





Abstract
Collection of exhaled breath condensate (EBC) is a noninvasive method for obtaining samples from the lungs. EBC contains large number of mediators including adenosine, ammonia, hydrogen peroxide, isoprostanes, leukotrienes, nitrogen oxides, peptides and cytokines. Concentrations of these mediators are influenced by lung diseases and modulated by therapeutic interventions. Similarly EBC pH also changes in respiratory diseases.
The aim of the American Thoracic Society/European Respiratory Society Task Force on EBC was to identify the important methodological issues surrounding EBC collection and assay, to provide recommendations for the measurements and to highlight areas where further research is required.
Based on the currently available evidence and the consensus of the expert panel for EBC collection, the following general recommendations were put together for oral sample collection: collect during tidal breathing using a noseclip and a saliva trap; define cooling temperature and collection time (10 min is generally sufficient to obtain 1–2 mL of sample and well tolerated by patients); use inert material for condenser; do not use resistor and do not use filter between the subject and the condenser. These are only general recommendations and certain circumstances may dictate variation from them.
Important areas for future research involve: ascertaining mechanisms and site of exhaled breath condensate particle formation; determination of dilution markers; improving reproducibility; employment of EBC in longitudinal studies; and determining the utility of exhaled breath condensate measures for the management of individual patients. These studies are required before recommending this technique for use in clinical practice.
- Airway inflammation
- biomarkers
- exhaled breath condensate
- lung diseases
- noninvasive monitoring
- oxidative stress
EXECUTIVE SUMMARY
Recently there has been increasing interest in the investigation of the lungs by noninvasive means including sputum induction and measurement of biomarkers in exhaled breath including nitric oxide (NO) and those found in the cooled and condensed exhalate, termed exhaled breath condensate (EBC). Compounds identified in EBC include adenosine, ammonia, hydrogen peroxide, isoprostanes, leukotrienes, nitrogen oxides (NOx), peptides, cytokines, protons and various ions. Analysis of EBC has potential to address unmet medical needs by expanding the portfolio of noninvasive assays for the multiple coexisting pathological mechanisms underlying respiratory disorders. However this approach to studying the airway chemical and inflammatory environment is still in its infancy, with questions as yet remaining unanswered.
The main objective of the American Thoracic Society (ATS)/European Respiratory Society (ERS) Task Force on EBC was to develop guidelines for EBC collection and measurement of exhaled biomarkers, to make recommendations on the possible use and limits of exhaled biomarkers and to highlight those areas where further research is required. An additional objective was to provide a comprehensive review of previous studies of exhaled biomarkers in EBC, to recommend how to optimise the method and to achieve better standardisation of procedures. Based on the currently available evidence and the consensus of an expert panel, the following general recommendations for oral EBC collection are submitted: collections should occur during tidal breathing using a noseclip and a saliva trap, with a defined cooling temperature and collection time; surfaces contacting the EBC should be inert to the compounds of interest in a given study; inclusion of expiratory flow resistance or filters is not required. As biomarkers in EBC have diverse stabilities and characteristics, these are only general recommendations.
Collection of EBC is a completely noninvasive method of sampling the respiratory tract that can be repeated several times with short intervals between sampling. Collection devices can be portable and can be used in a wide range of settings including intensive care units (mechanically ventilated patients), outpatient clinics, workplaces and at home. These attributes of EBC make it a useful tool for epidemiological investigation, and to help gain understanding of the time courses of important pathological processes (oxidative stress, inflammation) in carefully designed studies of respiratory disease.
Determination of the role of EBC in diagnosis and management of individual patients, an issue distinct from large studies of disease mechanisms, awaits further investigation. EBC is a dilute, complex solution of diverse biomarkers with various chemical stabilities. Conditions and duration of storage may decrease or increase assayed concentrations of biomarkers. For many biomarkers, assays are commonly employed at or near their detection limits, leading to higher variability. Immunoassays (for cytokines, 8-isoprostane, leukotrienes and others) require individual validation in the dilute, low protein, chemically diverse EBC, which is a very different matrix than that employed in many commercially available standards. Sample concentration (lyophilisation and resuspension) and the development of more sensitive techniques are assisting in improving reproducibility. Flow-dependency and the potential for oral/upper airway/salivary contamination is likely different for each biomarker, which therefore, require individual investigation. As yet no fully validated method for calculating dilution of respiratory droplets is available and the anatomic origin of biomarkers is not precisely known. Most of these uncertainties regarding EBC assays are shared by other investigative and even clinical techniques (such as sputum induction, bronchoalveolar lavage, and exhaled NO). Details are provided regarding many of the commonly studied biomarkers, including the advantages, limitations, and potential pitfalls of the detection methods. The effect of different disease states on these EBC biomarker levels is individually summarised.
At the conclusion of the meetings of this Task Force, none of the biomarkers in EBC had been validated sufficiently for clinical use. It is the very diversity of EBC itself that has prevented it from achieving clinical applicability yet. With only a relatively small number of investigators studying each biomarker, the process of advancing standardised methodologies for each individual biomarker will be much slower than that for exhaled NO, for which hundreds of investigators focused on one molecule. The Task Force fully recognises this issue. However, after such validations are indeed accomplished, EBC measurements may improve clinical practice by providing useful information on those critical aspects of disease that are left completely inaccessible by current means.
The number of original publications and reviews on EBC analysis has increased sharply in recent years, as has the interest at international conferences. Clinicians are awaiting the sufficient maturation of EBC techniques to help them with their work. The Task Force, therefore, consider it important to summarise current understanding of the technique and also the limitations of knowledge in the hope that this will generate more coordinated research to find the proper place of this sampling method both in research and clinical practice.
The document is organised as follows: a general section discussing issues common to all EBC biomarkers, followed by individual sections addressing specific biomarkers. Wherever possible, the recommendations and presented opinions are based on peer-reviewed published manuscripts (only scientific publications written in English were reviewed for this document) and not on abstracts; in the absence of clear data, we have relied on the experience of Task Force participants. When aspects of EBC collection and biomarker measurements are undetermined, this has been stated in the text. In each section unresolved issues are highlighted.
INTRODUCTION
Recently there has been increasing interest in the investigation of the lungs by noninvasive means including sputum induction 1 and measurement of exhaled NO 2, 3. Exhaled breath contains dozens of compounds, which can be measured from the cooled and condensed exhalate. After several issues regarding the problems and unsolved questions about EBC formation and collection were highlighted during an ERS Research Seminar 4, a joint Task Force of the ERS and the ATS was created.
The main objective of this Task Force was to develop guidelines for breath condensate collection and measurement of exhaled biomarkers, to make recommendations on the possible use and limits of exhaled biomarkers and to highlight those areas where further research is required. We also aimed to provide a comprehensive review of previous studies of exhaled biomarkers in EBC, to recommend how to optimise the method and to achieve better standardisation of procedures between different laboratories.
The work of this Task Force over 3 yrs was based on the exchange of knowledge between experts, and the recommendations of this document were formulated by international investigators in the field of measurements in EBC at four consecutive workshops held in Berlin in 2001, Atlanta in 2002, Stockholm in 2002 and Seattle in 2003. The initial draft was prepared by I. Horváth based on the notes taken during the workshops and submitted materials by participants and circulated among all Task Force members for review. The report was then presented to the ERS Executive Committee and ATS Board of Directors.
The document is divided into a general section followed by sections addressing individual biomarkers and assay methodology. Wherever possible, the recommendations are based on peer-reviewed published material. In the absence of clear data, the experience of Task Force participants was relied upon. When aspects of EBC collection and mediator measurements are undetermined, this has been stated in the text. In each section unresolved issues are highlighted. Although the number of publications has doubled in each year since 1999, the total number of English-written publications dealing with breath condensate collection is still under 300, and only a few of them address methodological issues. This fact limited evidence-based recommendations. Therefore, everybody interested in the field is encouraged to bring forward data linked to methodological questions to help to better understand this sampling method and to evaluate the usefulness of any data obtained.
While the use of recommendations given (table 1⇓ and section entitled Summary of current recommendations, requirements for EBC collection) will allow direct comparison of data obtained in different centres in future studies, this document does not intend to invalidate studies that have employed other techniques. Importantly, the Task Force does not want standardisation to inhibit innovation. There is substantial room for innovation in collection methods and assays.
GENERAL ASPECTS OF EXHALED BREATH CONDENSATE COLLECTION
Standardisation of terminology
Based on the consensus of the Task Force participants the expression “EBC” is the preferred term to describe the method. This term should be given as a keyword in manuscripts reporting data obtained by using this technique. Of note, in previous publications several other descriptions could be found including: condensate, airway droplets, solutes, etc. As molecules from the airways may be captured by other techniques, not only by cooling exhaled breath, EBC strictly relates to exhaled samples collected by cooling the exhaled breath.
Recommendation
The terminology “EBC” should replace other descriptive terms used for this technique.
Area for further research
None.
Content of EBC
EBC contains several components. The principal component is condensed water vapour 5. This fluid represents nearly all of the volume (>99%) of fluid collected in EBC 6. Only a small fraction of the condensate is derived from respiratory droplets containing nonvolatile molecules (which can be both hydrophobic and water-soluble molecules) 7. Water-soluble volatile compounds are absorbed by the condensing water during collection. During EBC collection exhaled breath is directed through a cooling device, resulting in a liquid or solid phase accumulation of exhaled breath constituents depending on the condenser temperature. During tidal breathing, the liberated aerosol particles range between 0.1–4 particles·cm−3 with a mean diameter of 0.3 μm 8–10, although these data do not identify the smallest particles, of which there may be substantial numbers. The mechanisms which cause airway/alveolar fluid substances or those from the mucus layer to be added to exhaled breath are not clear and further study is required.
