





Abstract
The study was designed to assess the patterns of use of home mechanical ventilation (HMV) for patients with chronic respiratory failure across Europe.
A detailed questionnaire of centre details, HMV user characteristics and equipment choices was sent to carefully identified HMV centres in 16 European countries.
A total of 483 centres treating 27,118 HMV users were identified. Of these, 329 centres completed surveys between July 2001 and June 2002, representing up to 21,526 HMV users and a response rate of between 62% and 79%. The estimated prevalence of HMV in Europe was 6.6 per 100,000 people. The variation in prevalence between countries was only partially related to the median year of starting HMV services. In addition, there were marked differences between countries in the relative proportions of lung and neuromuscular patients using HMV, and the use of tracheostomies in lung and neuromuscular HMV users. Lung users were linked to a HMV duration of <1 yr, thoracic cage users with 6–10 yrs of ventilation and neuromuscular users with a duration of ≥6 yrs.
In conclusion, wide variations exist in the patterns of home mechanical ventilation provision throughout Europe. Further work is needed to monitor its use and ensure equality of provision and access.
- Chronic obstructive pulmonary disease
- chronic respiratory failure
- Europe
- home mechanical ventilation
- neuromuscular disorders
- noninvasive ventilation
Home mechanical ventilation (HMV) for patients with chronic respiratory failure is an important, growing and successful technique for reducing morbidity and mortality, especially in those with chest wall and neuromuscular disease 1–3. The expansion in its use in the last 15 yrs was stimulated by the introduction of noninvasive ventilation via a mask and the recognition that more patient groups could benefit. Previous surveys of HMV have highlighted the experience of France 3, Italy 4, and Scandinavia 5. A pan-European survey published in 1992, however, found that the collection of information about HMV was incomplete and erratic in many countries and it was not possible to detail many aspects of its use due to the lack of documentation 6.
The aim of the present study was to perform a detailed survey of HMV use in 16 European countries and thereby identify patterns of its use in different countries and settings.
METHODS
HMV definition
For the purposes of the survey, HMV was defined as noninvasive ventilation or ventilation via a tracheostomy for a period of ≥3 months on a daily basis carried out mostly in the user's home or other long-term care facility (not a hospital). It did not include patients with obstructive sleep apnoea alone, or patients with a tracheostomy not requiring mechanical ventilation. Negative pressure ventilation, phrenic nerve stimulation and the use of ventilatory adjuncts, such as rocking beds, were included.
Centre identification
For each country, a National Representative was invited to participate in the survey. These consisted of leading clinicians nationally renowned in the field of HMV (see Acknowledgements). Their initial task was to identify as many HMV centres as possible in their country. HMV centres were defined as any hospital or outpatient unit that initiated or prescribed HMV and/or co-ordinated HMV services. Various methods were used for this process depending on the situation in each country. Registers of HMV centres and users were available in some countries (Sweden, Denmark, The Netherlands, Belgium), whilst others used information from previous surveys, national organisations and personal knowledge.
Unless the lists of centres and user numbers were thought to be complete, National Representatives were asked to conduct a preliminary centre identification process with a one-page questionnaire sent to all potential centres covering respiratory, intensive care, neurology and paediatric specialities. This questionnaire asked whether the centre had any HMV users and, if so, how many. At completion of this process, an estimate of the number of centres, users and the national prevalence was possible. Prevalence rates were calculated from population statistics for 2001 provided by each National Representative. From these estimates, an approximate response rate of completion of the full survey was also made possible.
Survey content
A draft of the survey was written by the co-authors and sent to all the National Representatives for comments prior to a meeting of all parties in June 2001 where each definition, section and question was modified to ensure that the final survey would accurately collect data on the practices in each country. The final survey was identical in each country and was translated appropriately. The survey included questions about the centre itself (type of institution and year of starting HMV), the number of HMV users on July 1, 2001, and basic, pooled details about their users, such as sex ratio, age ranges and the time on HMV in yrs. The survey also asked for details of the users' causes for respiratory failure, divided into three disease categories: 1) Lung: lung and airway diseases: chronic obstructive pulmonary disease (COPD), cystic fibrosis, bronchiectasis, pulmonary fibrosis and paediatric diseases, including bronchopulmonary dysplasia; 2) Thor: thoracic cage abnormalities: early-onset kyphoscoliosis, tuberculosis sequelae such as thoracoplasty, obesity hypoventilation syndrome and sequelae of lung resection; 3) Neur: neuromuscular diseases: muscular dystrophy, motor neurone disease (including amyotrophic lateral sclerosis), post-polio kyphoscoliosis, central hypoventilation, spinal cord damage and phrenic nerve paralysis.
