





Abstract
Resistive breathing is an “immune challenge” for the body, initiating an inflammatory response consisting of an elevation of plasma cytokines, and the recruitment and activation of lymphocyte subpopulations. These cytokines do not originate from monocytes, but are, instead, produced within the diaphragm, secondary to the increased muscle activation.
Oxidative stress is a major stimulus for the cytokine induction, secondary to resistive breathing. The production of cytokines within the diaphragm may be mediating the diaphragm muscle fibre injury that occurs with strenuous contractions, or contributing towards the expected repair process. These cytokines may also compromise diaphragmatic contractility or contribute towards the development of muscle cachexia. They may also have systemic effects, mobilising glucose from the liver and free fatty acid from the adipose tissue to the strenuously working respiratory muscles. At the same time, they stimulate the hypothalamic-pituitary-adrenal axis, leading to production of adrenocorticotropin and β-endorphins.
The adrenocorticotropin response may represent an attempt of the organism to reduce the injury occurring in the respiratory muscles via the production of glucocorticoids and the induction of the acute phase-response proteins. The β-endorphin response would decrease the activation of the respiratory muscles and change the pattern of breathing, which becomes more rapid and shallow, possibly in an attempt to reduce and/or prevent further injury to the respiratory muscles.
- Control of breathing
- exercise immunology
- interleukin-6
- oxidants/antioxidants
- respiratory immunology
- respiratory muscle
Resistive breathing is encountered in many disease states, such as asthma and chronic obstructive pulmonary disease (COPD). Asthma and COPD are associated with significant airway inflammation, with elaboration of various cytokines within the airways. When strenuous enough, inspiratory resistive breathing produces diaphragmatic fatigue 1 and diaphragmatic structural injury 2, 3. In this report, the current authors review recent evidence that resistive breathing per se is an “immune challenge” initiating an inflammatory response in the body. Potential implications that this immune response might have for respiratory failure are also discussed.
The immune response to inspiratory resistive breathing