Recommendation
None.
Areas for further research
Studies are required on how and from which site of the respiratory system different substances are transported/liberated into the exhaled air and on factors and disease states that influence this process.
Source of EBC
EBC samples collected through the mouth versus through tracheostomies/endotracheal tubes
Levels of some mediators have been compared between EBC samples obtained directly from the lower airways through a tracheotomy tube and those collected through the mouth. Concentrations of adenosine, and thromboxane B2 (TxBx2) and values of pH were not significantly different between these samples 11, 12. Furthermore, although no direct comparison was made, studies using EBC collection through tracheostomy and those collecting EBC through the mouth showed similar levels of hydrogen peroxide (H2O2) and 8-isoprostane 5, 13–17. These results suggest that most of these mediators are added to EBC samples in the lower airways. In contrast the concentration of ammonia is substantially lower in EBC samples obtained through tracheostomies than in those collected through the mouth suggesting that most of this compound is added to the sample from the upper airways or oropharynx 6, 11. The potential effect of inflammatory diseases of the mouth (i.e. periodontitis, gingivitis, etc.) on EBC constituents has not yet been studied. The investigators who most intensively study EBC pH note that if the laryngopharyngeal airway is sufficiently acidic, EBC pH will be affected. Gastric acid reflux could then contribute to EBC pH decline in a subgroup of patients.
Recommendation
Oral/upper airway production of identified EBC constituents should be considered and appropriate control measurements are recommended to be performed to evaluate the influence of the mouth and/or upper airways.
Areas for further research
Studies with direct EBC sampling from the lower airways are needed to determine more precisely the oral/upper airway influence on other mediators. Furthermore, studies on the effect of oral diseases on the content of EBC are required.
Nasal inhalation versus oral inhalation during EBC collection, use of noseclip
In most published studies, subjects inhaled and exhaled through the mouth during collection. In some studies, subjects were asked to inhale through the nose and to exhale exclusively through the mouth. There are some important differences between the two methods which may influence mediator levels found in EBC: 1) during nasal inhalation inhaled air is humidified in the upper airways; 2) mediators formed in the nose and the sinuses more likely enter the lower airways during nasal inhalation. In a study comparing the two methods (nasal inhalation-oral exhalation versus oral inhalation-oral exhalation) more EBC was collected with nasal inhalation in parallel with a larger volume of exhaled air, but no differences were found in the concentrations of adenosine, TxB2 and ammonia in healthy subjects 11. However, in patients with inflamed upper airways higher concentrations of adenosine were found in EBC samples collected with nasal inhalation-oral exhalation than those collected with oral inhalation-oral exhalation, suggesting that adenosine produced in the inflamed upper airways is added to EBC samples 11. These data emphasise that more attention should be given to the potential influence of the upper airways on sampled mediators, especially in patients with ongoing upper airway disease (either nasal or sinus), which should always be noted.
EBC collection with oral inhalation-oral exhalation may be performed with or without the use of a noseclip. Noseclip use prevents any accidental inhalation-exhalation through the nose during sample collection, while this cannot be safely ruled out when collecting samples without it. When tidal breathing is used for sample collection without resistance, the soft palate is not closed and air and mediators present in the nose and sinuses can be added to the sample. The use of noseclip may well minimise the aerosolisation of particles from the nasopharynx. On the other hand, volatile gases formed in the nasopharynx (such as NO) may be entrained to a greater extent in the exhaled air when noseclips are employed (as is indeed the case for NO) 2. At the moment no data are available comparing EBC collected with and without noseclips.
Recommendation
The consensus of the expert panel was that noseclip use is advisable to ensure that no sample is lost through the nose and that inspiration bypasses the nose. The most important recommendation is that investigators should consider the potential effect of nasal airflow on EBC levels of the compound in which they are interested, and perform appropriate control experiments when feasible. In manuscripts, precise description of sampling method (route of inhalation and exhalation, use of noseclip) is required and any ongoing upper airway disease should be mentioned.
Areas for further research
Comparison of data reproducibility between EBC samples obtained with and without noseclips (oral inhalation and exhalation) is needed for mediators detectable in EBC before making explicit recommendation on this issue.
Use of resistor
For single breath exhaled NO measurement, a resistance is used to close the soft palate and to prevent NO produced in the nose and the sinuses from influencing the results 2. Closing the velum consistently during several minutes of tidal breathing for EBC collection is a very different issue. Theoretically, it would be possible to place a resistor between the subject and the condenser during EBC collection, however, its value would be limited by the following: 1) the more effort dependent sampling technique (forced expiration instead of tidal breathing) would exclude a large number of patients who could produce EBC with the tidal breathing method, and 2) expiratory flow restriction would not be expected to prevent nasal contribution to the airstream during inspiration, during which the velum would not be kept closed regardless of expiratory resistance. It is worthy of note that all condensers have some resistance, which is negligible with the commercially available ones but should be checked in the custom-made devices. One group used a resistor when collecting EBC and found better reproducibility in EBC nitrite concentration when using it than without it 18.
Recommendation
At the moment it is not recommended to include resistance in the condensing device for EBC collection.
Areas for further research
Further studies to determine the utility of expiratory flow resistance on the concentrations of EBC mediators will be important. Design of condensers with adjustable flow restriction will be helpful in this endeavour.
Flow-dependency of EBC mediator levels
Few attempts have been made to determine the site of generation of different mediators in the EBC. In this respect, H2O2 level was shown to be flow-dependent, suggesting that it is at least partly derived from the conducting airways 19. In the range of expiratory flows during tidal breathing no flow-dependence was found in adenosine concentration 20. EBC pH was not affected by profound changes in flow rates 12. Similarly the concentrations of malondialdehyde (MDA) was not flow dependent in the flow range between 50 and 200 mL·s−1 measured by an ultrasonic flow sensor 21.
Recommendation
When it has not been sufficiently elucidated in the published literature, the flow dependence of mediator levels should be ascertained and incorporated into publications. This will assist in: 1) determination of the site of mediator liberation; and 2) establishing that, in the flow range found during EBC sampling, variability of mediator concentration is not caused by variation in expiratory flow.
Areas for further research
Further research is required to determine the flow-dependency and the anatomical origin of different mediators derived from the airways and/or alveoli.
FACTORS WHICH AFFECT COLLECTING EBC
Condensing equipments
Commercial versus custom-made devices
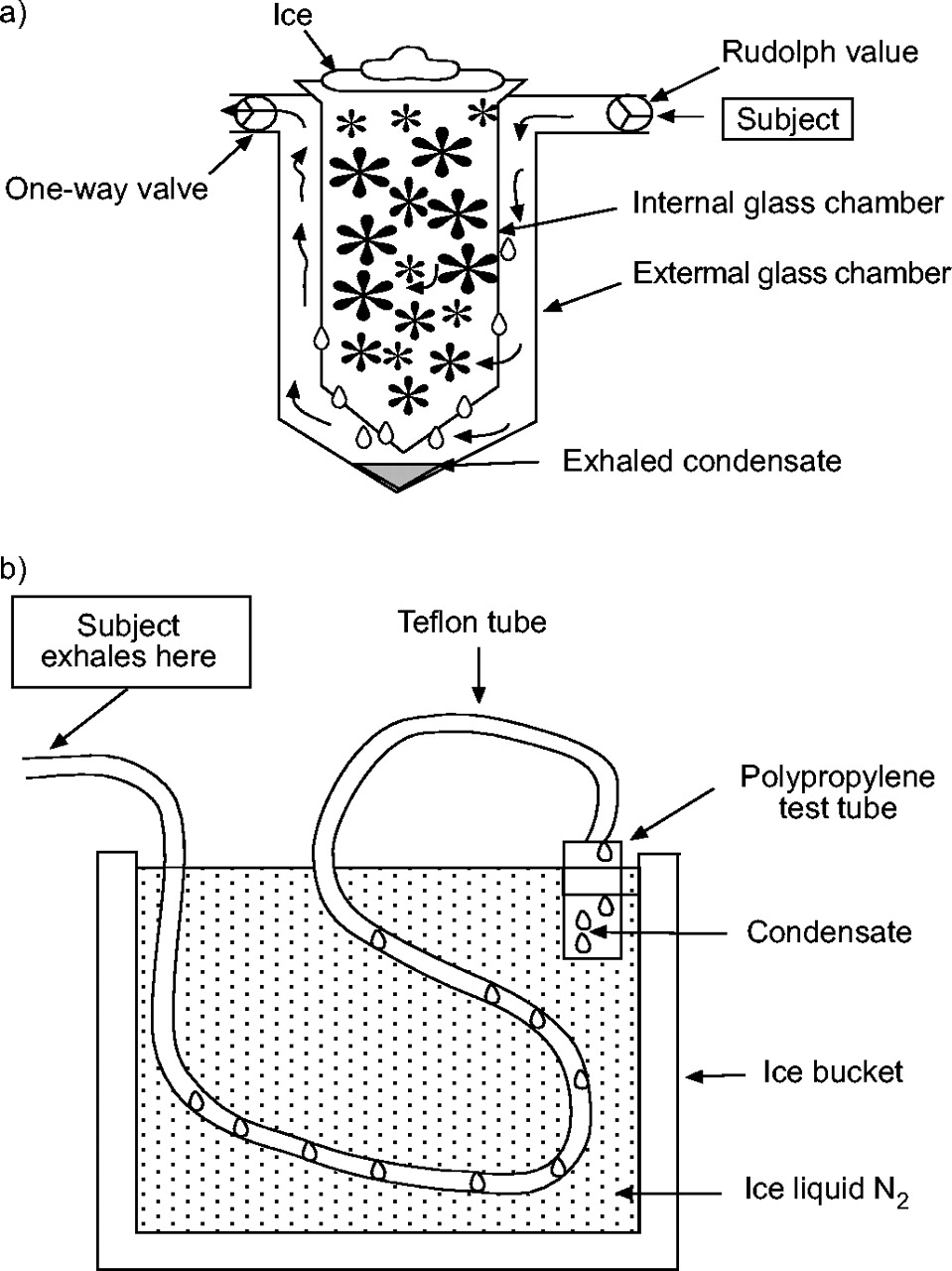
Several different devices have been designed for EBC collection including tubing of different materials (Teflon, polypropylene tubing) of differing length and diameter 5, 14, 19, or double-wall glass chambers 22 (fig. 1⇓).These collecting vessels are cooled with wet ice 5, air 24 metal 25 or dry ice to the required temperature. Comparing a custom-made device (Tygon tubing immersed in thawing ice) with a commercially available condenser (Teflon coated laminated metal tube cooled to −20°C) one study showed that the use of the two devices are interchangeable when measuring MDA, hexanal, heptanal or nonanal 21. Use of commercially available devices may help to overcome potential problems arising from the use of different devices, but no data are yet available showing that the use of these devices results in better reproducibility of data.

