





Abstract
Endobronchial ultrasound (EBUS) allows identification of airway wall structures and could potentially be utilised for in vivo studies of airway thickening in asthma. The present study investigated whether inflation of the fluid-filled balloon sheath over the transducer (necessary to provide sonic coupling with the airway wall) influenced in vitro measurements. In vivo comparability of EBUS with high resolution computed tomography scanning (HRCT), an established method for measuring wall thickness, was determined in control subjects.
The airway diameter and wall thickness were studied using EBUS in 24 cartilaginous airways obtained from four sheep, before and after balloon sheath inflation during immersion in saline. To assess EBUS versus HRCT comparability of airway measures in vivo, 12 control subjects underwent imaging of the posterior basal bronchus of the right lower lobe by both techniques. Intra- and interobserver agreement were also assessed.
Results with and without the balloon sheath gave comparable measures of airway internal diameter and wall thickness in vitro. Statistical analysis showed agreement between EBUS and HRCT, and intra- and interobserver variability in vivo.
The current study concludes that endobronchial ultrasound, which does not present a radiation risk, could be utilised in the in vivo study of cartilaginous airway wall remodelling in respiratory diseases, such as asthma.
This work was supported by the Bournemouth Chest Diseases Charitable Trust.
The endobronchial application of ultrasound (EBUS), using a miniature probe introduced via a fibreoptic bronchoscope biopsy channel, was first described in 1992 1 and has been commercially available since 1999 2. Its current, primary clinical use is in the assessment of tumour/lymph node invasion in cases of nonsmall cell lung cancer 2–4. The technique is safe and well tolerated 1, 5. Recent studies suggest EBUS may have a role in the assessment of peripheral lesions beyond direct vision of the bronchoscope 6, 7 and in nonmalignant parenchymal disease 8.
Ultrasound waves tend to be reflected by air-to-solid interfaces due to poor impedance matching. To overcome this, a saline-filled balloon sheath is inflated between the transducer and the airway wall to facilitate reliable imaging. The probe rotates through 360° within this balloon window to form an image of the airway and its surrounding structures, in the same way as a radar screen on a ship. The 20 MHz EBUS probe has a penetration depth of up to 2 cm, which has been determined to provide the optimum resolution with sufficient airway-wall image penetration 9. If the technique is to be validated for assessment of nonmalignant conditions, such as airway wall thickening in asthma, possible distortions introduced by balloon inflation become important. The balloon sheath, whilst essential when the EBUS probe is used in vivo, may be dispensed with for in vitro experiments, where material may be completely immersed in fluid to provide sonic coupling 10.
Previous in vivo studies of airway wall thickness in asthma have employed high resolution computed tomography scanning (HRCT) 11–14. This technique involves a radiation exposure equivalent to 400 chest radiographs and is not applicable for serial or repeated measurements.
The aim of the present study was, therefore, to validate the use of EBUS as a tool for the measurement of airway wall thickness. To address this, the current study examined whether inflation of the EBUS balloon sheath modified airway internal diameter or thickness in explanted sheep tissue, and assessed the agreement between measurements obtained by EBUS and the existing technique of HRCT in human control subjects.
Methods
In vitro studies
A total of four female, adult, Welsh mountain sheep were sacrificed with i.v. sodium pentabarbitone (150 mg·kg−1) and a post mortem was performed. Six segmental cartilaginous airways, with internal diameters of 4–5 mm and 8–10 mm in length were dissected from each animal, and placed in phosphate buffered normal saline (PBS). Secretions, blood and mucous within the airway were removed by gentle irrigation with PBS. Each bronchus was held vertically by insertion of a 22‐gauge needle through peripheral adventitial tissue away from the area to be studied, before immersion in PBS. The 20 MHz ultrasound probe (PL2220‐20; Hitachi Medical systems, Tokyo, Japan) with its latex balloon sheath was held centrally within the airway and two images were captured electronically (fig. 1⇓). The balloon sheath was inflated twice, to the minimum amount required to cause contact with the airway wall and obtain a 360° image, and again two images were recorded. Ethical approval for the study was obtained from the University and the animals were kept according to the code of practice laid down in the Animals (Scientific Procedures) Act 1986.

