patient groups. Indeed, the use of an initial CPET-based assessment prior to entering an exercise training programme is to be strongly recommended.
Exercise tolerance has become an important outcome measure in patients with COPD, CHF and other chronic diseases, mostly because evidence has been provided that exercise testing is superior to other functional measurements obtained at rest (e.g. FEV1, left ventricular EF) in demonstrating the positive effect of a specific intervention. In particular, exercise testing has been widely used in cardiorespiratory disease to explore the short- and long-term benefits of exercise-based rehabilitation, nutritional or hormonal therapy, drug therapy, O2 or heliox breathing, and surgical interventions such as LVRS and transplantation.
What is the “best” measure of improvement in exercise tolerance?
Laboratory-based tests allow evaluation of therapeutic effects mostly by detecting improvement of exercise capacity as well as characterising ventilatory, gas-exchange, circulatory and metabolic response patterns, but are limited by the setting and by expensive equipment. Walking tests can be used easily in a field setting and are inexpensive, but they provide less information regarding the specific physiological responses underlying altered exercise capacity.
Different exercise protocols and different exercise measures have been used to quantify the improvement of exercise tolerance in patients with cardiorespiratory diseases, although the laboratory symptom-limited incremental test, with measurement of V′O2,peak or peak work-rate, and walking tests, with measurement of maximal distance walked, have been most popular. More recently, indices reflecting the patient's endurance capacity have succesfully been used. The most common and popular of these is the time to symptom limitation on a constant-load cycle-ergometer test, although a few studies have actually defined the power–duration relationship and estimated critical power (CP; see supplementary material, 2.2 and fig. 8).
Comparisons between incremental and endurance cycle-ergometry tests indicate that the incremental exercise test is excellent at describing the profile of system abnormality but less suitable than endurance cycle-ergometry for discriminating the outcome of interventions in terms of improved exercise capacity. A necessary prerequisite for employing constant-load exercise testing as an outcome measure in pulmonary rehabilitation, and also in drugs studies, is individualising the work-rate to be performed in the pre-rehabilitation study. Power–duration principles 237–241 dictate that the work-rate to be used must be above CP (see supplementary material, 2.2 and fig. 8). It should be noted, however, that after training this work-rate may be below the pre-training CP (i.e. the patient may be able to perform the constant-load task for a relatively long period of time; see supplementary material, fig. 9). In COPD, there is increasing evidence that high-intensity constant-load endurance protocols with measurement of tlim, symptoms (e.g. dyspnoea and leg fatigue) and pertinent CPET variables (e.g. V′O2, V′E–V′CO2 slope respiratory frequency, IC, fC) at “isotime” are superior to other protocols (e.g. V′O2,peak on maximal intemental test, distance on 6-MWT) in the evaluation of the effects of therapeutic interventions 242.
In choosing an appropriate exercise test and a specific outcome marker, it is important to know the relationship between the specific exercise response and the local or systemic impairment intended to be modulated by the specific intervention. For example, Man et al. 88 showed in COPD patients that leg effort assessed by subjective scoring on a Borg scale is a frequent symptom during incremental and endurance cycle-ergometry, but infrequent during incremental and endurance walking. This would imply that interventions targeted specifically at the skeletal muscles should preferably be evaluated by cycle-ergometry and not by walking tests. Indeed, a recent study 243 in COPD patients on systemic corticosteroid treatment showed that, relative to exercise training alone, supplementation with anabolic steroids was reflected in enhanced improvement in peak exercise capacity during incremental cycle-ergometry, but not in improved 6-MWD. A complicating factor in a multicomponent disease like most chronic cardiorespiratory diseases, such as COPD or CHF, may be that in individual patients different factors dominate impaired exercise capacity.
Effective rehabilitative interventions will not only be reflected in improved effort-dependent measures of exercise tolerance (e.g. V′O2,peak, peak work-rate, tlim) but will also yield altered physiological responses to identical exercise tasks. These alterations can be detected in both incremental and constant-load cardiopulmonary exercise testing. Commonly used measures predictive of improved responses include dynamic hyperinflation, arterial lactate concentration, V′E, V′E/V′CO2, breathing pattern and Sp,O2.