{kind=link}
{kind=link}
Commercial systems and most published custom EBC collection systems employ one-way inspiratory valves to assure that the patients do not inhale cold air that has passed through the condenser during inspiration. This is an obvious important consideration to avoid unintentional cold air challenge.
Recommendation
Describe exactly what type of condensing device is used. If a home-made device is built, give details on the design (saliva trap, its resistance, material of the condensing surface, cooling method, temperature of condenser, its stability over the collecting period). When conducting a study, use the same device, or if different devices are to be used give results on the comparison of the equipments used. Current consensus is that equipment should have an inert material on the condensing surface, although different biomarkers may have different reactivities with surface materials. The collection equipment should be connected to the subject in a way that prevents gross salivary contamination, with one-way valves to prevent inhalation through the condenser and also to avoid condensation of ambient air before and/or during EBC.
Areas for further research
Comparison of efficacy and reproducibility of sampling (condensate volume, mediator level) between different devices should be a focus of further studies. Further studies are also required to establish if different mediators are evenly distributed in the expired air and if collection of all water vapour expired would decrease variability of EBC data.
Efficiency, duration and temperature of condensation
Generally, with 10 min of tidal breathing 1–3 mL of EBC can be collected from resting adult subjects (∼100 μL·min−1 EBC with range of 40–300 μL·min−1). None of the available condensers collect all exhaled water vapour, since estimated water loss is around 30–35 mg·L−1 in a wide range of ambient air temperature and humidity 26, 27. One study estimated the water extraction by a cold trap integrated into the cooled head sampling unit and found that ∼40% of water vapour was extracted with no difference in the efficiency of water vapour extraction in healthy subjects versus chronic obstructive pulmonary disease (COPD) patients 28. Similar EBC volume was found by others using a 200 cm tubing connected to the expiratory port of a ventilator kept under saline-ice water 14.
Collection time used in most published studies is between 10–30 min with only a few studies using very short (3 min) or rather prolonged (60 min) collection time 7, 12. In most studies 10 min has been used and this time period can be recommended for two practical reasons: 1) this collection time results in 1–2 mL of condensate from adult subjects and most children >4 yrs of age; and 2) subjects usually tolerate this period of sampling without fatigue (although loss of interest may still occur in children). At the same time, however, different study set-ups may require other collection times (i.e. shorter when time course of changes is assessed or longer when a larger amount of sample is needed). Direct comparison of different collection times has only been published regarding pH level, showing no effect of changes in collection time between 3–20 min on EBC pH in healthy subjects 12. Although no direct comparison is available regarding other mediators, no difference can be found in the concentrations of H2O2, nitrite/nitrate, 8-isoprostane, adenosine and MDA between studies using 10, 15 or 20 min for EBC sampling.
Gessner et al. 28 showed not only that EBC volume was linearly related to the volume expired, but also to the total protein and urea content found in EBC suggesting that these compounds accumulated in the collecting device by a similar mechanism as expired water vapour. This even distribution, however, is not necessarily true for all substances present in EBC and needs further study. For standardisation of EBC sampling some investigators have suggested collection for a time over which a pre-defined volume of air (100 L in adults) is expired, instead of setting fixed collection time. This approach is based on the observation that EBC volume is directly proportional to the volume of exhaled air, therefore, keeping the same volume of exhalate would minimise the otherwise large inter-individual variability of EBC volume. No published data are available, however, on studies comparing these two approaches with respect to reproducibility of mediator concentrations.
Condensation can be achieved at temperature around 0°C using wet (salty) ice, when EBC can be collected as fluid, and it can also be collected at lower temperatures using different techniques (dry ice, liquid nitrogen, placing cooling sleeve to required temperature, cooling air to preset temperature, etc.), which results in the collection of frozen material. Regarding temperature of condensation, it should be noted that the collecting surface warms up from the exhaled air and this influences the collecting temperature. The solubility of volatile mediators in the collected samples may be influenced by temperature, and data reveal that concentration of ammonia is lower if the condensate is collected as ice rather than water. Condensing temperature and time is also important for those mediators that are unstable, such as leukotrienes and purines.
Recommendation
Investigators should report collection temperature and duration of condensation (and if time or expired volume was kept constant). Keeping the same sampling temperature and time in studies that require repeated sampling is advisable. Regarding the collection time, 10 min is recommended for most mediators, as it provides an adequate sample for assay of most mediators of interest and is well tolerated by patients.
Areas for further research
Further studies need to address the effect of collecting time and temperature on different mediator levels and to compare the reproducibility of EBC mediator measurements between sampling with set collection time versus expiratory volume. Studies on particle distribution and development of more efficient devices are also needed.
Ambient air
Ambient air contains molecules which may influence EBC composition through several possible mechanisms. Atmospheric compounds can: 1) directly contribute to EBC levels; 2) react and, therefore, change or consume molecules trapped in EBC; and 3) lead to inflammatory and biochemical changes in the airway that are subsequently reflected by changes in EBC composition. It has been demonstrated that atmospheric NO reduces exhaled H2O2 levels 29. Ambient air that has not interacted with the respiratory system (not been inhaled) can be excluded by a device design with unidirectional flow through the condenser with the intention of minimising direct contact with ambient air. EBC samples can also interact with ambient air if samples are left exposed to room air after collection. This may result in important changes in mediator concentrations if an unstable mediator or a volatile compound is of interest or when the measured molecule or a reactive precursor molecule is present in ambient air. Finally, velocity, temperature and humidity of inhaled air may all influence the volume and content of EBC, but data are lacking on this issue.
Recommendation
Control experiments in which subjects inhale air that does not contain the compounds (or their precursors) that will be measured in EBC should be considered by each investigator. Furthermore, unless proven unequivocally to be acceptable for a given mediator, EBC samples should not be left out at room temperature after collection (the latter is important not only because of the interaction with ambient air, but also because substances may be degraded or formed in EBC more readily at this temperature).
Areas for further research
Studies with inhalation of known gas mixtures are needed to establish the effect of changes in ambient air on EBC characteristics.
Breathing pattern
Exhalation flow has an important influence on exhaled NO and it is, therefore, necessary to consider this possibility in relation to any volatile components of EBC. Exhalation flow influences the level of exhaled H2O2; at higher flows exhaled H2O2 concentration is lower, but with the low flows during tidal breathing the effect is minor 19. A strong correlation was found between total respired volume and breath condensate volume by different authors 11, 28. An animal study showed clear positive correlations not only between minute volume and EBC volume, but also to variables determining the breathing pattern (i.e. tidal volume per kg body weight and respiratory frequency) 30.
However, the effect of changes in minute ventilation on EBC volume and mediator concentration intra-individually in humans has not been fully published. It is known from previous studies that no consistent differences were detected in expired water content values as ventilation increased 26, 31.
No studies have been reported on the effect of breath-holding on mediator levels in EBC. No published data on the possible effect of cough (either spontaneous or induced) on EBC volume and content are available at the current time. Since this event likely influences both variables, and may even facilitate the release of “droplets”, controlled studies are required.
EBC collection appears to have no influence on lung function or exhaled NO levels 32.
Recommendation
Use tidal breathing for EBC sampling and report on the flow-dependency of the measured mediator where known.
Areas for further research
Further studies are needed to assess the effect of changing minute ventilation and coughing on the volume and content of EBC.
Airway calibre and lung function
EBC volume does not depend on lung function parameters including forced expiratory volume in one second and forced vital capacity (FVC) either in normal subjects or in patients with COPD 28. At present there is no evidence to show that changes in airway calibre cause any difference in mediator release or dilution of EBC, but this question has not been studied systematically. There are data that reveal no change in EBC pH after acute airway obstruction induced by methacholine 12.
Recommendation
None.
Areas for further research
Further studies are required to assess the effect of changes in airway calibre on different mediators in EBC.
Age and sex
The largest database of variables affecting the concentration of an EBC biomarker is available for H2O2. This mediator is not age-dependent in children, but higher levels were found in older than younger adults 13, 33, 34. Body weight or height do not affect EBC volume and H2O2 concentration in adults 28; however no data are available regarding other mediators. No published data are available on the potential effect of race, sex and body position on the volume of orbiomarker concentrations in EBC.
EBC can be collected from children as young as 3–4 yrs using the same technique as used in adults 32, 33. It may be possible to use a face-mask 35 and EBC has been successfully collected from newborn babies in this way 36. Collections by continuous aspiration through a nasal cannula can also be considered 37, 38. When sampling EBC orally from children the main difficulty is their loss of interest, so sample collection time should be minimised.