Strenuous whole-body physical exercise, in the form of long-distance running, treadmill and cycle ergometry, has been shown to increase the level of circulating cytokines. Thus, increased plasma levels of tumour necrosis factor (TNF)-α, interleukin (IL)-1β, IL-1 receptor antagonist, TNF receptors, IL-10, IL-8, and macrophage inflammatory protein-1 are found after strenuous exercise 4.
Inspiratory resistive breathing represents a form of “exercise” for the respiratory muscles. Accordingly, when healthy normal volunteers were subjected to resistive breathing (45 min at 75% of their maximum inspiratory pressure through alinear inspiratory resistance with unloaded expiration), the plasma levels of IL-1β and IL-6 and TNF-α were significantly elevated (figs 1⇓ and 2⇓) 5, 6.
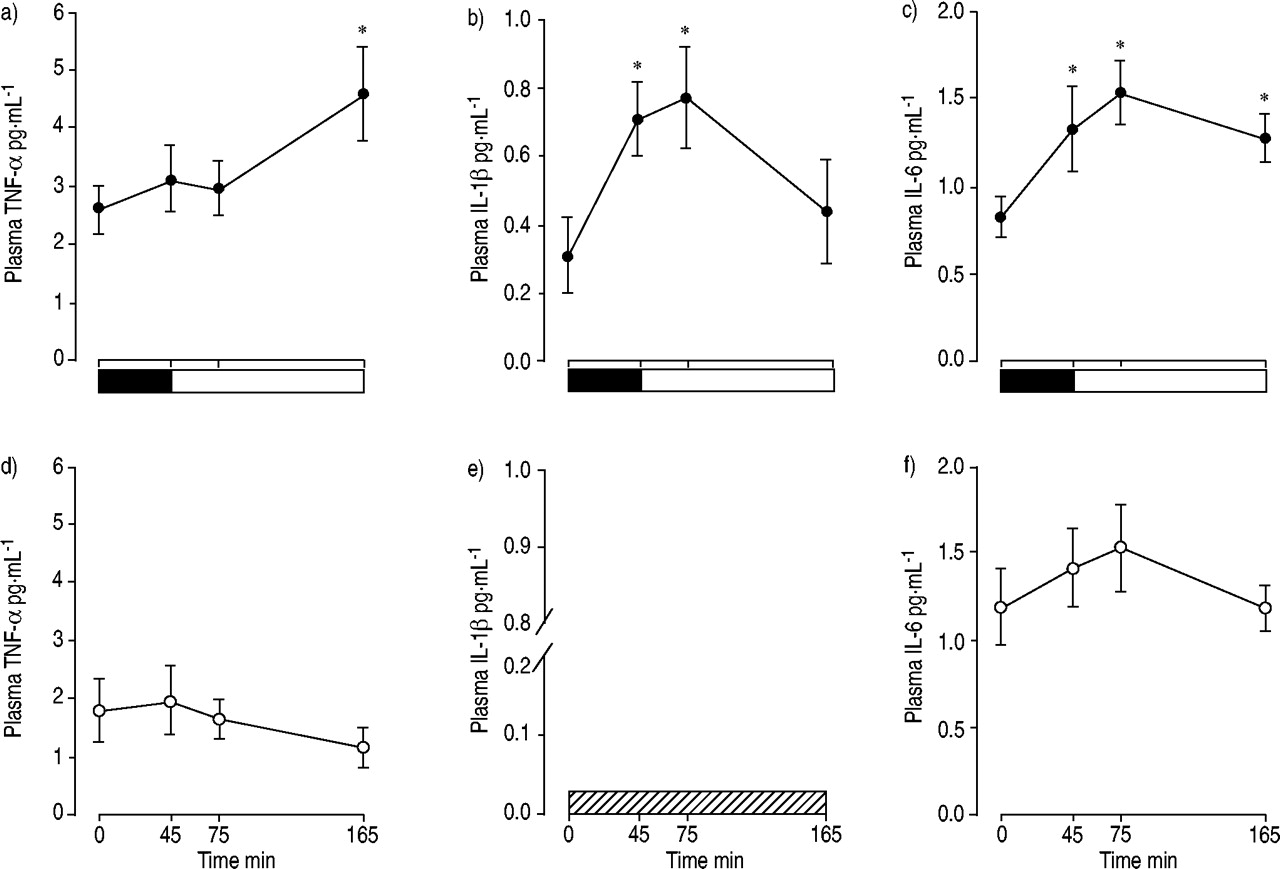
The plasma cytokine response to resistive breathing before (•; a, b and c) and after (○; d, e and f) antioxidants. The mean plasma tumour necrosis factor (TNF)-α (a and d), interleukin (IL)-1β (b and e), and IL-6 concentrations (c and f) before the resistive breathing session (0 min), at the end of resistive breathing (▪: load; 45 min), and 30 and 120 min after the end of resistive breathing (□: recovery; i.e. 75 min and 165 min after the beginning of the resistive breathing session) were recorded. The plasma IL-1β was below detection limit after antioxidant supplementation (└; e). *: p<0.05 compared with baseline values (0 min). Modified from 6 with permission.
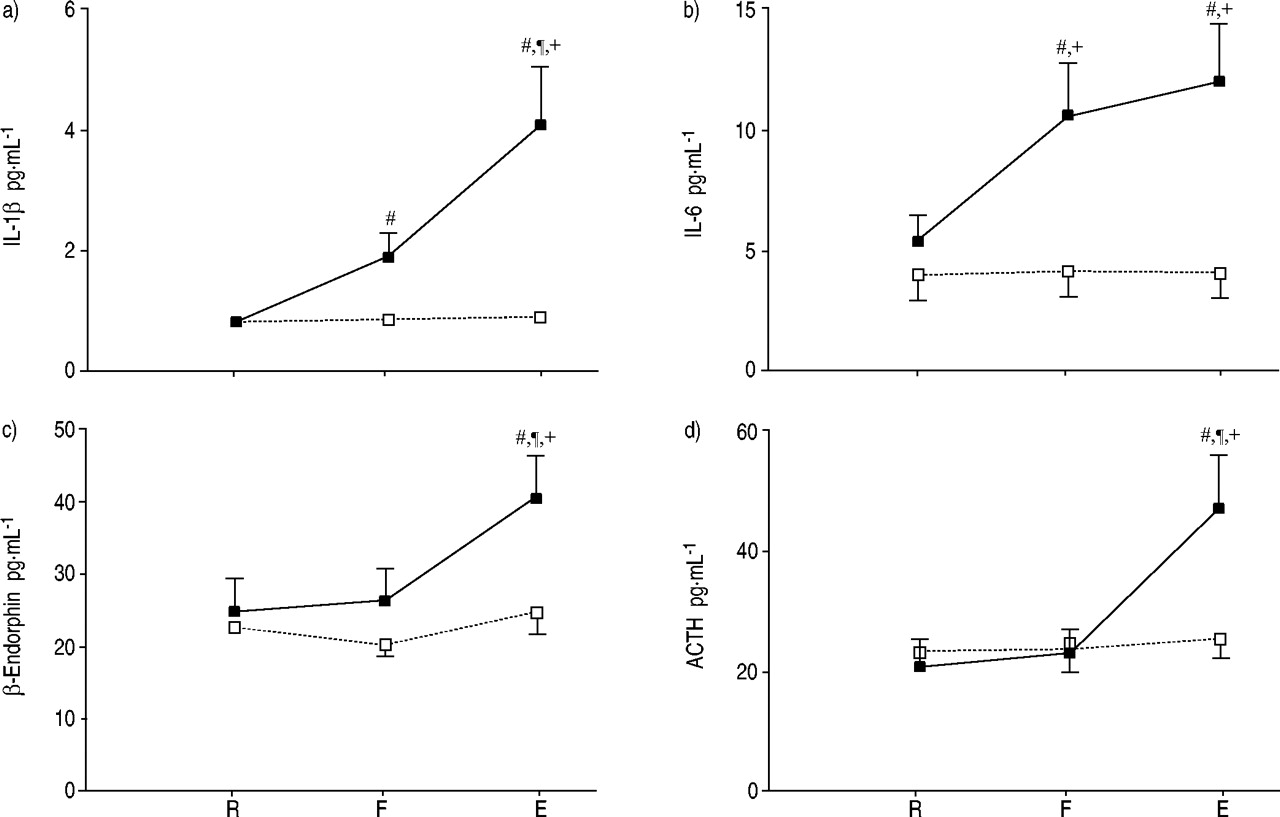
The plasma cytokine and hypothalamic pituitary responses to resistive breathing. Mean plasma level of interleukin (IL)-1β (a), IL-6 (b), β-endorphin (c) and adrenocorticotropin hormone (ACTH; d) at rest (R), at the point where the subjects could not generate the target maximum inspiratory pressure (75% of maximum, 45 min after the beginning of resistive breathing; F), and at the end of resistive breathing (15 min later, at 60 min from the beginning; E). From F to E, subjects were put through an alinear resistance to the maximum they could achieve. Data are presented as mean±sem. ▪: high-load run; □: moderate-load run. #: statistically significant difference (p<0.05) from R; ¶: statistically significant difference (p<0.05) from F; +: statistically significant difference (p<0.01) from the moderate-load run. Modified from 5 with permission.