Equipment used for in vitro measurement of airway wall thickness by endobronchial ultrasound with and without inflation of the balloon sheath. PBS: phosphate buffered saline.
In vivo studies
Twelve healthy volunteers (four male, eight female) participated in the study, mean±sd age was 37±10 yrs. All subjects had no history of respiratory disease; were nonsmokers or exsmokers who had smoked <5 pack-yrs; had normal spirometry 106±10% predicted; provocative concentration of histamine causing a 20% fall in forced expiratory volume in one second (PC20 histamine) ≥16 mg·mL−1; and negative skin-prick test reactions to five common aeroallergens. Each underwent limited HRCT scanning and subsequent fibreoptic bronchoscopy with EBUS. All subjects gave their informed consent and the study was approved by the local research ethics committee.
HRCT scans were performed on a GE systems HiSpeed CTi (GE Medical Systems, Milwaukee, WI, USA) helical scanner using a high resolution reconstruction algorithm, collimation thickness 1 mm, pitch 1.5 mm, 120 KV and 180 mA. Images were captured with subjects in suspended full inspiration from the level of origin of the right middle lobe to 2 cm above the right hemi diaphragm with a field of view of 13 cm, coned down to cover the basal segments of the right lower lobe.
Fibreoptic bronchoscopy was performed as previously described 15. Briefly, subjects were given i.v. atropine 0.6 mg and i.v. fentanyl 50 µg to suppress coughing. Topical 2% lignocaine was applied to the pharynx and the bronchoscope (Olympus BFXT 40; Olympus Optical Co., Tokyo, Japan) passed transorally with further 1% lignocaine instilled through the bronchoscope as necessary, up to a maximum of 5 mg·kg−1. Arterial oxygen saturation was monitored throughout (Ohmeda, Louisville, KY, USA) and supplemental oxygen given by nasal cannulae if required. A separate EBUS probe to that used in the in vitro work was advanced via the bronchoscope working channel into the posterior basal bronchus of the right lower lobe. The balloon sheath was inflated and deflated three times with an EBUS image captured during each inflation.
Image analysis
EBUS and HRCT images generated in both studies were captured by computer and stored as Digital Imaging and Communications in Medicine format. Image analysis was carried out using Osiris 4.18 (The Digital Imaging Unit, Informatics Center, University Hospital of Geneva, Geneva, Switzerland). In the in vitro experiment on sheep bronchi, the short axis wall thickness (T) and internal diameter (D) were measured directly using electronic callipers, and the mean taken from the two images. In the in vivo study of human