Recommendation
Consider the potential effect of race, age and sex.
Areas for further research
Further studies are required to establish reference data for different mediators in EBC.
Food and drink
To the best current knowledge of the Task Force food and drink do not influence the determined nonvolatile mediators. This question, however, has not been studied systematically for all compounds of interest. When measuring mediators known to be affected by certain drinks or foods it is advisable to refrain from these for a few hours before measurement (for example to refrain from caffeinated drinks before measuring adenosine).
Recommendation
As study protocols are developed, evaluate the potential effect of eating, drinking, taking medication on the EBC concentration of the biomarkers of interest.
Areas for further research
Further studies are required to assess the effect of food and drink on different mediators in EBC.
Circadian rhythm
A circadian rhythm has been demonstrated for EBC H2O2 level both in normal subjects and patients with COPD 13, 34. No circadian rhythm was identified for pH in a study of 152 subjects 12. No prospective studies are available to show or rule out any diurnal variation of EBC volume or other mediators present in EBC.
Recommendation
In longitudinal studies consider the potential of circadian rhythm in mediator level and plan sampling to the same time of the day if diurnal variation is shown.
Areas for further research
Further studies are required to assess circadian rhythm of different mediators in EBC.
Tobacco smoking
Information is available on cigarette smoking, but not on cigar or pipe smoking. The effects on EBC biomarkers of different cigarette brands, including presence or absence of a filter and origin, have not been elucidated. Smoking (both chronic and acute smoke exposure) has considerable effect on H2O2, isoprostane, nitrite and nitrotyrosine levels measured in EBC 35, 39–42. In healthy subjects cigarette smoking causes an increase in EBC H2O2, 8-isoprostane and nitrotyrosine concentration and in neutrophil chemotactic activity with no change in concentrations of interleukin (IL)-1β or tumour necrosis factor-α 35, 39–42. In asthmatic patients acute smoke exposure also caused an elevation in EBC H2O2 level 43. In patients with COPD no difference was observed in the mean EBC H2O2 and 8-isoprostane level between smokers and nonsmokers 44–46.
Recommendation
Smoking habit should be documented and in smokers it is advisable to refrain from smoking for at least 3 h before measurements to prevent the acute influence of smoke on mediator levels. An acute smoking group can also be considered as a control. In long-term studies changes in smoking habit should be noted (if possible avoided).
Areas for further research
Studies on the effect of smoking on other mediators/characteristics of EBC are needed.
Systemic diseases
It is important to consider the potential effect of systemic diseases including extrapulmonary systemic diseases on mediator levels in EBC. In this respect approximately 20-fold higher H2O2 level was described in EBC from uraemic patients compared to healthy subjects 47.
Recommendation
Consider systemic diseases as potential confounding factor when EBC variables are used as biomarkers of respiratory diseases.
Area for further research
Studies are required to determine the effect of systemic diseases on EBC variables. The potential use of EBC as a biomarker of extrapulmonary diseases should also be studied.
Medication
Several studies showed differences in EBC mediator levels in relation to medication (see details in paragraphs discussing mediator measurements). Although most studies on mediators in EBC are cross-sectional, significant differences have been demonstrated between treated and untreated groups in different airway diseases.
Recommendation
All used medication should be carefully listed and their effect on mediator level should be considered.
Areas for further research
Determination of the utility of EBC for evaluating effects of therapeutic compounds will benefit from longitudinal studies assessing the effect of medications on mediator levels.
Ventilated patients
Condensers can be connected to the outgoing limb of most respirators and samples can be collected 5, 6, 11, 12, 14, 36, 48, but the humidification system may contribute solutes or substantially dilute the EBC, and these factors will likely change depending on the total flow through the circuit. This approach provides an opportunity to sample the lower airways directly and to investigate patients with respiratory failure.
Recommendation
None.
Areas for further research
None highlighted.
Safety
Collection of EBC is a safe method of gaining information regarding respiratory fluids; no adverse events have been reported in over 10,000 measurements performed in different laboratories with different devices. EBC collection does not have any influence on lung function or mediator levels, and can be repeated several times with short intervals (minutes) between measurements. Since the pattern of breathing is normal, it is safer than FVC measurements, which may provoke bronchospasm in some asthmatic patients. It is noted that some people tend to hyperventilate especially at the beginning of EBC collection, but this has not led to any adverse event. Care must be taken that the risk of infection between individuals is avoided. Although no bacterial DNA fragments were detectable in EBC samples from tidally breathing cystic fibrosis (CF) patients 49, the possibility of other components of the collecting system transmitting microbes to subsequent users seems real. This risk of infection can be minimised by using disposable mouthpieces and tubing between the mouth and condenser and a one-way valve to avoid inhaling from the condenser. The use of disposable condensers is an alternative approach. In most pulmonary function equipment, an exhalation particle filter is employed to eliminate contamination of the machine. The use of such a filter for EBC collection presents potential problems, however, the effect of an expiratory particle filter proximal to the condenser on the concentration of a compound in EBC will depend on the characteristics of the compound. Substances that are primarily derived as volatiles (by nature, uncharged) may be affected differently by a filter than charged nonvolatile macromolecules, which may be trapped more by the filter. The use of such filters inserted before the condenser is, in general, not recommended, unless appropriate studies are performed to evaluate the effects of filtering the exhaled breath on the levels of the specific mediator studied. Disinfection of reusable condensers must be carried out with special caution, since some residual disinfection agents (i.e. those work with formaldehyde) may destroy mediators collected in the disinfected collection tubes, and residual contamination from the cleaning process may affect subsequent samples
Recommendation
Do not use filters between the subject and the condenser. Take special care to disinfect reusable collecting devices, and assure that residual cleaning agents do not adversely effect the assays for, or levels of, the biomarkers of interest.
Areas for further research
Further studies are needed to assess if infective agents including viruses can be demonstrated in EBC.
Reproducibility, dilution factor, concentration of samples
With tidal breathing methods the volume of EBC is a reproducible characteristic of EBC, which is not surprising since exhaled air is nearly saturated with water at body temperature 5, 11. Mediator levels in EBC are more variable than EBC volume even if reference techniques such as HPLC are used for determination, but with sensitive assays good reproducibility has been found for adenosine, aldehydes, glutathione and pH in EBC 11, 12, 20, 50. The cause of variability is not completely understood, but two components are likely to be involved: changing dilution (for nonvolatiles) and large same sample variability of some of the assay techniques used. The latter in most cases is due to the fact that most biomarkers in EBC are at the low end of assay sensitivity, making variability more likely.
Dilution factor
Some attempts have been made to assess the dilution of alveolar lining fluid (ALF) in EBC samples and to standardise EBC by using exhaled volume 5, exhaled ions 6, 51, 52, urea 6, 53, protein concentration 28 or conductance of lyophilised samples 51 as “internal standards”, or by using external dilution markers. The importance of a dilution factor is based on the assumption that the ratio of liberated solutes to exhaled water vapour is unpredictable and can change, but a so called “dilution factor” can be determined from each EBC sample by determining the concentration of a substance in EBC, which has a well known concentration in sera and diffuses through the cell membranes, but is not produced in the alveoli or airways. Such a dilution marker would make it possible to calculate the “real airway level” of determined mediators in EBC. It has been suggested that concentrations of electrolytes or urea or the measurement of conductance can be used for estimating dilution of EBC 6, 51. The simplest of these is the measurement of conductivity of lyophilised samples 51. One study found only a small inter-day intra-subject variability in the concentration of sodium and chloride concentrations in EBC samples from healthy subjects and patients with CF, suggesting that variable dilution is not likely a major cause of variable biomarker levels 52. In contrast, when measuring urea as a dilution factor for nonvolatile compounds in EBC, considerable within-subject variability was found with a dilution factor ranging between 8,300 and 48,400 53.
EBC collection offers an advantage over collecting bronchoalveolar lavage (BAL) because it is completely noninvasive, no medication is required to employ the technique and no external fluid is added to the airways 54. ALF is diluted to a great extent in EBC 6 and EBC compounds are likely to represent not only ALF, but also the mucus layer of the airways 53. It has not yet been convincingly demonstrated that better reproducibility can be achieved by normalising EBC data with a dilution factor. Although dilution may be a factor influencing EBC data, it is unlikely that changes in mediator levels observed in different airway diseases can be completely explained by changes in droplet release or formation. Furthermore, it is important to note that this approach cannot be used for volatile compounds in EBC, for which other aspects need to be considered 53.
Detection limit of the assay techniques, sample concentration
Most of the mediators found in EBC are in the lower range of detection of the assay techniques currently available, where the intra- and inter-assay variability of methods is large (see Measurements of mediators in EBC). Exceptions, in which levels are fully in the range of available assays, include total protein, nitrate, pH and ammonia. Reporting inter-assay and intra-assay variation given by the manufacturer may be misleading when values are around the lower detection limit and, therefore, they should be determined for the concentration range found in EBC samples to enable any power calculation for studies using the measurement of given mediator in EBC. In this respect more sensitive methods for detection and very careful handling of samples are required. Another source of concern is that standard curves for immunoassays should be generated using standards that are similar to the EBC matrix, or at least that the assay be validated to assure that nonspecific results/false positives are avoided.
A potential option to overcome this problem is the concentration of samples. Lyophilisation and vacuum-evaporation has been used by some investigators. These approaches were used in some studies (i.e. 3-, 4-fold concentration for measurement of nitrotyrosine and leukotriene B4 (LTB4); see below, or lyophilisation for conductivity measurement; 51), however these methodologies were not systematically evaluated (i.e. data on mediator recovery have not been published). Volatile , semi-volatile, and unstable substances (i.e. ammonia, H2O2, leukotrienes) will or may be lost during freeze-drying.