Not only were plasma cytokines elevated, but preliminary data suggest that specific lymphocyte subpopulations were also recruited and activated. Accordingly, flow cytometric analysis of blood derived from these subjects, with incubation of lymphocytes with monoclonal antibodies against cell surface antigens characterising their subpopulation and activation state, showed that the immunofluorescence of positive cells for CD3−/CD16/56+, CD3/CD8 and CD8/CD45RA was increased after the resistive breathing session, which means that strenuous resistive breathing increases the percentage of T-cytotoxic lymphocytes, T-cytotoxic naïve lymphocytes and natural killer cells 7.
Thus, strenuous resistive breathing induces an immune response consisting of the elevation of plasma cytokines, and the recruitment and activation of lymphocyte subpopulations.
The origin of resistive breathing-induced plasma cytokines
The source of the resistive breathing-induced cytokines was not known. Blood monocytes are a major, though not an exclusive, source of immuno-inflammatory mediators 8. When activated by various stimuli, they release a cascade of cytokines, including TNF-α, IL-1β and IL-6 8. Thus, it was hypothesised that activated blood monocytes are a likely source of cytokine production during strenuous resistive breathing, given that intense exercise induces (apart from cytokines) endotoxaemia 9, and leukocyte mobilisation and activation 10. Six healthy subjects performed resistive breathing sessions at 75% of maximum inspiratory pressure. Monocytes were isolated from blood, and were made permeable (with saponin treatment) and incubated with fluorescent monoclonal antibodies against TNF-α, IL-1β and IL-6 6. Intracellular flow cytometric detection of cytokines was used, which allows for the sensitive determination of cytokine production by specific cell types, since it measures the amount of protein arrested at the Golgi complex of a specific cell population at a specific time point 11. Neither the percentage, nor the absolute number of cytokine-positive monocytes increased in response to resistive breathing 6. The mean fluorescence intensity, a rough estimate of the amount of cytokine production by cytokine-positive cells 11, was also not altered by resistive breathing. Furthermore, no correlation was found between the level of cytokine expression in monocytes and the plasma level of cytokines. Thus, although a role for monocytes in the baseline plasma level of cytokines cannot be excluded, monocytes do not contribute to the resistive breathing-induced plasma cytokine elevation.
Studies using various techniques have established that skeletal muscles exhibit a low level of constitutive expression of various cytokines, such as TNF-α 12, IL-1β 13, and IL-6 14. Since strenuous muscular contractions increase IL-6 production within skeletal muscles 14, it was hypothesised that cytokines are induced in the diaphragm in response to acute resistive loading 15. Anaesthetised, tracheostomised, spontaneously breathing adult Sprague-Dawely rats were subjected for 1, 3 or 6 h to inspiratory resistive loading, corresponding to 45–50% of the maximum inspiratory pressure. Rats that were subjected to the same procedures and allowed to breathe spontaneously for equal time periods with no load served as controls. The diaphragm and the gastrocnemius muscles were excised at the end of the loading period, and mRNA expression of 11 cytokines and two housekeeping genes (L32, glyceraldehyde-3-phosphate dehydrogenase) was analysed in these muscles using a multi-probe ribonuclease protection assay system (RiboQuant; Pharmingen, San Diego, CA, USA). IL-6, and to a lesser extent IL-1β, TNF-α, IL-4, IL-10 and interferon (IFN)-γ, were significantly increased in a time-dependent manner in the diaphragm of animals subjected to inspiratory resistive loading. No changes in cytokine expression were observed in the diaphragms of control animals or in the gastrocnemius muscle 15.
Thus, cytokines are constitutively expressed within the respiratory muscles, and are significantly upregulated during strenuous respiratory muscle contraction induced by inspiratory resistive loading. In fact, previous studies provide indirect evidence that cytokines are upregulated in the diaphragm, secondary to exercise 16. When rats were subjected to an acute bout of exercise (90 min treadmill running) and their diaphragms were excised and homogenised at the end of the exercise session, the diaphragmatic homogenate could increase the in vitro proliferation of thymocytes, which suggested that increased cytokine bioactivity was present in the diaphragmatic homogenates, since cytokines are strong proliferative stimuli for thymocytes 16.