Clearly, task-specificity also needs to be considered. For instance, interventions specifically aimed at improving upper extremity muscle endurance may be reflected in improved endurance time during arm-ergometry but not during cycle-ergometry.
For use in clinical trials or in individualised patient care, it is also important to know the minimal clinically important change in the different exercise tests. Using the 6-MWT, Redelmeier et al. 244 proposed that a meaningful difference in performance was 54 m for patients with COPD. The minimum clinically important difference has not yet been published for the incremental or endurance shuttle walk test, or for cycle-ergometry.
Besides considering the information that can be retrieved from an exercise test, other factors need to be considered, such as standardisation of procedures to minimise variation, to avoid learning effects and to limit confounding influences related to motivation. This may be particularly relevant when the tests need to be used in multicentre clinical trials.
Symptoms
The severity of exertional dyspnoea, but also leg fatigue, is usually assessed by using a Borg scale or by a visual scale (VAS) 245, 246. The Borg scale has been used extensively to detect changes in dyspnoea after therapeutic interventions, particularly in COPD patients 247–254.
Symptom-limited incremental test
Until recently, most of the studies looked at changes in V′O2,peak, peak work-rate and θL (and also V′E,max and maximum fC) with symptom-limited incremental CPET as primary outcome variables. It should be recalled that as peak work-rate is dependent on the work-rate increment rate (see supplementary material, 1.1 and fig. 1⇓), interpretation of intervention-induced changes should take this into account. In most studies, the improvement in V′O2,peak and/or peak work-rate is usually modest (∼5%) and not unequivocally confirmed (e.g. the improvement in V′O2,peak after rehabilitation in COPD), particularly in patients with the most advanced disease. In some controlled studies, V′O2,peak increased significantly 255–258, while other studies failed to observe a significant amelioration 259, 260. θL has also been used as an outcome variable, particularly in CHF patients. As described earlier, the potential advantage of measuring θL during CPET is that maximal effort is not required; the results of the studies that have used θL are again not unequivocal. In COPD patients, controlled studies did not observe changes in maximal fC or in maximal V′E 258, 259, 261.
Endurance time and physiological measurement at standardised time
Endurance time during high-intensity exercise (i.e. above CP; see supplementary material, 2.2) is increasingly used to assess exercise tolerance before and after a therapeutic intervention. Work-rates used in recent clinical studies were 75–80% of V′O2,peak or peak work-rate measured during symptom-limited incremental CPET. In addition to tLIM, comparisons of symptom intensity (e.g. dyspnoea, leg effort) or physiological variables of interest (e.g. IC, V′E, V′O2, V′E/V′CO2, fC) at a standardised time (isotime) have proved very useful in identifying the underlying physiological mechanisms responsible for increases in exercise tolerance induced by a particular intervention. Recent data from the literature support the notion that in COPD patients, endurance tests are more sensitive than other exercise protocols in detecting exercise-related physiological changes induced by interventions, and are thus very useful in clinical practice (fig. 4⇓) 242.
In recent years, high-intensity constant-load protocols (e.g. 75–80% peak work-rate) have been used to demonstrate the positive effects of interventions such as bronchodilator therapy 252, 253, 262; oxygen 263 and heliox 254 administration during exercise; bronchoscopic lung volume reduction 264; and rehabilitation 265, 266. By using this approach, it is possible to demonstrate a significant improvement in endurance time, mostly due to a reduction in lung dynamic hyperinflation and dyspnoea at isotime (table 3⇓). The “high-intensity” exercise endurance protocol should therefore now be considered the test of choice in evaluating the effects of therapeutic interventions in COPD.
Moderate constant-load exercise
Moderate constant-load tests (i.e. below θL), on a cycle-ergometer or on a treadmill, lasting 6–8 min have been used to detect reductions in symptom scores and also in assessing the V′E and fC responses to training (see supplementary material, 2.1). These tests have been shown to be reliable and reproducible 267. After exercise training, significant reductions in ventilation 255, 256, 259, 261, 268 and lactate levels 255, 261, 268 at identical submaximal work-rates have been observed. These findings suggest an improvement in aerobic metabolism 255, 269 and are in agreement with the observation of a significant increase in oxidative enzyme levels (16–40%) in the quadriceps femoris muscle after a strenuous exercise programme 261. Positive cardiac adaptation at submaximal exercise, identified by a lower fC, has been demonstrated in controlled 255–257, 270 and uncontrolled 261, 271 studies.