A subsequent section requested a breakdown of the type of ventilator and interface currently used for the patients in each disease category.
Survey distribution and collection
Surveys were sent out by the National Representatives to all centres from July 2001 onwards with a covering letter of explanation. Two written reminders were sent out to centres not returning surveys, followed up by one telephone reminder. Completed surveys were returned to the National Representatives where copies were made and the originals sent to the data collection centre in London, UK. The deadline for receipt of the completed surveys was June 1, 2002.
Data entry and analysis
All data relating to centres, and therefore users, was coded and kept strictly confidential. Data was summarised for each country using nonparametric statistics and are presented as median (interquartile range, unless otherwise indicated). Spearman's rank correlations were used to identify relationships in various centre and user characteristics. Chi-squared tests were utilised were the variable had a binomial distribution. Individual centre data was also analysed nonparametrically in a similar fashion. Paediatric centres and French Associations were not included in the centre analysis as they were at the extremes of centre size and would have biased the relationships.
RESULTS
Estimated prevalence
The estimated prevalence of HMV was 6.6 per 100,000 people in the 16 European countries surveyed. Table 1⇓ shows the estimated number of centres and users after the initial centre identification process and the estimated prevalence that was calculated for each country. Prevalence was closely related to a country's median year of starting HMV (see below).
Estimated number of centres, home mechanical ventilation users and prevalence#
Survey response rate
A total of 329 centres completed and returned the full survey. Table 1⇑ shows the actual number of centres and HMV users on which data was collected for each country and national response rates. Of the originally identified centres, 62% completed full surveys. For some countries, the actual number of centres was greater than that estimated since during the process of survey distribution and collection, further centres were identified. France's estimated number of centres was an approximation of the number of Associations plus known large prescribing centres.
Overall, the surveys provided data on 21,526 HMV users, giving a response rate of 79% by user numbers. Some of these users may be described twice by, for example, French Associations and Hospital units. A total of 2,787 users were included in the Associations' surveys. Outside France, a further 2,230 users were described as having “shared care” with another unit. Taking these two situations into account, the absolute minimum number of individual users described in the surveys is 16,509 (61% of the estimated number). There was a close relationship between the estimated and actual number of both centres and users (r = 0.828, p<0.001 for centres; r = 0.932, p<0.001 for users).
Institution characteristics
Institution type
Excluding French Associations, 40% of the surveys were completed by university hospitals, 50% by non-university hospitals and 10% by a mixture of private institutions, outpatient or rehabilitation centres. Figure 1⇓ shows the variation in the type of institution between countries. Overall, university hospitals had more users (university: 40.5 (13.5–87.5); non-university 14.5 (6.5–38); p<0.001), had started their service earlier (year of starting: university: 1991 (1987–1996); non-university 1994 (1990–1998); p = 0.002), were more likely to be referral centres (p<0.001, Chi-squared test) and had initiated more users themselves (percentage initiated: university: 97.5 (91–100); non-university 93 (80–100); p = 0.025).

Percentage of each institution by country. ▪: university hospital;  : non-university hospital; □: private institution; ▪: other; └: French Association.
: non-university hospital; □: private institution; ▪: other; └: French Association.
Year of starting HMV and centre size
The median year of starting HMV by country (fig. 2⇓) was related to the country prevalences, with countries starting earlier having a greater prevalence (r = −0.611; p = 0.02). The year of starting also determined the country's median centre size (as measured by user numbers; fig. 3⇓) with larger centres seen in countries starting earlier (r = −0.602; p = 0.014).

Median (interquartile range) year of starting home mechanical ventilation (HMV) for each country. Denmark shows the median and full range as only two centres were included.

Median (interquartile range) centre size for each country measured by number of home ventilation users. Denmark shows median only (range 250–253 for its two centres).
User characteristics
Disease categories and demographics
There were large differences between countries in the relative percentages of users in the three disease categories (fig. 4⇓). There was a close relationship between lung and thoracic users and age >66 yrs (Lung: r = 0.447, p<0.001; Thor: r = 0.265, p<0.001) with a reciprocal positive relationship between younger age (0–65 yrs) and neurological users (age 0–16 r = 0.324, p<0.001; age 17–25 r = 0.382, p<0.001; age 26–65 r = 0.179, p = 0.003). Lung users were more often male (r = 0.163; p = 0.006) and thoracic users more often female (r = 0.132; p = 0.027).