The upregulation of cytokine expression within the diaphragm, secondary to the resistive loading, observed represents relatively abundant mRNA tissue levels, since cytokines were detected using a multi-probe ribonuclease protection assay 15, which does not amplify the RNA signal and is less sensitive than the commonly used technique to detect RNA, the RT-PCR (requiring 104–105 larger quantities for RNA to be present in the tissues for positive signal detection 17). The mRNA upregulation was accompanied by commensurate increases in the cytokine protein levels, at least for the IL-6 and IL-1β. Furthermore, immunohistochemistry revealed that myocytes are the IL-6-producing cells in the diaphragm.
It has to be acknowledged that the intradiaphragmatic cytokine production does not prove that these cytokines are released in the circulation and can account for the plasma cytokine elevation, secondary to resistive breathing. However, results from leg extension exercise studies, where the arteriovenous IL-6 difference across the contracting femoris muscle was determined, suggest that this is very likely, since the IL-6 production from the quadriceps femoris muscle could account for the systemic IL-6 elevation 18.
It can also be speculated that the increased transpulmonary pressure gradient during resistive breathing causes cytokine induction from cells that are resident in the lung, such as epithelial cells and fibroblasts, secondary to the augmented extraluminal stress imposed, which could contribute to the plasma cytokine elevation. This possibility is supported by studies of isolated, perfused mouse-lung preparations, where increased transpulmonary pressure led to IL-6 and TNF-α release 19. It should be emphasised, however, that these results were obtained by profound overdistention of the lung, which is unlikely during resistive breathing, at least in normal humans and animals.
Consequently, the diaphragm is the only proven source of cytokine induction during resistive breathing. More studies are, of course, needed to elucidate other potential tissues/cells of cytokine origin, secondary to resistive loading.
It has to be acknowledged that the immune response described secondary to resistive breathing was observed in healthy humans and animals, and, thus, extrapolation of these results to disease states or other forms of loaded breathing (e.g. elastic loading) should be done with great caution. The level of loading was relatively high (45–75% of maximum inspiratory pressure), which is usually observed during acute exacerbations of asthma or COPD leading to acute respiratory failure 20. However, data from peripheral skeletal muscle exercise and the rat model of resistive breathing that the current authors used suggest that lower levels of resistive loading, if prolonged, would also lead to an immune response in a time-dependent fashion. Furthermore, when a skeletal muscle is “primed” by a bout of exercise, subsequent bouts of exercise (of equal duration and load) exhibit an augmented cytokine response 21. Such a pattern would be typical of an asthmatic patient with waxing and waning airway narrowing. The underlying condition of the muscles and the adaptations observed secondary to disease states (e.g. COPD) might also influence the immune response to exercise. Although there is a paucity of existing data, the immune response to exercise is rather augmented in COPD patients 22: only 11 min of cycling (at 40% of peak work rate) increased plasma TNF-α levels in COPD patients, but not in healthy controls. Obviously, more studies are needed to elucidate the immune response to resistive and other forms of loaded breathing in various disease states.
The stimuli for the resistive breathing-induced plasma cytokines
The stimulus for the upregulation of cytokine induction in response to resistive breathing is not known. Resistive breathing increases the production of reactive oxygen species (ROS), both within the working respiratory muscles and in the extracellular and vascular compartments 23. ROS are able to induce cytokine production from various cell types. To test the hypothesis that oxidative stress is a stimulus for the cytokine induction secondary to resistive breathing, six healthy subjects performed two resistive breathing sessions before and after receiving a combination of antioxidants (vitamins E 200 mg·day−1, A 50,000 IU·day−1 and C 1,000 mg·day−1 for 60 days, allopurinol 600 mg·day−1 for 15 days and N-acetylcysteine 2 g·day−1 for 3 days before the second session) 6. Before antioxidants, plasma cytokine levels (determined by ELISA) increased secondary to resistive breathing (TNF-α and IL-6 by twofold, IL-1β by threefold). After antioxidants, plasma IL-1β became undetectable, the TNF-α response to resistive breathing was abolished, and the IL-6 response was significantly blunted (fig. 1⇑) 6.
Since the diaphragmatic myocytes are the source of the resistive breathing-induced cytokines, the ability of ROS to stimulate the production of IL-6 from skeletal myocytes was tested in vitro 24. Differentiated C2C12 murine skeletal muscle cells (myotubes) exposed to ROS-producing agents (pyrogallol, xanthine/xanthine oxidase or H2O2) for 24 h exhibited a concentration-dependent increase in IL-6 production. In addition, pre-treatment of cells with the ROS scavenger N-acetylcysteine blocked the TNF-α-induced IL-6 release, suggesting a crucial role for endogenously produced ROS in IL-6 production, since TNF-α treatment leads to intracellular oxidative stress. Treatment of myocytes with ROS-generating agents increased nuclear factor (NF)-κB-dependent promoter activity. Finally, pre-incubation of myotubes with the pharmacological inhibitor of NF-κB, diethyldithiocarbamate or transient transfection with a dominant negative NF-κB construct inhibited the ROS-stimulated IL-6 release. These in vitro results showed that ROS stimulate IL-6 production from skeletal muscle cells in a manner that involves transcriptional activation of the IL-6 gene via a NF-κB-dependent pathway 24.