Recommendation
Give details of intra-assay and inter-assay reproducibility measurements carried out using EBC samples by using appropriate means of evaluation (i.e. Bland-Altman test when appropriate, or coefficient of variation) 55. Specify the lower limit of detection and the definition used for it (this may vary even between commercial kits). If there are values under the detection limit consider them as such and use appropriate test for statistical analysis. Whenever possible, use methods which give data well above the detection limit. In case of sample concentration give adequate data on recovery. Rigorously determine specificity of the assay.
Areas for further research
Adequate studies on reproducibility measurement and reference data are required. Development of more sensitive and specific assays for most mediators found in EBC and data on results of sample concentration are also needed.
Salivary contamination
Studies on the protein content of EBC collected through the mouth show that EBC contains molecules not present in saliva 56 and the electrolyte ratios of saliva differ from those in the orally collected condensate 6. This information suggests that saliva is not the dominant contributor to EBC.
However, saliva contains many of the mediators that are also present in the lower airways, and indeed it is reasonable to consider that there is some exchange of compounds between the saliva and the lower airways. This is particularly relevant for the compounds found at higher concentrations, including volatile substances. Since we are interested in lower airway sampling, salivary contamination should be rigorously excluded when collecting exhaled breath. Various techniques can be used to avoid gross salivary contamination, such as the use of a saliva trap, placing the condenser at a higher level than the mouth making it more unlikely that saliva can enter the collecting device and separating the mouth-piece from the condenser by a length of tubing. Detecting salivary amylase is a frequently used method to exclude saliva contamination in EBC. Several studies have demonstrated that if care is taken to exclude saliva from EBC samples amylase can be detected only in a small portion of samples with levels approximately 10,000 times lower that those in saliva 6, 20. However, amylase measurements are not specific for salivary amylase and amylase can also be found in the lungs, so positive results of the test do not necessarily mean salivary contamination. Furthermore, the dilution of airway lining fluid is great in EBC, and care must be taken in interpreting amylase data. A negative signal does not completely exclude minute contribution from the mouth. Furthermore, the majority of proteins recovered from EBC collected from isolated lower airway were also found in saliva, suggesting that these proteins are present in both compartments (i.e. saliva and secretions of the lower airways) 56. Both the anatomical and biochemical sources are still an issue with exhaled NO 57, and these issues should be considered no less important for EBC. It is, therefore, reasonable to assume that there is some degree of oral contamination of EBC because of particles being formed there as well. To complicate matters, lower airway-derived compounds can be trapped in the mouth. To allow the assessment of potential sample “contamination” by the mouth, it will be useful to seek changes in salivary concentration of the compounds that are being assayed in EBC. Whenever possible, studies should also be conducted in patients with endotracheal tubes or tracheotomies.
Recommendation
According to current experience there is no need to determine and report salivary amylase level in EBC samples, but efforts should be made to prevent salivary contamination.
Area for future research
More sensitive assays to exclude oropharyngeal contamination are of interest.
Summary of current recommendations, requirements for EBC collection
Based on the consensus of the expert panel and on the published data detailed above, the following recommendation should be observed for EBC collection (table 1⇓): oral sample collection should be performed with subjects in sitting position wearing a noseclip while tidal breathing. Collection time and temperature can vary depending on the study objective, but it should be kept the same within any one study and precisely reported. It is required to have a condensing device with inert material on the collecting surface, containing a sufficient salivary trap, having a mouth piece with separated inlet (as an inhalation port) and outlet (to direct exhaled breath toward the condensing apparatus), with low resistance without a filter between the subject and the condensing chamber.
When reporting data on EBC detailed methodology for sample collection should be provided. This includes the description of the sampling device, the collecting surface material, the volume of the dead space (if possible), the duration and temperature of collection, breathing pattern, use of noseclip and route of inhalation, method and duration of sample storage. Additionally, intra-assay and inter-assay variability of the assay technique, and intra-subject variability of the mediator should be reported. Lastly, details on participants should contain information on upper airway disease, smoking habit, and medication.
MEASUREMENTS OF MEDIATORS IN EBC
Storage of EBC samples
Because on-line measurements are not available for most mediators present in EBC with the exception of a few assays including those for pH and H2O2, EBC samples are usually stored before mediator measurements.
EBC samples should be immediately frozen after collection and stored at −70°C until mediator determination is performed. It is advisable to test the stability of mediators at the storage temperature if not published previously. Assays clearly should be performed well within the time period that the biomarker is known to be stable. There have been no comparisons between samples “immediately snap-frozen” and then placed into the -70 degrees freezer or those placed to the freezer as collected. If it is planned that more than one mediator will be determined from the obtained EBC sample, samples should be stored in separate tubes to avoid multiple frosting-defrosting cycles which could destroy certain mediators, such as prostaglandins, leukotrienes and H2O2. Even when stored under these conditions, some mediators are not stable after long-term storage. For example, the concentration of H2O2 is known to decrease causing detectable change in its level after a few days. Cysteinyl-leukotrienes (cys-LTs) are also unstable compounds in most biological fluids, although data on their stability in EBC is not available. On the other hand pH has been reported to be stable up to 2 yrs of storage. To avoid difficulties with storing, some research groups employed a method in which they added the obtained EBC sample immediately to a reaction mixture and stored the EBC with the now stable reaction product until measurement 58–60.
Rationale for measurement of mediators
EBC sampling is performed with three major aims: 1) to learn more about the pathological mechanisms of airway diseases by detecting changes in mediator levels; 2) to learn more about the composition of the airway lining fluid; and 3) to use the determined mediators as exhaled biomarkers of airway diseases.
H2O2
Source
H2O2 is produced after converting superoxide anions O2•− to H2O2 by superoxide dismutase in several cell types 15, 61. In the respiratory system H2O2 may be released both from inflammatory and structural cells including neutrophils, eosinophils, macrophages and epithelial cells. H2O2 is a volatile molecule, which has been demonstrated in EBC by several investigators 4.
Protocols, recommendations and potential pitfalls
H2O2 in EBC is unstable, therefore, EBC should be rapidly frozen after collection and kept at ≤−70°C until the determination of its peroxide concentration. Different data have been published on the stability of H2O2 in frozen EBC samples varying between from 2–3 days to 2 months 33, 46. One option to circumvent the problem of instability is to add assay reagents immediately after collection of EBC and store the stable reaction product frozen until the measurement 58. Saliva contains 10–100-fold higher H2O2 concentration than EBC, therefore, exclusion of saliva is of great importance. Nasal and oral EBC collection have been compared and showed that the two methods are not interchangeable when measuring this mediator 38.The most frequently used methods of measuring H2O2 in EBC are the colorimetric or fluorimetric measurements, which are based on the ability of H2O2 to react with suitable substrates 4, 15. The lower limit of detection with the fluorimetric method is 0.1 μm·L−1, but in one study a lower detection limit (0.005 μm·L−1) was reported by using automated flow injection to detect the fluorescence of the reaction product 62. Most groups have reported 0.1 μm·L−1 as the detection limit for the colorimetric assay 45, but one recent study used 0.31 μm·L−1 for detection limit 63. Values presented both for healthy individuals and patients with different respiratory disorders vary widely, most of them are close to the lower limit of detection and often include zero (see more details below). Data on reproducibility have not been given in many publications and the reported values vary between studies showing quite good agreement of data 62, 64, 65 or a rather high coefficient of variation within repeated measurements 19, 34, 63. The mean coefficient of variation over 21 days was 45% in COPD patients and 43% in healthy subjects 34. Due to the variability of data, concern has been raised regarding the reproducibility of the colorimetric assay in the range of values found in EBC and the usefulness of this measurement for monitoring oxidative stress in the airways 15, 36, 63, 66. Therefore, the use of more sensitive methods is advisable for peroxide measurement and further studies are required to establish the usefulness of other methods (i.e. chemiluminescence or other) for H2O2 measurements in EBC 59, 67–70.
Diseases states that influence H2O2
In healthy, young, nonsmoking individuals H2O2 levels diverge from 0 to 0.9 μmol·L−1. Higher H2O2 concentrations were found in healthy elderly persons, smokers and ex-smokers 13. A correlation between age and H2O2 concentration has also been reported. Furthermore, a circadian rhythm of exhaled H2O2 was shown in healthy subjects with highest levels at 12:00 and 24:00 h and also in patients with COPD 13. Increase in EBC H2O2 level was found in asthma 22, 58, 60, 71–73, healthy smokers 35, 39, COPD 34, 44, 45, 59, 65, 74, 75, bronchiectasis 76, 77, CF 78, 79 and acute respiratory distress syndrome (ARDS) 5, 80, 81, acute hypoxaemic respiratory failure 14, reperfusion injury 82, allergic rhinitis 83, common cold 84, post-operative period after lung resection 85, systemic sclerosis 86 and in experimental models of hypoxia/reoxygenation 87, 88.
In asthma, levels were related to the eosinophil differential counts in induced sputum and also to airway responsiveness 22. In patients with exacerbations higher peroxide levels were reported than in patients with stable disease and treatment with corticosteroids lowered its concentration, but no change was reported after treatment with montelukast 58, 72, 73.