Percentage of users in each disease category by country (see Methods section for an explanation of disease categories). ▪: lung/airways;  : thoracic cage; □: neuromuscular.
: thoracic cage; □: neuromuscular.
University centres had a higher proportion of neurological users and non-university hospitals more lung users (percentage: Neur: university 36.4 (17.5–70); non-university 19.9 (6.7–58.3); p<0.001. Lung: university 20 (3.2–39.9); non-university 37.5 (9.9–70.6); p = 0.001). Non-university hospitals had more elderly users (percentage >66 yrs: university 33.3 (18.2–50); non-university 40 (16.7–58.3); p = 0.036). Centres starting their service earlier had more neurological and less lung users (year of starting related to: Neur: r = −0.324, p<0.001; Lung: r = 0.261, p<0.001).
Years on HMV
Figure 5⇓ shows the variation in the number of years each country's HMV users had been on ventilation. This was related to a country's median year of starting HMV; those countries starting earlier had more users on ventilation for ≥10 yrs (r = −0.847; p<0.001) and fewer for <1 yr (r = 0.55; p = 0.03). This was true for all the centres. In addition, larger centres had less users starting in the previous year (r = −0.198; p = <0.001) and more users on for 6–10 yrs (r = 0.457; p<0.001).

Duration of ventilation (number of yrs) by country. ▪: <1 yr;  : 1–5 yrs; □: 6–10 yrs; ▪: ≥11 yrs.
: 1–5 yrs; □: 6–10 yrs; ▪: ≥11 yrs.
Disease categories and years on HMV
Overall, neurological users were most likely to have been on ventilators for >6 yrs (6–10 yrs: r = 0.246, p<0.001; >10 yrs: r = 0.273, p<0.001). Lung users had an opposite pattern, with more ventilated for <1 yr (r = 0.322; p<0.001). Thoracic users were associated with a length of time on HMV of 6–10 yrs (r = 0.155; p = 0.01).
Equipment
Ventilator type
Almost all of the HMV users had positive pressure ventilators, with only 0.005% (79 users) having other types. Volume preset positive pressure ventilators were used the least for lung problems and most frequently for neurological problems (% volume: Lung 15%; Thor 28%; Neur 41%). Figure 6⇓ shows the relative proportion of volume and pressure preset ventilators used by each country. Non-university hospitals used more volume preset ventilators for their neuromuscular users than university hospitals (% volume: non-university 50 (0–88); university 25 (0–67); p = 0.04). Longer established centres used less pressure in all the disease categories (Lung: r = 0.341, p<0.001; Thor: r = 0.329, p<0.001; Neur: r = 0.203, p = 0.002).

Percentage of pressure and volume preset positive pressure ventilators used by all home mechanical ventilation users by country. ▪: pressure preset;  : volume preset.
: volume preset.
Interface type
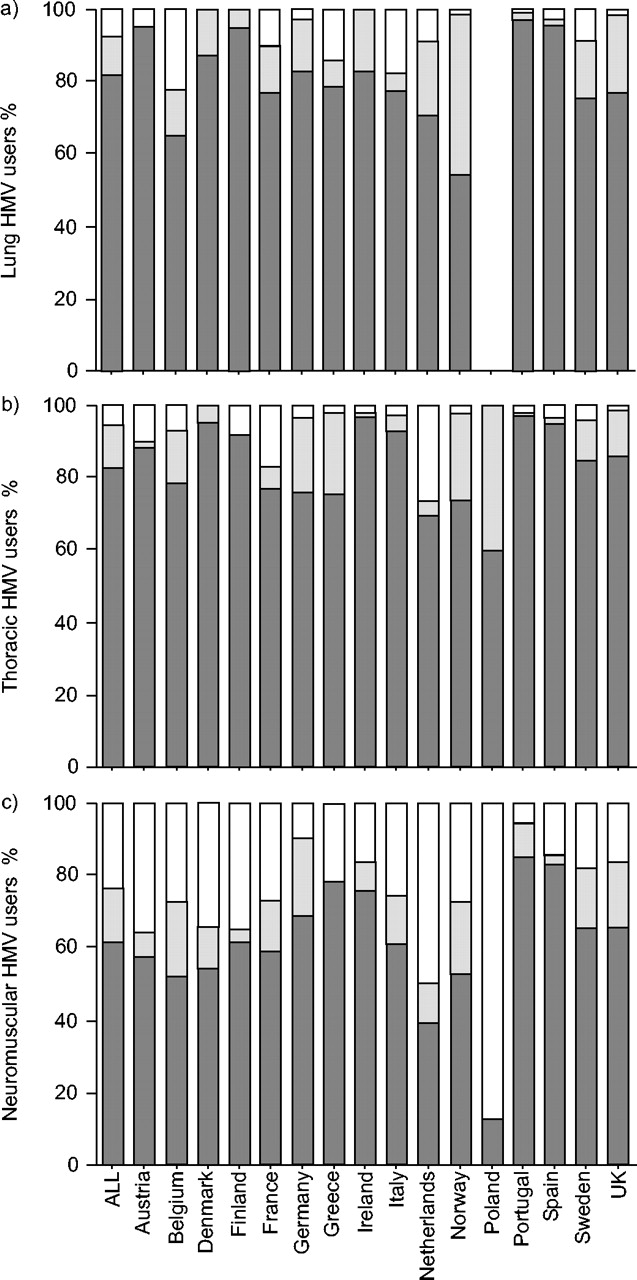
Overall, 13% of the survey population had ventilation via a tracheostomy with the highest percentage in neuromuscular patients (Neur 24%; Thor 5%; Lung 8%). Figure 7⇓ shows the variation in the use of different interfaces for the three disease categories between countries. Smaller centres had a higher percentage of neuromuscular users with tracheostomies (r = −0.187; p = 0.004). Centres starting their HMV service earlier used more tracheostomies for both thoracic and neuromuscular users (Thor: r = −0.346, p<0.001; Neur: r = −0.150, p = 0.02).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Percentage of nasal and facial masks and tracheostomies for each disease category by country for a) lung, b) thoracic and c) neuromuscular home mechanical ventilation (HMV) users. ▪: nasal mask;  : facial mask; □: tracheostomy. No data was available for Polish lung users.