volunteers, the previously validated parameters, including wall thickness to external diameter ratio (T/D) 11, 13 and percentage wall area (%WA) 14, 16, were calculated from a mean of three EBUS/consecutive HRCT images (fig. 2⇓). HRCT images were viewed at a window level of −450 Hounsfield Units (HU) and width of 1,500 HU. These settings have been validated in previous studies using phantoms 14, 17, 18.
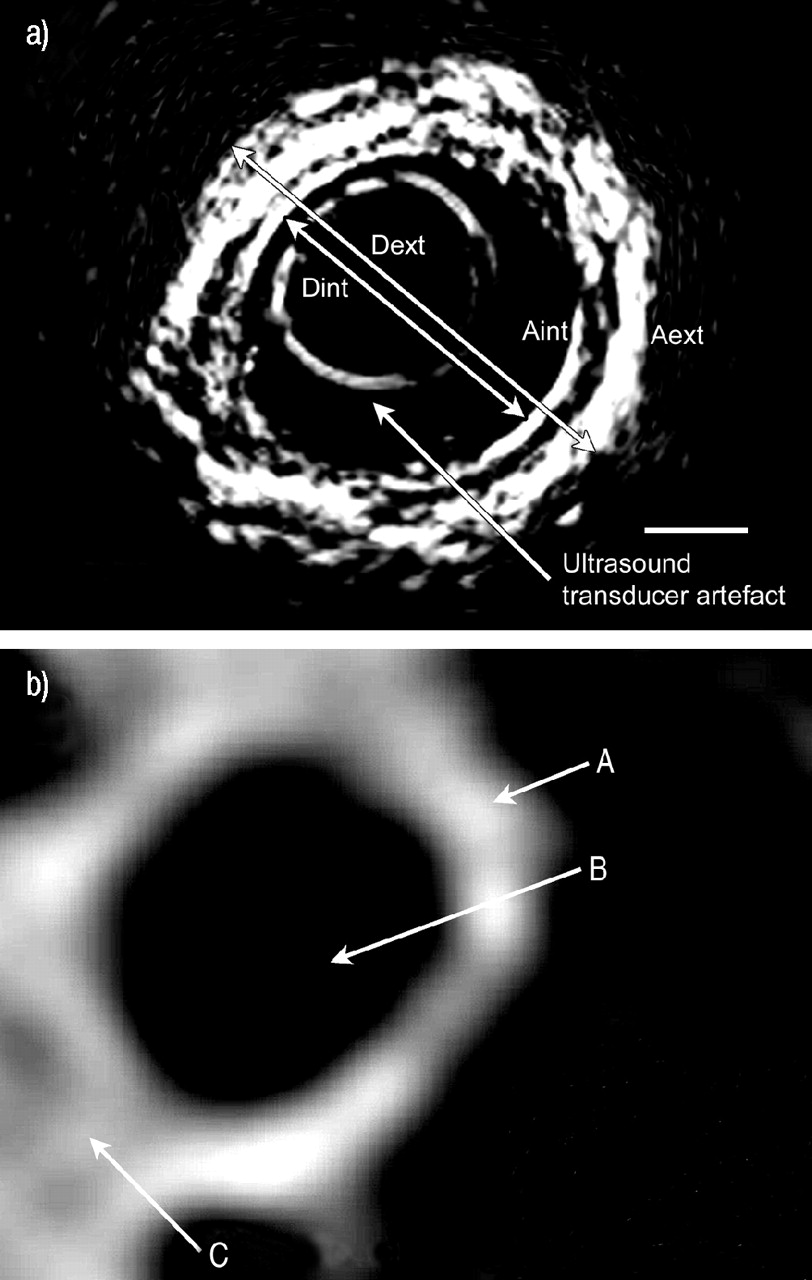
a) In vivo endobronchial ultrasound (EBUS) image of a segmental airway showing EBUS image and measurement of the short axis internal (Dint) and external diameters (Dext). Wall thickness (T; T=(Dext–Dint)/2), wall area (WA) and percentage wall area (%WA) were calculated by tracing the internal and external perimeters to give the corresponding areas (Aint and Aext) (WA=Aext–Aint; %WA=(Aext–Aint/Aext)×100). Scale bar corresponds to l mm. b) Corresponding high-resolution computed tomography image scaled to the same magnification. A: airway wall; B: airway lumen; C: adjacent vessel.
Reproducibility of airway dimensions in the in vivo study
All airway measurements were conducted by a single observer in a blind fashion. Intra-observer variability was tested by this observer independently repeating the measurements after an interval of several weeks. Interobserver variability was assessed by having two observers conduct the same measurements independently.
Statistical analysis
Data were summarised using mean±sd for each airway parameter. The in vitro EBUS airway measurements with and without balloon sheath inflation were compared using the methods described by Bland and Altman 19 and intra-class correlation coefficients (ICC) calculated. EBUS and HRCT measurements of T/D and %WA were also compared using the methods of Bland and Altman 19, and mean within-site coefficients of variation (CV) calculated for each airway parameter. A p-value of <0.05 was accepted as statistically significant.
Results
In vitro studies
A total of 24 sheep airways were studied, with a mean±sd internal diameter of 4.3±0.8 mm and wall thickness of 1.4±0.2 mm without balloon inflation, and 4.2±0.8 mm and 1.5±0.3 mm, respectively, after inflation. Bland and Altman plots comparing measurements with and without balloon inflation are shown in figure 3⇓. Significant agreement was seen between these approaches for both outcome measures: internal diameter, ICC=0.97 (p<0.001) and wall thickness, ICC=0.88 (p<0.001).

Variability in airway internal diameter (D) and wall thickness (T) measured by endobronchial ultrasound with and without inflation of the balloon sheath. ––––: mean; ----: mean±2 sd of the difference, respectively.