Expired H2O2 level was shown to be elevated both in healthy smokers 39 and also in patients with COPD compared with values from healthy nonsmokers with no significant difference between their values 44–46. In COPD patients with exacerbations, higher levels of expired H2O2 were found than in patients in stable condition 45. Inhaled steroids had no effect on H2O2 level in this disease in some studies 45, 74, but caused a decrease in another investigation 89. Long-term antioxidant treatment with N-acetylcysteine decreased exhaled H2O2 concentration in patients with COPD 75. Experimental data using a horse model of COPD showed a positive correlation between H2O2 in EBC and the numbers of neutrophils in BAL fluid indicating the significant relationship between H2O2 in EBC and the degree of inflammation 90.
EBC H2O2 concentrations were elevated in bronchiectasis with a significant inverse correlation between lung function and exhaled H2O2 level 76, 77. In CF an increase in exhaled H2O2 concentration has also been described, although not consistently 64, 78, 79. Treatment with antibiotics caused a decrease in H2O2 level in CF 79.
Level of validation
Independent groups confirmed the presence of H2O2 in EBC using different assay techniques, and have reported day to day intra-subject coefficient of variation is 43% in healthy subjects 33.
Nitrogen oxides and related products
Nitrite/nitrate
Source
Nitrite (NO2−) and nitrate (NO3−) are nitrogen redox forms that are present in the epithelial lining fluid of the human respiratory tract. The term nitrogen oxides (NOx) incorporates these two ions, as well as other oxides of nitrogen.
Protocols, recommendations and potential pitfalls
NO2− and NO3− have been detected in EBC by using spectrophotometric assays (Griess reaction), a fluorimetric method (2,3-diaminonapthalene (DAN) reaction), chemiluminescence assays or ion chromatography followed by conductivity measurement 91–104. The reported detection limit of the DAN assay is 0.1 μM and that of the Griess reaction is higher 91, 92. NO2− tends to be found in condensate in the 1 μM range, which is, therefore, close to the detection limit for these assays. Data on day-to-day reproducibility has not been published. The chemiluminescence technique is sensitive in the nM range and NO2−/ NO3− have been detected by this method in BAL 93, 94. Caution must be taken when interpreting NO2− assays, as the compound cannot be considered stable at low pH, and even at neutral pH. NO3− is considered stable. NO3− levels tend to be roughly 5–10 fold higher than NO2− levels, although this may vary in part because of changes in airway oxidative conditions. Since most combined NO2−/ NO3− assays rely on the formation of NO2− from NO3−, variability of data may arise partially from differences in the efficacy of the reduction method chosen. In this respect, enzymatic reduction was found to be better for NO3− determination in EBC than cadmium reduction 95.
NOx are present on every laboratory surface, including glassware and pipette tips. Therefore, investigators should take great precautions to avoid contamination of the sample. Experience suggests that it is necessary to thoroughly rinse with highly pure (distilled/de-ionised) water any material that might come in contact with EBC, including devices used for collection, processing and assaying EBC. It is best to perform this rinsing very soon before use, because readily diffusible ambient NO becomes oxidised and contaminates surfaces rapidly.
Diseases states that influence nitrite/nitrate concentration in EBC
Concentrations of NO2 and/or NO2+NO3 were found to be significantly higher in asthma, CF and bronchiectasis compared with healthy controls 18, 96–99, 101, 102, but in mild asthma and CF some studies showed no increase 91, 103, 105. In smokers both increases and normal concentrations of EBC NO2 have been described 40, 42, 103. In patients with exacerbations of asthma, higher NO2− levels were observed compared with stable patients and treatment with inhaled steroids resulted in a significant decrease in its concentration 96, 98. In children with asthma and CF higher EBC NO2− levels were found than in children with nonasthmatic, episodic cough 98. In CF, NO2− level in EBC was elevated or normal in contrast to decreased level of exhaled NO 18, 91, 92. Similarly, in primary ciliary dyskinesia (PCD), a genetic disorder associated with low levels of exhaled NO, normal NO2− levels were described in EBC 106. The dissociation between exhaled NO levels and EBC NO2− concentrations observed in CF, PCD and smoking healthy subjects emphasise further the need for more research on biochemical changes in the airway walls. Conflicting reports of exhaled NO3− concentrations have been published showing unchanged or increased NO3− levels in different airway conditions 101, 102. EBC NO2− level was demonstrated to be elevated in patients with acute lung injury 107.
Level of validation
Independent groups confirmed the presence of NO2−/ NO3− in EBC using different assay techniques. There are no reported data on day-to-day intra-subject coefficient of variation.
Nitrotyrosine
Source
The reaction of NO and superoxide anions in the airways leads to the formation of peroxynitrite, which is a highly reactive oxidant species. Peroxynitrite reacts with tyrosine residues of proteins to form the stable product nitrotyrosine, which may be detected with specific antibodies 108.
Protocols, recommendations and potential pitfalls
EBC nitrotyrosine has been measured by specific enzyme immunoassay (EIA), which has a detection limit if 3.9 ng·mL−1. Nitrotyrosine has not been detected in all EBC samples (not even when samples were concentrated three-fold). The range of nitrotyrosine concentrations in EBC of healthy subjects is 0–14 ng·mL−191, 108. Day to day variability was reported on seven healthy subjects finding a coefficient of variation of 6% 91. Using mass spectrometry (MS) technique nitrotyrosine can be measured in picomolar range 109. Although not universally recognised, the commercial ELISA assays (which are sandwich ELISAs) presumably quantify proteins nitrated at more than one site, rather than single amino acids. Thus, when nitrotyrosine levels are reported from sandwich ELISA assays, what likely is meant is that nitrated proteins are present.
Disease states influencing nitrotyrosine concentration in EBC
Nitrotyrosine concentrations were found to be increased in patients with asthma compared with healthy controls with a relation between exhaled nitrotyrosine and NO levels in these patients 109. In CF patients, levels of EBC nitrotyrosine were also elevated, despite the normal level of NO2− and NO3− and a decreased level of exhaled NO in these patients as compared with those of normal subjects 91. An inverse correlation between the levels of nitrotyrosine and the severity of lung disease was also found in this study 91.
Level of validation
Only one research group demonstrated the presence of nitrotyrosine in EBC using different assay techniques in two separate studies. Reported day-to-day intra-subject coefficient of variation is 6% in a small group of healthy subjects 91.
Nitrosothiols
Source
Nitrosothiols (RS-NOs) are formed by interaction of NO or NO2− with gluthatione or other thiol containing molecules 110, 111.
Protocols, recommendations and potential pitfalls
RS-NOs can be measured using commercially available colorimetric assay kit 103. The assay is based on the cleavage reaction of RS-NOs releasing NO, which is then oxidised to NO2−, which is detected by the kit. The reported detection limit of the kit is 0.025 μM. Nitrosothiols can be more sensitively detected using chemiluminescence analysis after reduction to NO in copper-cysteine or by ultraviolet light 104. RS-NOs level in EBC of healthy subjects is 0.05–0.8 μM 103, 106. Data on reproducibility have not been reported.
Diseases states that increase RS-NO concentration in EBC
Concentration of RS-NOs was found to be increased in patients with inflammatory airway diseases, including asthma and CF, values vary between 0.05–1.25 μM 103, 106.
Level of validation
Only one research group demonstrated the presence of nitrosothiols in EBC using the same assay technique in two separate studies, there are no reported data on day-to-day intra-subject coefficient of variation.
Adenosine
Source
Adenosine is formed during the degradation of adenosine triphosphate (ATP) and has a wide range of effects in the respiratory system through its specific receptors 112.
Protocols, recommendation and potential pitfalls
EBC adenosine can be determined by HPLC. The method used for plasma adenosine measurement has been validated for EBC 20, 113. The detection limit of the method is 2 nmol·L−1 (signal to noise ratio at least 3:1) The inter-assay reproducibility of EBC adenosine measurement was found to be <10% 11, 20. The range of healthy adenosine values was found to be between 0–20 nmol·L−1; EBC levels were several-fold lower than those in plasma or BAL, however, taking dilution factor of EBC into account EBC and BAL adenosine values resulted in similar airway concentrations 114, 115.
Disease states that increase EBC adenosine concentrations
EBC adenosine level was found to be elevated in patients with allergic rhinitis 11 and in asthmatic patients with substantial overlap with healthy values in both conditions 20. In patients with worsening of asthma symptoms, EBC adenosine concentration was higher than in stable disease and adenosine level in EBC showed a positive correlation with exhaled NO concentration in asthma 20.
Level of validation
Only one research group demonstrated the presence of adenosine in EBC using the same assay technique in different studies. Mean intra-day coefficient of variation is 10% in healthy subjects 20. There are no reported data on day-to-day intra-subject coefficient of variation.
Arachidonic acid metabolites
Prostaglandines and thromboxanes
Source
Arachidonic acid, released from the cell wall by phospholipase A2, is converted to prostaglandin endoperoxides by cyclo-oxygenase. Endoperoxides are then converted to prostaglandins, prostacyclin and thromboxane A2 (TXA2) 116. TXA2 is rapidly converted to TXB2, a chemically stable but biologically inactive metabolite (one of the further metabolic processes TXB2 undergoes is the common β-oxidation resulting in the formation of 2,3-dinor TXB2). Thus, thromboxane synthesis in biological tissues has been monitored by measuring TXB2.
Protocols, recommendations and potential pitfalls
Prostoglandin E2 (PGE2) and TxB2 can be measured by EIA and also by radioimmunoassay (RIA) 11, 117–120. The specificity of PGE2 measurement by RIA has been validated by reverse phase HPLC 118. The detection limit of the EIA for TxB2 is 13 pg·mL−1 and that of the RIA is 13.6 pg·mL−1. While TxB2 was detected only in a small part of EBC samples by EIA 119, higher TxB2 values were found by RIA (normal range between 0–200 pg·mL−1) 11. The observed difference is likely attributable to the 100% cross-reactivity of the RIA assay, but not the EIA method, with 2,3-dinor- TxB2. The difference in specificity between the two kits, therefore, needs to be taken into account when comparing data. Reproducibility data have not been published on TxB2 measurements. The detection limit for PGE2 (EIA) is 8 pg·mL−1, the repeatability data showed an intra-class correlation coefficient of 0.79 120.