: facial mask; □: tracheostomy. No data was available for Polish lung users.
DISCUSSION
The present study is the initial report of a major survey into the custom and practices in relation to HMV in 16 European countries. It presents information on centre characteristics, user demographics and equipment choices for 329 centres with up to 21,526 users.
A postal survey requesting detailed information on practices is never completely accurate. The initial challenge was to identify all centres with HMV users. Apart from a few countries with registers of centres, extensive research was involved and an initial questionnaire was sent to all possible centres. Although the response rate to this was not 100%, all National Representatives completed the first stage thoroughly and were confident that their estimate of the number of centres and users was as accurate as possible at the time. Therefore, the estimated comparative prevalence has some validity, although conclusions should be seen in the context of the method used by each country.
The estimated prevalence of HMV in Europe was 6.6 per 100,000 people with the highest prevalences in France, Denmark, Sweden, Portugal, Norway and Finland. There was a close relationship between the median year each country started HMV services and their estimated prevalence. This effectively explains the lower prevalences for Poland and Greece, as well as the higher prevalences in Scandinavia and France. However, this cannot be the only explanation for the variability. France, Denmark and Sweden have detailed observatories 3 or registers 4 of their associations/centres and user numbers; they also started their service at similar times. Nonetheless, there remains a marked variation in prevalence, with France's 70% higher than the other two countries. The true prevalence of HMV in Europe can only be measured from accurate and up-to-date national and international registers of users, and is likely to be higher than the estimate from this survey.
The overall response rate to the main survey was good, with returns from 62% of identified centres. The responding centres represented up to 79% of the estimated number of users. The centres failing to return the surveys were more likely to be smaller, as demonstrated by most countries' higher response rate by user rather than centre numbers. For example, the 26% of Swedish responding centres represented 83% of the well-documented HMV user population of that country 5. The close correlation between the estimated and surveyed number of centres and users suggests that there were no large discrepancies. Therefore, the data presented on centre characteristics, user demographics and equipment choices are likely to be a realistic representation of the situation in each country and Europe as a whole.
The variation between countries in the proportion of lung and neuromuscular patients ventilated is conspicuous. The lung users in this survey were more likely to be male and aged >65 yrs. The majority, therefore, are likely to represent COPD patients. The survey showed that 34% of HMV users (>7,000 people) had lung diseases, and 38% were aged >66 yrs. Therefore, despite conflicting evidence of a long-term benefit for ventilation in COPD patients 7–10, the current authors have found that it is being used on a wide scale. Previous reports have indicated an increasing rate of ventilation for COPD patients in France 11 and Switzerland 12. However, high levels of variation in the relative percentage of lung users demonstrate that this is not true for all countries.