The extent of speeding of the response kinetics of V′E and V′O2 (see supplementary material, 2.1 and fig. 7) has also been used to detect improvements in oxygen transport and/or skeletal muscle metabolism after a specific intervention 255, 271, 272. The V′O2 kinetics reflect the overall efficiency of the oxygen transport system including muscle oxidative capacity and, in COPD, seem to be influenced by the oxygen delivery to the working muscles 273.
Walking tests
This approach has been used extensively both in patients with respiratory and in those with cardiac disease. The 6-MWT has been widely used in many large trials exploring the benefits of rehabilitation, pharmaceutical intervention, oxygen supplementation and surgery in cardiorespiratory disease. The 6-MWT has been shown to be a submaximal high-intensity constant-load test 274, 275. The test is used to investigate the effects of interventions on patients’ walking endurance capacity. Measurements of Sp,O2 and fC may be included to detect physiological improvements associated with improvements in exercise tolerance.
Redelmeier et al. 244 proposed that a meaningful difference in performance for patients with COPD was 54 m. This indicates the level at which the patient would appreciate an improvement in function capacity. Troosters et al. 276 reported a mean increase of 52 m in a study of the short- and longer-term benefits of pulmonary rehabilitation delivered over a 6-month period. Results from similar rehabilitation studies confirm the magnitude of change 277, 278. Pharmaceutical interventions have employed the 6-MWT as an outcome measure with some success 279. The test has also been used as an outcome measure in rehabilitation for CHF 280 where a modest change in walking distance after 3 months of exercise training was observed.
The incremental SWT (ISWT) has not been extensively incorporated into pharmacological studies, but has been cited in a number of significant rehabilitation studies 281, 282. There is considerable evidence that the test is sensitive to change. However, the minimum clinically important difference has not yet been published. A large rehabilitation study reported mean changes of 75.9 m 281. In a large group of patients with COPD, the SWT was sensitive to the administration of formoterol and ipratopium bromide 283, 284. The endurance SWT (ESWT) seems more sensitive to change after a course of rehabilitation than the ISWT. Revill et al. 285 secured a mean increase in duration of 160%, compared with the ISWT change of 32%.
The administration of ambulatory oxygen has been described in many international guidelines. This is largely based upon the response to a standard field exercise test. The response is suggested to be either a 10% increase in distance or 10% reduction in dyspnoea with supplemental oxygen. The mode of exercise testing may be important. It appears that walking induces a greater degree of arterial desaturation than cycling 54, 86, 88, 286. The 6-MWT has previously been shown to be sensitive to the administration of supplemental oxygen 287, 288. The ISWT is responsive to the acute administration of oxygen 289. However, the ESWT appears to demonstrate a greater magnitude of change to supplemental oxygen 290.
EVIDENCE-BASED INDICATIONS TO EXERCISE TESTING IN CLINICAL PRACTICE
The Task Force members felt that it was important to indicate the level of recommendation for the most relevant indications for exercise testing in clinical practice, on the basis of the arguments discussed and references provided. For this purpose an appropriate grading system, commonly used for recommendations in evidence-based guidelines, was utilised 291. The grade of recommendation (A = highest, D = lowest), based on the levels of evidence is reported in table 4⇓ for CPET and in table 5⇓ for walking tests. It should be noted that with the use of this rigorous system, grade A is relatively rare and grade B is usually considered the best achievable.
Clear evidence now exists for the utility of CPET, as well as for other exercise test protocols, such as timed walking tests and constant-load tests, in evaluating the degree of exercise intolerance, the prognosis and the effects of therapeutic interventions in adult patients with chronic lung disease (COPD, ILD, PPH), in children and adults with CF, in children and adults with EIB, in adults with CHF, and children and adolescents with CHDs. No consistent data are available in the literature on the clinical impact of CPET in diseases other than those mentioned above.