In vivo studies
The 12 human airways studied had a mean±sd internal diameter of 4.9±0.9 mm and wall thickness of 1.3±0.4 mm using EBUS, and 5.2±1.0 mm and wall thickness of 1.2±0.2 mm by HRCT. The mean within-site CV for the three measurements of each airway were 12% (T/D) and 7% (%WA). Bland and Altman plots comparing measurements with and without balloon inflation on the airway parameters T/D and %WA are shown in figure 4⇓. In each case the mean difference was close to 0 and there was no obvious relationship between the measurement error and airway parameter.

Variability in airway thickness to diameter (T/D) and percentage wall area (%WA) measured by high resolution computed tomography (HRCT) and endobronchial ultrasound (EBUS). ––––: mean; ----: mean±2 sd of the difference, respectively.
Intra- and interobserver reproducibility
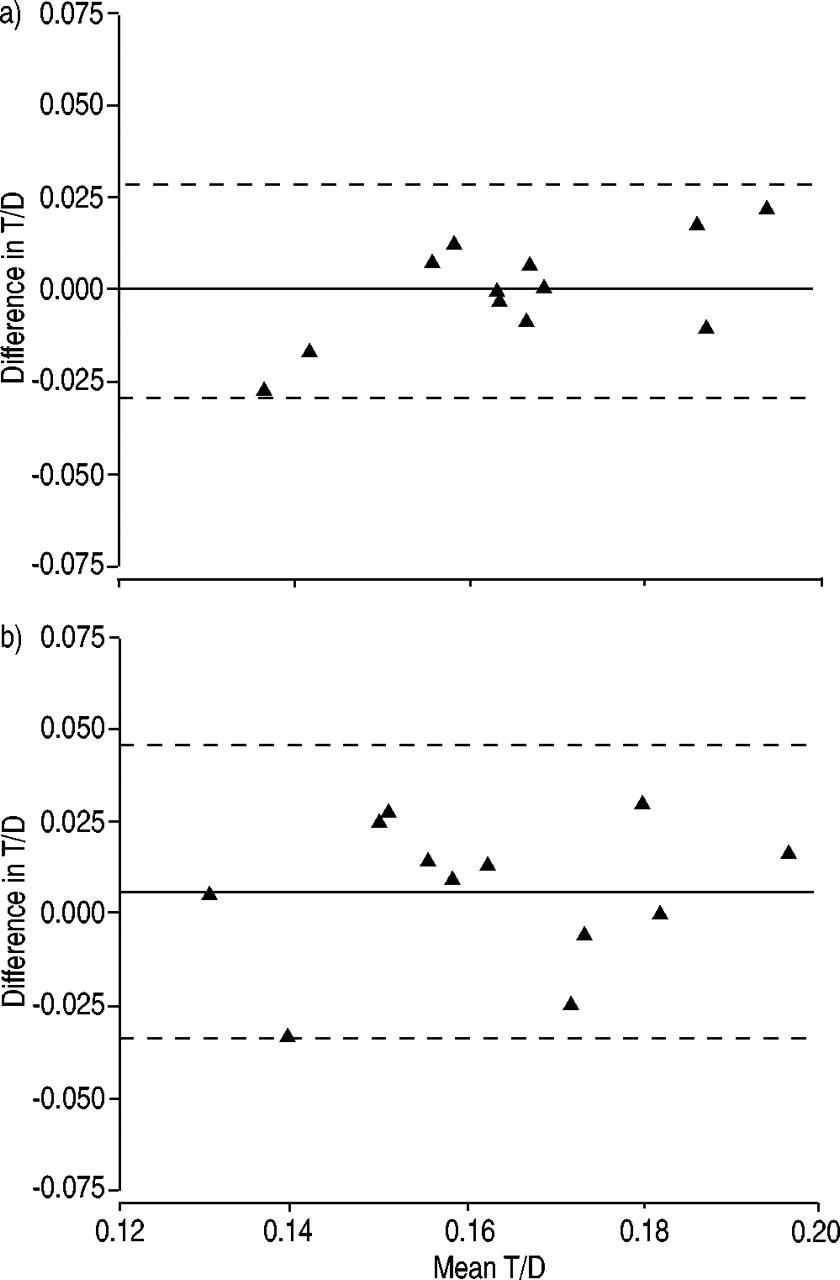
Plots of the mean and the difference between the two T/D ratio measurements obtained to assess intra- and interobserver variability are shown in figure 5⇓. Again, in each case the mean difference was close to 0 and there was no obvious relationship between the measurement error and T/D ratio.