The antioxidant supplementation blunted, but did not completely abolish the IL-6 response to resistive breathing. This suggests that the stimuli for the IL-6 production during resistive breathing might be multiple. Although these stimuli during resistive breathing have not been studied, results from whole-body exercise studies suggest that carbohydrates attenuate the IL-6 response to exercise and glycogen depletion greatly augments it 25. Interestingly, significant glycogen depletion has been documented in the diaphragm secondary to resistive breathing 26. Furthermore, adrenergic stimulation could also have a contributing role 25.
The stimuli for the induction of cytokines other than IL-6 during exercise are less well studied. Pre-treatment with antioxidants abolished the resistive breathing-induced elevation of TNF-α, whereas IL-1β became undetectable (fig. 1⇑) 6, which suggests that oxidative stress is a strong stimulus for the resistive breathing-induced IL-1β and TNF-α response.
Thus, it is possible that the plasma cytokine induction during resistive breathing is differentially regulated by various stimuli, some of them being common (e.g. ROS), whose relative importance varies with each respective cytokine. Further studies are needed to elucidate other potential stimuli for the resistive breathing-induced cytokine upregulation.
Implications for respiratory failure
Resistive breathing-induced cytokine upregulation may serve several local and systemic functions, which could be both adaptive and maladaptive.
Local effects
Muscle injury
Strenuous resistive breathing results in diaphragmatic injury in both animals and humans 2, 3, 27. The mechanisms involved are not definitely established, though increased activity of the proteolytic enzymes' calpains 2 and ROS 27 are involved. It is tempting to speculate that intradiaphragmatic cytokine induction could be involved in mediating the injurious process 15. In fact, cytokines, such as IL-1β, can upregulate the expression of adhesion molecules on the surface of endothelial cells and enhance transendothelial migration of blood-derived inflammatory cells 28. Initially, this would recruit neutrophils and, later, monocytes within the muscle, which might mediate the injury. This response is similar to the eccentric exercise-induced intramuscular IL-1 expression and neutrophilic infiltration associated with limb muscle damage in humans 29. Furthermore, cytokines, such as TNF-α, could augment oxidative stress in a paracrine fashion 30, which could contribute to muscle injury 27. In fact, increased oxidative stress was documented in the diaphragm even 3 days after resistive loading 27, which cannot be attributed to increased muscle activation at that time point (3 days after activity). Cytokines and cytokine receptors are upregulated in the muscles in various forms of muscle injury 31, and in muscle diseases, such as critical illness polyneuropathy and myopathy 32. However, the cytokine response is not only maladaptive. In fact, not only pro-inflammatory cytokines, such as IL-1β, TNF-α and IFN-γ, were induced, but anti-inflammatory cytokines, such as IL-4, IL-10 and IL-6 (which has some pro- but mainly anti-inflammatory properties 33), were also upregulated 15, suggesting that some of these cytokines might serve to control local inflammation 33.
Muscle regeneration
Cytokines are also essential in orchestrating muscle recovery after injury. Cytokines, such as TNF-α, IL-6, leukaemia inhibitory factor and IL-1β 31, 34–36, and their cognate receptors 37 are upregulated in skeletal muscle after injury. These cytokines enhance proteolytic removal of damaged proteins 38, 39 and cells (via recruitment and activation of phagocytes). TNF-α also activates satellite cells to enter the cell cycle from the normally quiescent state and enhances their proliferation once it has been initiated 40. Satellite cells are quiescent cells of embryonic origin that reside in the muscle and are transformed into myocytes either during the normal muscle remodelling or when the muscle becomes injured to replace damaged myocytes 41.
Muscle contractility
Cytokines might affect contractility of the diaphragm. TNF-α impairs the in vitro contractility of diaphragm strips from hamsters 42, mice (fig. 3a⇓) 43, or intact diaphragmatic muscle fibres from mice (fig. 3b⇓) 43. Diaphragm strips from mice exhibiting cardiac over-expression of TNF-α with resultant high circulating TNF-α levels show contractile dysfunction of the diaphragm 44, and i.v. TNF-α administration depressed the in vivo contractility of the diaphragms of dogs 45. The mechanism by which TNF-α depresses diaphragmatic contractility is not definitely established. However, the effect is at the level of the myofibrils (actin and myosin) (fig. 3c⇓ and d), since the calcium release and re-uptake is not affected (fig. 3e⇓ and f) 43. The intradiaphragmatic expression of cytokines and, especially, TNF-α with the attendant contractility-depressing effect might contribute to the development of peripheral muscle fatigue (i.e. decreased force production upon constant electrical stimulation of the muscle) observed after resistive loading 1. The intradiaphragmatic expression of cytokines and, especially, TNF-α might also explain the observation that force decline after resistive loading is proportionally greater than the observed muscle injury 46. Whereas force declines by as much as 30%, the degree of injury is only 9%, which suggests that other factors, in addition to injury, are depressing the contractility of the diaphragm 46.