This may help explain the variable estimated prevalences of HMV between similar countries. For example, France's excess compared with Denmark and Sweden may be a reflection of the greater interest in the ventilation of COPD patients in some French centres. In contrast, there are still large differences in prevalences among other countries with similar proportions of lung patients. Germany has a prevalence that is 40% higher than Italy; Portugal's is more than double that of Austria. Among those countries with a greater proportion of neuromuscular users, after considering the year of starting, variations remain evident. Denmark's prevalence is 40% higher than the Netherlands; Finland is similarly ahead of Belgium. Thus, there are clearly many factors contributing to the variation in estimated prevalences, but it is likely that at least some of the explanation lies in different national attitudes to the potential value of long-term ventilation in both lung and neuromuscular conditions. The system of reimbursement may be an explanation in some countries with national policies, dictating which users are ventilated. For example, Belgium has strict criteria for agreeing to reimbursement for ventilated COPD patients.
Many studies have shown equivalent effects of pressure and volume preset ventilators on blood gases 13, ventilatory pattern 14, and nocturnal oxygen saturation 15. Although there is evidence to suggest that volume preset ventilators offer an advantage in patients with the most severe respiratory failure 16, this may not be borne out in routine clinical practice. In general, older centres used more volume preset ventilation; they also had patients on HMV for a greater number of years. Therefore, these users may represent a cohort with more severe respiratory failure. The older centres may also have used volume preset ventilators in the past as they were more commonly available in the 1980s and early 1990s and have not switched their longer term users to newer machines. The variation between countries in their choice of ventilator type is also likely to be a reflection of national ventilator company activity and other logistical or reimbursement policies.
The use of tracheostomy varied considerably between countries. Only France, Greece, Italy and Belgium had a significant percentage of lung users with tracheostomies. France has the most experience of this technique in COPD, with variable results from published trials comparing ventilation via a tracheostomy with oxygen therapy alone 17–18. In countries with comparatively more neuromuscular users, variations were also apparent in the relative use of tracheostomy for these patients. A total of 50% of Dutch neuromuscular patients had a tracheostomy, compared with 35% in Denmark and only 18% in Sweden. The evidence for improved outcome with tracheostomy in progressive neuromuscular conditions is limited 19–20 and the conflicting patterns most likely reflect local and national practices, including the availability of carers and other resources.
The survey showed that lung users had been on ventilation for the shortest time and neuromuscular users the longest. This supports previous evidence, measured by the probability of continuing ventilation, indicating a relatively worse prognosis for lung users on long-term ventilation 1–2. In contrast, it could also reflect a more recent escalation in the use of long-term ventilation in COPD patients. The fact that neuromuscular and thoracic users continue their ventilation for ≥6 yrs supports previous findings that neuromuscular and thoracic patients can be maintained on ventilation for many years 2.
In conclusion, the present well-supported survey has provided reliable estimates of the prevalence of home mechanical ventilation in Europe and has revealed a large variation in the 16 countries involved. It has also shown different patterns of home mechanical ventilation use, especially in its application in older patients with chronic obstructive pulmonary disease and the use of tracheostomies in neuromuscular users. It should facilitate national and European planning for home mechanical ventilation in the future, particularly with the recent expansion of the European Union. Europe-wide registers of centres/users, guidelines and further epidemiological research would aid the development of home mechanical ventilation services and ensure equality of provision and access.
Acknowledgments
The contributors to the Concerted Action included five partners, other members of the Steering Committee and 16 National Representatives. The partners were N. Ambrosino (Italy), J. Escarabill (Spain), R. Farre (Spain), D. Robert (France) and J.A. Wedzicha (UK). Together with the five partners, the Steering Committee included G.C. Donaldson (UK), B. Fauroux (France), S.J. Lloyd-Owen (UK), B. Schoenhofer (Germany) and A.K. Simonds (UK). The National Representatives for each country were T. Wanke (Austria), D. Rodenstein (Belgium), O. Nørregaard (Denmark), R. Pirtimaa-Kaitanen (Finland), J-F. Muir (France; with A. Cuvelier), G. Laier-Groeneveld (Germany), N. Siafakas (Greece; with M. Klimathianaki), W. McNicholas (Ireland; with L. Doherty), A. Vianello (Italy), M. Kampelmacher (The Netherlands), S.O. Mollestad (Norway), J. Zielinski (Poland), J.C. Winck (Portugal), F. Masa (Spain), B. Midgren (Sweden) and M. Elliott (UK). In addition, the authors would like to thank all the centres who took part in the survey and acknowledge the organisational support provided by N. Roberts and database design advice provided by K. St Louis.
- Received June 7, 2004.
- Accepted March 15, 2005.
- © ERS Journals Ltd
References