Diseases states that influence eicosanoid concentration
No significant differences were found in exhaled PGE2, PGD2 and TxB2 levels between healthy subjects and patients with asthma, whereas PGE2 concentrations were found to be increased in EBC in patients with COPD and in asthmatic smokers 120–122.
Level of validation
Independent research groups demonstrated the presence of PGE2, PGD2 and TxB2 in EBC using different assay techniques, there are no reported data on day-to-day intra-subject coefficient of variation.
Leukotrienes
Source
The Cys-LTs (leukotriene (LT)C4, LTD4, LT4) are released from inflammatory cells of the airways, particularly mast cells and eosinophils, and play a role in asthmatic airway inflammation 123. LTB4 is formed from arachidonic acid as a result of enzymatic hydrolysis of LTA4, a potent activator of neutrophils and a proinflammatory mediator 124.
Protocols, recommendations and potential pitfalls
Cys-LTs (LTC4/D4/E4) and LTB4 can be measured by EIA with detection limit of 15 pg·mL−1 and 4.4 pg·mL−1, respectively 30, 125–132. The range of cys-LT concentrations in EBC of healthy subjects varies between 0–25 pg·ml−1 and that of LTB4 is between 0–220 pg·mL−1 73, 109, 125–132. In one study authors could not detect cys-LTs at all in EBC 73. The specificity of the immunoreactivity of the LTB4 EIA assay was confirmed by using reverse-phase high performance liquid chromatography 133. The correlation coefficient for two repeated LTB4 measurements was 0.76 133.
Diseases states which influence LT concentrations
An elevation in exhaled LTB4 level was demonstrated in calves after experimental respiratory tract infection 30. Cys-LTs and LTB4 were found to be elevated in asthmatic patients as compared with normal subjects 109, 117, 125–128. Furthermore, elevated concentration of cys-LT found during exacerbations in asthmatic children was decreased significantly after prednisone treatment 126. In COPD, LTB4 was increased in the stable state and further increased during exacerbations and decreased following antibiotic treatment 129. An increased concentration of LTB4 was also found in CF patients 130 and in patients undergoing lobectomy, but not after cardiopulmonary bypass 48.
Level of validation
Independent research groups demonstrated the presence of Cys-LTs and LTB4 in EBC using different assay techniques. Reported day to day intra-subject coefficient of variation for LTB4 is 2% in a small group of healthy subjects 125.
8-isoprostane
Source
8-isoprostane, a stable prostaglandin-like product, is formed from arachidonic acid by the nonenzymatic action of reactive oxygen species, and, therefore, it is suggested to be a marker of oxidative activities and oxidative stress 134.
Protocols, recommendations and potential pitfalls
Most studies used commercial EIA kits to measure 8-isoprostane with a detection limit of 3.9 pg·mL−1 to detect 8-isoprostane in EBC 17, 128, 129, 135, 136. The assay was validated directly by gas chromatography/MS showing high correlation between added known amounts of 8-isoprostane and the concentration measured with the EIA 118. 8-isoprostane levels in EBC samples from healthy subjects varied between zero and 40 pg·mL−1 and the average concentration given in different studies show pronounced differences. Reproducibility of this assay has been determined by different groups with contradictory results 63, 65. A more sensitive and specific method to assay EBC isoprostane is gas chromatography/MS. Using this method Carpenter et al. 16 found 8-isoprostane only in some healthy subjects, but Moloney et al. 48 presented data demonstrating detectable level of this molecule in EBC from all subjects tested.
Disease states influencing 8-isoprostane concentration in EBC
8-isoprostane concentration was found to be elevated in asthma 17, 117, 121, 126, 128, COPD 41, 129, interstitial lung disease 135, CF 136, ARDS 9, pulmonary sarcoidosis 137, obstructive sleep apnoea 138, and also in healthy subjects after ozone-inhalation 139. In asthma, the increase observed in EBC 8-isoprostane level was related to the severity of the disease and a relative resistance of 8-isoprostane to steroids has been reported in children with asthma exacerbation 17, 121, 126, 128. 8-isoprostane was also found to be increased during COPD exacerbation and decreased after treatment 40, 129.
Level of validation
Independent research groups demonstrated the presence of 8-isoprostane in EBC using different assay techniques. There are no reported data on day to day intra-subject coefficient of variation.
Other markers of oxidative stress
Source
Aldehydes (malondialdehyde, 4-hydroxyhexanal, 4-hydroxynonenal, hexanal, heptanal and nonanal) are lipid peroxides which reflect oxidant-induced damage 21. Conversely, reduced glutathione reflects the antioxidant capacity 140.
Protocols, recommendations and potential pitfalls
Measurement of thiobarbituric acid-reactive substances is a simple, but nonspecific method for the assessment of lipid peroxidation, therefore, it is not recommended as a marker of lipid peroxidation 44.
Aldehydes were detected in EBC using liquid chromatography-tandem MS which had a detection limit for different aldehydes between 0.31–1.07 nM 21, 141. Glutathione was determined by high performance liquid chromatography with fluorescence detection with a detection limit of 2.0 nM 142. The range of aldehydes in healthy subjects was between 15–55 nM and that of reduced glutathione was 11–17 nM. The mean coefficient of variation (%) of aldehyde measurements in EBC was between 12–20% for the different aldehydes. Oxidised glutathione has been reported to be below detection limits in EBC.
Disease states that influence aldehyde and gluthatione concentrations
In asthma elevated aldehyde levels and decreased glutathione levels were detected in patients with exacerbations and these values returned towards the levels found in normal subjects after appropriate treatment 142. Furthermore, levels of aldehydes were also increased in COPD 21.
Level of validation
Only one research group demonstrated the presence of glutathione in EBC in one study. The presence of aldehydes in EBC was also demonstrated only by one group in two studies using the same assay techniques in both studies. Reported day to day intra-subject coefficient of variations for different aldehydes are between 12–20% 142. There are no reported data on day-to-day intra-subject coefficient of variation on EBC glutathione.
pH
Source
Airway pH homeostasis is maintained by a balance of different buffer systems and the production and release of acids and bases in the airways.
Protocols, recommendations and potential pitfalls
The acidity (pH) of EBC can be readily measured with pH electrodes and indicator dyes 12, 143. In healthy subjects, the pH of EBC immediately tested tends to be unstable. To enhance the stability of the readings, de-aeration (gas standardisation) with a CO2 free gas (such as argon, nitrogen oxygen or another CO2-free gas) can be performed. During de-aeration, the pH gradually rises to a point when stable reading can be obtained (at this point, no further CO2 can be removed by de-aeration). In healthy subjects, EBC pH after de-aeration has a mean pH of 7.7, with a range of normal considered by the investigators to be 7.4–8.8. These values are obtained from orally collected EBC samples. From intubated subjects without lung disease, the mean pH of de-areated samples is likewise 7.7 with no difference from matched oral collections 12. In another study, the pH of EBC samples from intubated subjects undergoing cardiothoracic surgery was reported to be between 5–7 48. There is a debate as to whether orally collected EBC pH assays reflects acidification of the lower airways, because of high ammonia content of the mouth 144 conceivably interferes with the assay. However, this concern has not been proven. Extensive data do not reveal an effect of oral ammonia on EBC pH assays 145. Intra-day and intra-week coefficients of variation of EBC pH measurements in healthy subjects are reported to be 3.5% and 4.5% respectively 12. The pH of de-areated EBC is not affected by hyperventilation, duration of collection (3–7 min), duration or manner of storage (up to 2 yrs), oral versus endotracheal collection, exclusion of oral ammonia (a base), or acute airway obstruction with methacholine 12.
Disease states that influence EBC pH
Up to three log order decreases in EBC pH have been described in acute asthma 102, 143, CF 146, COPD, bronchiectasis 102 and acute lung injury 48, 147. In asthma, pH rose back to normal after successful treatment with steroids 143. Furthermore, pH levels were related to eosinophilic or neutrophilic inflammation of the airways 102. At the moment no published data are available on direct comparison of EBC pH values and pH measured directly in the airways.
Level of validation
Independent research groups confirmed that pH is easily assayed in EBC and data are reproducible. Reported day to day intra-subject coefficient of variation of EBC pH is 4.5% 12.
Ammonia (NH3/NH4)
Source
Ammonia produced during the urease hydrolysis and/or glutaminase activity in the airways may have important functions, including pH regulation 148.
Protocols, recommendations and potential pitfalls
Ammonia is a volatile compound, and collection temperature and duration influences its level in EBC. NH4+ can be readily measured spectrophotometrically in EBC 148. Most of EBC ammonia arises from the mouth 6, 11, 53.
Disease states that influence ammonia concentration in EBC
The concentration of ammonia in EBC was found to be between 14–1220 μM in healthy subjects and is lower in asthma 147. It has been suggested that the decreased level of exhaled ammonia in asthma reflects reduced pulmonary production 147, but this has been disputed 149. Previous observations showed that the pH of the mouth has a profound effect on the release of NH3 into the exhaled air 150.
Level of validation
Independent research groups demonstrated the presence of ammonia in EBC by different assay techniques. Mean intra-day coefficient of variation is 60% with a broad range from 10–180%. Intra-week coefficient of variation of 64%, with a similarly broad range of variabilities 145.
Cytokines
Source
Inflammatory cells and structural cells of the pulmonary system are all able to form different cytokines 151.