Effect of tumour necrosis factor (TNF)-α on diaphragmatic contractility. a) TNF-α depresses diaphragm force. Diaphragm fibre bundles treated with TNF-α 500 ng·mL−1 (○) developed lower forces than paired controls (•) at all stimulus frequencies (p<0.001). Data are presented as mean±sem. P0: maximal tetanic force. n=8 per group. b) TNF-α stimulates loss of force in single fibres. Values depict mean rates of force decline (%·h−1) measured by regression analysis using data from individual experimental fibres (n=5) before and after exposure to TNF-α 500 ng·mL−1. TNF-α accelerated the loss of force in each of five fibres studied (p<0.02). c, d) Depression of tetanic force transients by TNF-α. Individual tracings obtained from intact single fibres stimulated at 80 Hz before (––––) and after (……) 4-h incubation in either buffer alone (control fibre; c) or in TNF-α 500 ng·mL−1 (experimental fibre; d). e, f) Insensitivity of tetanic intracellular calcium ion concentration ([Ca2+]i) transients to TNF-α. Individual tracings obtained from intact single fibres stimulated at 80 Hz before (––––) and after (•;) 4-h incubation in either buffer alone (control fibre; e) or in TNF-α 500 ng·mL−1 (experimental fibre; f). Modified from 43 with permission.
Systemic effects
Cytokines produced within the diaphragm secondary to resistive breathing may spill into the circulation, thus explaining the cytokinemia observed after resistive loading in normal humans 5, 6. Interestingly, in diseases of increased diaphragmatic loading, such as COPD, increased plasma cytokine levels have been documented 47–50. Although, initially, these cytokines had been attributed to the bronchial inflammation that accompanies COPD, recent data have shown different regulation of the cytokine response in induced sputum and plasma 47, which suggests that plasma cytokinemia in COPD is not due to an overflow of inflammatory mediators from the local lung compartment. It is tempting to speculate that cytokines produced within the diaphragm, secondary to the increased load, enter the circulation and could explain the discrepancies between the lung and systemic inflammation. Interestingly, plasma IL-6 was increased during an exacerbation of COPD 51, a condition that further augments the load faced by the respiratory muscles. Furthermore, COPD patients exhibit an augmented plasma TNF-α response to exercise, which cannot be attributed to production of TNF-α by the exercising leg muscles, since no increase was observed in the TNF-α mRNA level in biopsy samples from the vastus lateralis muscles of these patients 22. An interesting, yet speculative explanation could be that TNF-α can originate from the strenuously contracting respiratory muscles of COPD patients during exercise.
Increased plasma IL-6 and TNF-α levels have also been documented in sleep apnoea patients 52–55, which could not be explained by the attendant obesity, since obese individuals with similar body mass indices had significantly lower cytokine values. A potential explanation could be that cytokines are produced by the diaphragm, secondary to the strenuous contractions induced by upper airway obstructions during apnoeas and hypopnoeas. Along these lines, a significant elevation of TNF-α and a smaller (nonstatistically significant) elevation of IL-6 were observed during sleep after the first obstructive apnoea 55. Hypoxaemia that developed during sleep, secondary to the apnoeas-hypopnoeas, might also contribute to the plasma cytokine elevation 55. In fact, the effects of exercise and hypoxaemia are synergistic in elevating plasma IL-6 56. In support of the role of strenuous respiratory muscle contraction and hypoxaemia as the reasons for cytokine elevation in sleep apnoea, nasal continuous positive airway pressure therapy, which prevents the apnoeas-hypopnoeas with the attendant strenuous diaphragmatic contractions and the episodes of hypoxaemia, results in significant decrease of plasma IL-6 levels 54. Furthermore, a deranged ex vivo production of TNF-α is observed in sleep apnoea patients 57, where the nocturnal elevation of the ex vivo production of TNF-α by blood mononuclear cells stimulated in vitro by lipopolysaccharide (endotoxin) is blunted. This pattern is quite similar to what is happening in normal subjects during exercise; while plasma cytokines increase secondary to the exercise, when blood mononuclear cells derived from the same subjects are stimulated in vitro, the ex vivo production of cytokines by these cells is downregulated after exercise 58. In sleep apnoea patients, plasma cytokines increase during the night, while the production of cytokines by blood mononuclear cells stimulated in vitro decreases 57, suggesting that the immune response to sleep apnoea might, in essence, be an immune response to the “exercise” imposed to the respiratory muscles by the repeated episodes of apnoeas-hypopnoeas. Further studies are needed to elucidate these interesting possibilities.
The circulating resistive breathing-induced cytokines may serve several functions, as follows.
Effects on metabolism and endurance
The significantly greater induction of IL-6 within the diaphragm, secondary to resistive breathing, suggests that it might be involved in physiological muscle signalling, and not only to the injury-inflammation repair process 25. Diaphragmatic contraction leads to glycogen depletion 26, which greatly augments IL-6 production from skeletal muscles 14, 59. IL-6 has a hormone-like glucoregulatory role, signalling that glycogen stores are reaching critically low levels in the contracting muscles, and stimulating hepatic glucose output to maintain glucose homeostasis and muscle glucose supply 25. IL-6 also augments lipolysis and fat oxidation 60, which increases the energy that is available to the “exercising” respiratory muscles. IL-6 overproduction might be required for protecting the endurance of the respiratory muscles in conditions of increased respiratory load. Accordingly, double IL-6 knockout mice (IL-6−/−) 61 exhibit reduced endurance to exercise compared with control mice, which suggests that endogenously produced IL-6 is important for maintenance of exercise capacity. IL-6 could serve to attenuate the TNF-α induction, secondary to exercise 62, which decreases diaphragm contractility. Thus, the greater induction of IL-6 within the diaphragm, secondary to resistive breathing, might represent an adaptive response to augment diaphragmatic endurance and contractility in the face of increased load.