In clinical practice, CPET has not proven useful in diagnosing specific conditions. However, characteristic profiles of cardiopulmonary and gas-exchange response, discerned using CPET, may help in the differential diagnosis between pulmonary and cardiac limitation to exercise.
CPET should be considered the gold standard for evaluating maximal/symptom-limited exercise tolerance in patients with pulmonary and cardiac disease. Importantly, cardiopulmonary and gas-exchange response profiles measured at CPET are reproducible in the short term and in the longer term they can reflect disease progression. Field testing, often in combination with limited physiological measurements, is also a useful approach to assessing exercise intolerance in patients who may not need comprehensive CPET-based testing. CPET variables, as well as distance covered during 6-MWT, have proven to be useful in the prognostic evaluation of patients with pulmonary and cardiac diseases, and these are now a main indication for exercise testing in these patient groups.
From the available literature, exercise tolerance and other CPET variables appear to be better predictors of prognosis than resting lung and/or cardiac function. However, studies have not yet been carried out to look at combinations of variables.
CPET variables, as well as distance covered during walking tests, have proven to be useful in clinical trials evaluating interventions in patients with pulmonary and cardiac diseases. This is now the main indication for exercise testing in these patient groups. It should be noted that, even if a clinical trial were originally designed to evaluate the effect of an intervention and the trial included exercise tolerance as one of the main outcomes, this can still provide indirect evidence of the interventional utility of exercise testing.
CPET variables as well as distance covered during walking tests have proven to be useful in the individual prescription of pulmonary rehabilitation and oxygen supplementation (by exercise testing pre- and post-intervention), and also for safety for subsequent exercise training (e.g. “healthy” elderly subjects). These should now be considered main indications for exercise testing in these patient groups.
V′O2,peak, 6-MWD and tLIM during high-intensity constant-load endurance protocols have been proven to be superior to changes in resting lung and cardiac indices in the evaluation of the effects of interventions. High-intensity constant-load endurance protocols with measurement of tlim, symptoms and pertinent CPET variables at a standardised time (isotime) should be considered the test paradigm of choice, since they are able to detect significant improvement in exercise tolerance, which is often not the case for symptom-limited incremental exercise testing.
In conclusion, the evidence base on the value of exercise testing in functional evaluation, prognosis and discrimination of interventional changes in pulmonary and cardiac diseases has grown substantially in the past decade. However, as is evident from the summary tables (4 and 5), in some instances, the low power grades are reflective not so much of well-powered statistical judgements as they are of weakness in the density of the relevant evidence base. Such areas should be seen as important priorities for future investigation.
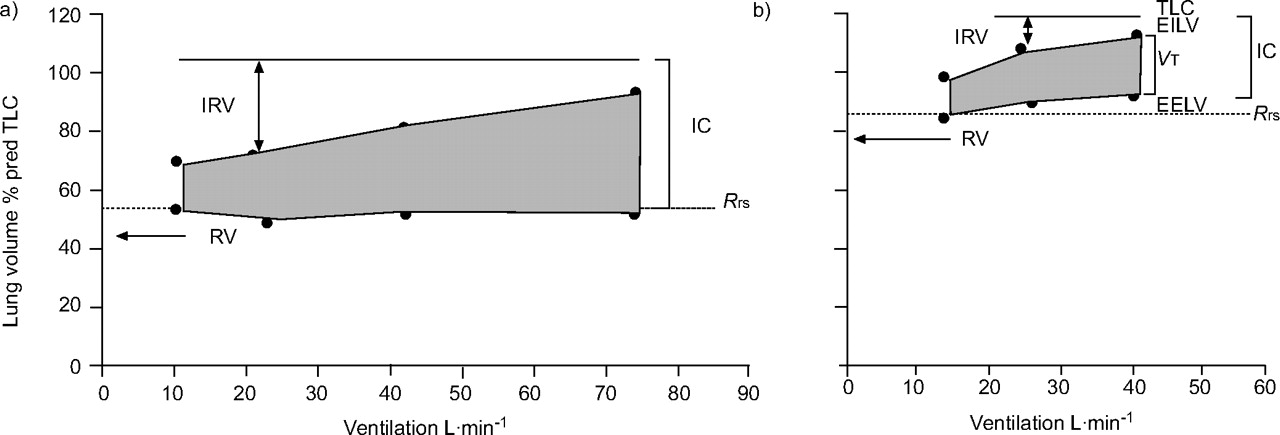
Changes in operating lung volumes are shown as ventilation increases with exercise in a) age-matched healthy subjects and b) chronic obstructive pulmonary disease (COPD) patients. End-expiratory lung volume (EELV) increases above the relaxation volume of the respiratory system (Rrs) in COPD, as reflected by a decrease in inspiratory capacity (IC), while EELV in health either remains unchanged or decreases. TLC: total lung capacity; RV: residual volume; IRV: inspiratory reserve volume; EILV: end-inspiratory lung volume; VT: tidal volume. Reproduced from 78 with permission from the publisher.