Protocols, recommendations and potential pitfalls
Cytokine concentrations in EBC samples are usually quantified by EIA/ELISA kits. The manufacturer's description provides a detection limit and also an intra- and inter-assay variability. Caution must be taken when using these methods, because the concentration of several cytokines are at around the lower limit of detection in unconcentrated EBC samples, where variability is higher than the values given in the manuals (values may fall out of the linear range of the standard curve). To circumvent this problem samples can be concentrated before measurement. Assurance of the validity of these assays using EBC samples is not ascertained. Several different cytokines have been described to be present in EBC 7, 42, 64, 138, 152–156, although some of them, such as IL-8 could only be detected in small proportion of subjects 64 and values often include zero.
Disease states that influence cytokine concentrations
Increased levels of IL-4 and a decreased level of interferon-γ were described in EBC of asthmatic children 152. Steroid treatment was associated with a significant reduction in IL-4 and an elevation in interferon-γ concentration in exhaled condensate. IL-6 is elevated in nonsmall cell lung cancer patients 153, obstructive sleep apnoea 138, COPD 154, CF 130 and in cigarette smokers 155. Ischaemia-reperfusion was found to be associated with increased IL-10 concentrations in EBC 156. IL-1β was also detected in EBC 42.
Level of validation
The presence of IL-8 and IL-6 has been demonstrated by different authors, other ILs were demonstrated only once. Reported day to day intra-subject coefficient of variation of IL-6 is 5.9% in healthy subjects 130.
Other molecules/materials
EBC contains other molecules/characteristics that can provide important information including p53 mutation 157, 158, DNA 7, 49 hepatocyte growth factor 159, vitronectin, endothelin-1 160, chemotactic activity 42. The protein content of EBC was found to be different between samples from healthy subjects and those from smokers 42 or patients with COPD 28. EBC collection may also be useful for rapid detection of infectious processes in the lung using PCR technology, such as tuberculosis 49, 161.
Level of validation
Total protein content was reported by independent research groups using different techniques. The other molecules were demonstrated only by one group. There are no reported data on day to day intra-subject coefficient of variation on these mediators.
Summary of mediator measurements
Mediators/features determined in EBC represent a wide range of variables from protons to DNA fragments. Due to their diverse biochemical features (volatility, stability, molecular weight, etc.) each of them requires special considerations when measured in EBC. According to the current evidence the measurement of EBC pH is the most easy and reproducible test in EBC. Concentration of some volatile substances (i.e. ammonia) can vary widely. Assay systems are often the limiting factor for biomarkers found at lower concentrations, with assay limitations contributing substantially to sample variability. Validation of individual biomarkers in EBC has been a slower process than that for exhaled NO for the simple reason that there are so many compounds to study in EBC.
General summary
EBC analysis addresses important medical research needs by enabling noninvasive assessment of biochemical and inflammatory parameters in the airway. This technique holds promise for clinical applicability. However, this approach still has several unresolved questions. Analysis of EBC is not limited to patient monitoring and understanding mechanisms of pulmonary disease. It also could become a useful tool for monitoring and screening of healthy individuals for possible early pulmonary tissue damage. EBC collection is a completely noninvasive way of sampling the respiratory tract that can be repeated frequently within short intervals without adverse events with good reproducibility in EBC volume and mediator concentration for several tested markers including pH, H2O2, adenosine, 8-isoprostane 11, 12, 19, 20, 28, 32, 34, enabling the method to be used both for demonstrating short-term effect of interventions (i.e. acute effect of smoking, medications) and also in longitudinal studies. Collection devices can be portable and can be used in a wide range of settings including intensive care units (mechanically ventilated patients), outpatient clinics and home.
Currently available assay techniques are not sensitive enough for many biomarkers, contributing to reported variability. Many assays are laborious and time-consuming. As yet no fully validated method for calculating dilution of respiratory droplets is available and the anatomic origin of biomarkers is not precisely known. These and the other unsolved issues regarding this technique limited the present Task Force recommendations to several aspects of the technique. Therefore, its primary aims could not be fully met. There is agreement on the recommendations that could be made based on the currently available evidence (or in some cases based on the consensus of the expert panel), clear consensus on areas of uncertainties, and delineation of needed further studies. Not surprisingly, the Task Force group was faced with many of the same problems and limitations associated with other methods of sampling the airways (sputum induction, BAL, and exhaled NO) 2, 57, 162. The number of original publications and reviews on EBC analysis 23, 24, 163–173, and presentations at international conferences has increased sharply in recent years with editorials and correspondences in respiratory journals debating the value of this sampling method 144, 149, 174–181. The rapid expansion of research on EBC is reflected by the fact that during the ATS/ERS evaluation and approval of this Task Force report >40 publications appeared using this method in peer-reviewed journals 182–228. The Task Force considered it important to put together this report summarising their current understanding of the technique, and also the limitations of their knowledge, in the hopes of catalysing research that improves the methodologies and to find the proper place of this sampling method both in research and clinical practice.
FUTURE DEVELOPMENTS
It is clear that EBC contains many potential biomarkers. It is now important to optimise their measurement and study the clinical value of monitoring biomarkers in the breath in a variety of lung diseases and to establish the reproducibility of these measurements. This is a complex task as each biomarker needs to be considered individually because of differing solubility, stability, volatility and amount.
One of the current limitations of EBC measurements is the low concentration of many biomarkers so that their measurement is limited by the sensitivity of assays. It is likely that ever more sensitive assays will be available as more potent antibodies are developed and new molecular detection techniques are introduced. Metabonomics is a recent technique that may be particularly applicable to EBC analysis. Metabonomics involves the detection of hundred of thousands of metabolites in a biological fluid usually using high resolution nuclear magnetic resonance spectrometry or liquid chromatography/MS. Powerful pattern recognition computer programs recognise patterns of metabolites that are sensitive to disease, effects of treatment and disease severity. Metabonomics of EBC (a “breathogram”) may, therefore, prove to be useful in screening lung diseases, following disease progression, predicting responses to treatment and in monitoring of response to therapy 229, 230.
One relative disadvantage of EBC measurements is that they require a subsequent analysis and it is likely that there will be important advances in on-line detection of particular biomarkers using sensitive biosensors. For example, it is possible to detect H2O2 on-line (real-time) using a silver electrode or by coating a platinum electrode or polymer with horseradish peroxidase 69, 70, 231. Similar enzyme detector systems may also be developed for real-time monitoring of various lipid mediators, including 8-isoprostane. It is relatively easy to monitor pH of EBC and this is readily amenable to real-time detection. Several molecular biosensors are now in development and have the potential to detect very low concentrations of various relevant biomarkers. Ultimately it may be desirable to collect EBC to monitor patients in clinical practice using disposable detector sticks.
Proteomics, which applies high resolution gel electrophoresis or MS to detect multiple proteins in biological samples, may also be a useful approach to analysis of the proteins in EBC. This may reveal disease-specific patterns and may lead to the identification of novel proteins for detection of disease and identification of new therapeutic targets. However, there are several technical problems that need to be overcome before this becomes a useful approach.
It is clear that exhaled breath condensate is an exciting new approach to monitoring lung diseases that may have great potential in the future. These guidelines provide the first step in standardising measurements and encouraging research in this new field.
Summary of recommendations for EBC analysis
Acknowledgments
Task Force participants (who attended one or more meetings). Those participants who helping in the writing up of the Report are listed as co-authors: K. Alving (Stockholm, Sweden); A. Antczak (Lodz, Poland); B. Balint (Deszk, Hungary); E. Baraldi (Padova, Italy); G. Becher (Berlin, Germany); W.J.C. van Beurden (Nijmegen, Netherlands); A. Blomberg (Umea, Sweden); M. Corradi (Parma, Italy); R. Dekhuijzen (Nijmegen, Netherlands); R.A. Dweik (Cleveland, OH, USA); T. Dwyer (Jackson, MS, USA); R. Effros (Milwaukee, WI, USA); S. Erzurum (Cleveland, OH, USA); J. Freels (Tucson, AZ, USA); B. Gaston (Charlottesville, VA, USA); C. Gessner (Leipzig, Germany); M. Goldman (Los Angeles, CA, USA); A. Greening (Edinburgh, UK); L.P. Ho (Oxford, UK); J.M. Hohlfeld (Hannover, Germany); J. Hunt (Charlottesville, VA, USA); Q. Jöbsis (Maastricht, Netherlands); S.A. Kharitonov (London, UK); F. Kelly (London, UK); D. Laskowski (Cleveland, OH, USA); C. Lehmann (Hannover, Germany); A. Lindstrom (Research Triangle Park, NC, USA); S. Loukides (Athens, Greece); D. Marlin (Kentford, UK); P. Montuschi (Rome, Italy); A-C. Olin (Gothenburg, Sweden); A.E. Redington (Hull, UK); P. Reinhold (Jena, Germany); E.L.J. van Rensen (Leiden, Netherlands); R. Robbins (Tucson, AZ, USA); M. Rothe (Freiburg, Germany); I. Rubinstein (Chicago, IL, USA); P. Silkoff (Denver, CO, USA); H-J. Smith (Gauting, Germany); W.R. Steinhaeusser (Marburg, Germany); W.G. Teague (Atlanta, GA, USA); K. Toren (Gothenburg, Sweden); G. Vass (Budapest, Hungary); J. Vaughan (Charlottesville, VA, USA); C. Vogelberg (Dresden, Germany); and H. Wirtz (Leipzig, Germany).
Footnotes
-
For editorial comments see page 371.
- Received March 14, 2005.
- Accepted April 28, 2005.
- © ERS Journals Ltd
References
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵
- ↵