Cachexia
Cytokines may contribute to the cachexia observed in some COPD patients 63–65. In fact, a reduced creatinine height index (an indirect measure of skeletal muscle mass) was associated with increased circulating levels of IL-6, TNF-α and their soluble receptors 48. The interested reader could consult recent excellent reviews 63, 64.
Sleep
Diaphragm-derived cytokines may also have central nervous system effects. Both TNF-α and IL-1β affect sleep in healthy and diseased states. The interested reader could consult a recent review 66.
Hypothalamic pituitary adrenal axis stimulation
Cytokines, and especially IL-1β and IL-6, are very strong stimulants of the hypothalamic-pituitary-adrenal (HPA) axis 67–69 (fig. 4⇓), exhibiting significant synergism 70. Both stimulate hypothalamic corticotrophin-releasing hormone secretion from parvicellular neurons located in the paraventricular nuclei, which is the major pro-opiomelanocortin secretagogue by the pituitary corticotroph 67, 70. The pro-opiomelanocortin molecule is then subjected to post-translational modification to produce adrenocorticotropin (ACTH) and β-endorphin, which are concomitantly secreted by the pituitary gland. In fact, cytokines, such as TNF-α, IL-1 or IL-6, exhibit significant synergism in stimulating the release of ACTH 71. IL-6 plays a fundamental role in the stimulation of the HPA axis, but the participation and interaction of IL-1 and TNF-α is also required 70. Interestingly, strenuous inspiratory resistive breathing that induces plasma cytokines stimulates the HPA axis, resulting in increased levels of circulating β-endorphin and ACTH 5 (fig. 2⇑).

Cytokines stimulate the hypothalamic pituitary adrenal axis. a) Changes in plasma concentration of adrenocorticotropin ([ACTH]) in capsaicin-desensitised (└; n=6) and control (□; n=6) groups after i.v. injection of interleukin (IL)-1β (2 µg·kg−1; arrow). *: p<0.05; ***: p<0.001. Modified from 68 with permission. Plasma immunoreactive ACTH (b) and cortisol (c) responses to a s.c. bolus injection of IL-6 (30 µg·kg−1). The grey areas represent the mean±sd responses of healthy normal volunteers to a standard bolus dose (1 µg·kg−1) of corticotrophin-releasing hormone and were included for comparison. Modified from 69 with permission.
There are two alternative, not mutually exclusive explanations for the mechanism of HPA activation, secondary to resistive breathing. First, it may have resulted secondary to the increased levels in circulating proinflammatory cytokines induced by strenuous resistive breathing. This notion is supported by the different time courses of cytokine and hormonal elevations (cytokine elevation appearing first, followed by the increase in β-endorphin and ACTH level; fig. 2⇑). Furthermore, the increase in IL-6 was strongly correlated with the increase in both β-endorphin and ACTH, implying a causative role of IL-6 for the HPA-axis stimulation, secondary to resistive breathing (fig. 4⇑). A second alternative/complementary mechanism accounting for the increased levels of β-endorphin and ACTH is that they may be due to stimulation of small afferent nerve fibres (type III and IV). In fact, it has been suggested that small-diameter phrenic afferent fibres are stimulated by strenuous contraction-induced metabolic changes in the diaphragm, and that these fibres project to various levels of the central nervous system 72. Therefore, it is tempting to speculate that strenuous inspiratory resistive breathing causes β-endorphin and ACTH secretion, secondary to stimulation of small afferent nerve fibres, within the respiratory muscles 68. In fact, this might also be due to the effect of intradiaphragmatically produced cytokines, since cytokines can stimulate small afferent nerve fibres, leading to ACTH elevation 68, 70.
The ACTH response may represent an attempt of the organism to reduce the injury occurring in the respiratory muscles via the production of glucocorticoids by the adrenals, which suppress inflammatory genes, and induction of the acute phase-response proteins from the liver, which serve as antiproteases 67.
Control of breathing
Diaphragm-derived cytokines may also affect the control of breathing. In fact, large exogenous doses of IL-1β 73 and endotoxin, which leads to pro-inflammatory cytokine release 74, stimulate the respiratory controller. However, the effect of endogenously produced cytokines might be different. This could either be a direct effect on the respiratory controller or an indirect effect mediated through the production of β-endorphins, though the two mechanisms might coexist. Accordingly, mice suffering from muscular dystrophy have blunted ventilatory response to hypercapnic challenge (7% CO2) compared with normal mice 75. Concurrent elimination of TNF-α (by deletion of the genes for TNF-α) significantly improved the hypercapnic ventilatory response, which suggests that endogenously produced TNF-α depresses the respiratory controller 75.