Kaplan–Meier survival curves using quartiles of peak oxygen uptake (V′O2,peak). ––––: V’O2,peak >995 mL·min-1 (n = 37); ········: V’O2,peak 793–995 mL·min-1 (n = 38); ------: V’O2,peak 654–792 mL·min-1 (n = 38); – – –: V’O2,peak: <654 mL·min-1 (n = 37). Reproduced from 185 with permission from the publisher.

Kaplan–Meier cumulative survival curves for 3-yr survival of 70 patients with primary pulmonary hypertension. Patients with a peak oxygen uptake (V′O2,peak) >10.4 mL·kg-1·min-1 (––––) versus ≤10.4 mL·kg-1·min-1 (········). Reproduced from 127 with permission from the publisher.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Changes in various measures of exercise performance after oxitropium bromide in three exercise tests. Changes are expressed as the percentage change versus placebo. Values are expressed as mean±se. □: 6-min walking distance (6-MWD); ░: progressive cycle-ergometry; ▒: cycle endurance test. WR,max: maximal work-rate; V’O2,max: maximal oxygen uptake; V’CO2,max: maximal carbon dioxide output; V’E,max: maximal minute ventilation. *: p<0.05; **: p<0.01; ***: p<0.001 versus placebo. Reproduced from 242 with permission from the publisher.
Exercise indices that have been shown to predict the prognosis of patients with chronic respiratory and cardiac diseases
Cox regression analysis, including sex, age, left ventricular ejection fraction, and New York Heart Association class, for calculation of risk of death at 6 months
Effects of different therapeutic interventions on endurance time, lung hyperinflation and dyspnoea in chronic obstructive pulmonary disease
Indications for cardiopulmonary exercise testing in clinical practice
Indications for 6-min and shuttle walking tests in clinical practice
Acknowledgments
The members of the Task Force on Clinical Exercise Testing are grateful to R. Antonucci for her skilful assistance in the preparation of the manuscript.
The members of the Task Force are: P. Palange (Rome, Italy), S.A. Ward (Leeds, UK; chairmen), K.H. Carlsen (Oslo, Norway), R. Casaburi (Torrance, CA, USA), C.G. Gallagher (Dublin, Ireland), R. Gosselink (Leuven, Belgium), O'Donnell DE (Kingston, ON, Canada), L. Puente-Maestu (Madrid, Spain), A.M. Schols (Maastricht, The Netherlands), S. Singh (Leicester, UK) and B.J. Whipp (Leeds, UK).
Footnotes
-
THIS ARTICLE HAS SUPPLEMENTARY MATERIAL ACCESSIBLE FROM ERJ.ERSJOURNALS.COM.
- Received April 4, 2006.
- Accepted August 16, 2006.
- © ERS Journals Ltd
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
-
-
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵











Jump To
- Article
- Abstract
- UTILITY OF CPET IN DIAGNOSIS AND FUNCTIONAL EVALUATION
- CPET response profile in specific diseases
- UTILITY OF EXERCISE TESTING IN PROGNOSTIC EVALUATION
- UTILITY OF EXERCISE TESTING IN DEFINING RESPONSES TO INTERVENTIONS
- EVIDENCE-BASED INDICATIONS TO EXERCISE TESTING IN CLINICAL PRACTICE
- Acknowledgments
- Footnotes
- References
- Figures & Data
- Info & Metrics