The indirect effect is likely to be mediated through the elaboration of β-endorphins that decrease the activation of the respiratory muscles and change the pattern of breathing, which becomes rapid and shallow. This is probably an attempt of the respiratory controller to reduce the strenuous respiratory muscle contractions and, thus, the accompanying muscle injury, through the decline in tidal volume at the expense of increased respiratory frequency 76. Ιn animals, adequate evidence supports this concept 77–80. It was demonstrated that resistive loading resulted in a progressive reduction in tidal volume, which was partially reversed by administration of the opioid antagonist naloxone 76, 79 (fig. 5⇓). An increase in β-endorphin in the cisternal cerebro-spinal fluid was also detected 79.

Endorphins and resistive loading. The tidal volume (VT) response of unanaesthetised goats to 2.5 h of high inspiratory flow-resistive loading prior to and following the administration (open arrow) of naloxone (•) or saline (○). VT, which fell considerably after loading (shallow breathing), increased after naloxone administration, while saline had no effect. These data indicate that inspiratory resistive loading activates the endogenous opioid system, and that the reduction of VT in response to loading is partly mediated by β-endorphins. Data are presented as mean±sem. Modified from 76 with permission.
In humans, in support of the role of β-endorphins, an increase in the β-endorphin plasma level was measured, secondary to resistive breathing 5, 81. It was also demonstrated that naloxone could restore the load-compensatory reflex in patients with COPD in whom it was initially absent 82. In 14 patients with COPD (but without respiratory failure) and eight normal controls, ventilation, mechanical lung function, respiratory sensitivity to carbon dioxide, and the increase in respiratory effort elicited by an increase in resistance to breathing were measured before and after administration of naloxone. Before naloxone, increased resistance to breathing enhanced respiratory effort in all controls, but seven out of 14 patients with COPD had no response. After naloxone, these seven patients had load responses. Furthermore, the respiratory effort elicited by the resistance also increased after the drug was given to the patients who had had a response 82. Moreover, in asthmatics after methacholine challenge inducing severe reductions in forced expiratory volume in one second, pre-treatment naloxone resulted in increased occlusion pressure and mean inspiratory flow rate (two measures of the respiratory drive) when compared with saline pre-treatment 83, which suggested that during metacholine-induced resistive loading, endorphins were suppressing the drive of the respiratory controller to the respiratory muscles, which was augmented after pre-treatment naloxone.
Such a strategy, representing an adaptive response much in the way that β-endorphins are generated in response to chronic pain, certainly minimises dyspnoea and may avoid or delay the onset of respiratory muscle peripheral fatigue, protecting the ventilatory pump from exhaustion. However, it may result in hypoventilation and development of hypercapnia.
Summary
Figure 6⇓ illustrates an integrated view of the origin and functional consequences of resistive breathing-induced cytokines. Resistive breathing results in the generation of oxidative stress and the induction of cytokines within the diaphragm, secondary to the increased muscle activation. Oxidative stress is a major stimulus for this cytokine induction. TNF-α compromises diaphragmatic contractility and contributes to the development of muscle cachexia. IL-6 attenuates the TNF-α expression, secondary to strenuous diaphragmatic contraction. IL-6 mobilises glucose from the liver and free fatty acid from the adipose tissue, which increases the energy available to the strenuously working respiratory muscles.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Integrated view of the origin and functional consequences of resistive breathing-induced cytokines. Resistive breathing results in the generation of oxidative stress and the induction of cytokines within the diaphragm, secondary to the increased muscle activation. Oxidative stress is a major stimulus for this cytokine induction. Tumour necrosis factor (TNF)-α compromises diaphragmatic contractility and contributes to the development of muscle cachexia. Interleukin (IL)-6 attenuates the TNF-α expression, secondary to strenuous diaphragmatic contraction. IL-6 mobilises glucose from the liver and free fatty acid (FFA) from the adipose tissue, which increases the energy available to the strenuously working respiratory muscles. At the same time, cytokines stimulate the hypothalamic-pituitary-adrenal axis either haematogenously or via stimulation of small afferent nerve fibres, leading to production of adrenocorticotropin (ACTH) and β-endorphins. The ACTH response may represent an attempt of the organism to reduce the injury occurring in the respiratory muscles through the production of glucocorticoids by the adrenals and the induction of the acute phase-response proteins. The β-endorphin response would decrease the activation of the respiratory muscles and change the pattern of breathing, which becomes more rapid and shallow, possibly in an attempt to reduce and/or prevent further injury to the respiratory muscles. POMC: pro-opiomelaninocortin; ROS: reactive oxygen species; TG: triglycerides.
At the same time, cytokines stimulate the hypothalamic-pituitary-adrenal axis either haematogenously or via stimulation of small afferent nerve fibres, leading to production of adrenocorticotropin and β-endorphins. The adrenocorticotropin response may represent an attempt of the organism to reduce the injury occurring in the respiratory muscles through the production of glucocorticoids by the adrenals and the induction of the acute phase-response proteins. The β-endorphin response would decrease the activation of the respiratory muscles and change the pattern of breathing, which becomes more rapid and shallow, possibly in an attempt to reduce and/or prevent further injury to the respiratory muscles.
- Received June 8, 2004.
- Accepted August 17, 2004.
- © ERS Journals Ltd
References