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Variability in airway thickness to diameter (T/D) showing a) intra-observer variability (first versus second readings by observer 1) and b) inter-observer variability (first reading by observer 1 versus reading by observer 2). ––––: mean; ----: mean±2 sd of the difference, respectively.
Discussion
In the present study it has been demonstrated that EBUS can be used to measure airway wall thickness in vivo. The technique was simple to perform and repeat, with three images taking <5 min to obtain. Subjects did not describe undue discomfort, such as pain or coughing associated with the procedure, and no difficulties were experienced with balloon insertion into the segmental airways via the bronchoscope. The measurements made by EBUS were in good agreement with those made by HRCT, but without the radiation risk of the latter technique. As the technique of EBUS involves the inflation of a fluid-filled balloon around the ultrasound probe, to provide sonic coupling to obtain good quality images, the current authors were concerned that this process may compress the airway and alter the wall thickness measures. To evaluate this, comparative measurements with and without the balloon sheath inflated in explanted cartilaginous airways from sheep were undertaken. The current study found that inflation of a balloon sheath around the EBUS transducer did not significantly distort the airway and that there was a close agreement between measurements with and without the balloon. Specifically, the balloon sheath did not cause an increase in the airway diameter or alter the airway wall measurements in airways of this type. The airways studied were of a similar size to those at the segmental level in man.
Ultrasound images recorded in the in vitro study, with the balloon inflated, demonstrated a slightly greater airway wall thickness (∼0.5 mm) than when it was deflated, although this difference did not reach statistical significance. Clearly when the latex balloon sheath is in contact with the airway its thickness is included in the measured wall thickness. However, the sheath is only 0.05 mm thick and this does not account for the observed difference. A more probable explanation is that the sheath-to-wall contact allows the inner airway wall to be identified more readily during image analysis, since the balloon sheath clarifies the density change between that seen in the lumen and the bronchial wall.
The short axis internal diameter was used in the analysis, as it has previously been shown to be less influenced by the effects of partial voluming. This is the apparent increased diameter and wall thickness seen in the long axis dimension when an airway is cut obliquely rather than at right angles 20.
A number of previous studies have utilised HRCT as a tool to measure airway wall thickness in excised canine lungs 17, controls and asthmatic subjects 11–14, 16. Some investigators have found good intra- and interobserver agreement 12, 14, whilst others have shown a discrepancy in interobserver measurements 13. These studies have applied a number of different measures to allow comparison of different sized airways including T/D ratio 11, 13, %WA directly from image analysis 14, 16, derived %WA from airway diameters 13, 21, percentage wall thickness 21 and measures of wall thickness related to body surface area 14. The present study utilised the first two of these measures (T/D and %WA) as they have been validated in studies similar to the present one, looking at more central airways.
The radiation dose resulting from a complete HRCT scan of the thorax is estimated to be 8 mSv, equivalent to ∼400 chest radiographs 22. By limiting the field of view and exposure settings this can be reduced. The calculated radiation exposure to each subject in this study was 0.6 mSv per patient (ImPACT®; Bence Jones Offices, St Georges Hospital, London, UK). None of the studies above quote a figure for radiation exposure. The safety of repeated HRCT measures of airway wall thickness in a prospective longitudinal interventional study is ethically debatable.
The posterior basal bronchus of the right lower lobe was chosen for its convenient orientation, such that the CT images avoid tangential cuts through the airway. Validation of this approach, using a single segmental airway, has been shown in a previous study, which demonstrated good correlation between airway parameters at this site with other areas 14. The apical segment of the right upper lobe, as also studied in the work by Niimi et al. 14 cannot be accessed by EBUS since the transducer is too rigid to permit entry into this lung segment.
In conclusion, this study demonstrates that endobronchial ultrasound is a valid technique for the assessment of total airway wall thickness in vitro and in vivo. Inflation of the saline-filled balloon sheath over the endobronchial ultrasound transducer does not significantly affect airway size or wall thickness of cartilaginous airways, and good agreement is seen between endobronchial ultrasound and high resolution computed tomography measurement of airway wall thickness in control subjects in vivo. The endobronchial ultrasound technique could be applied to the study of the airway wall remodelling changes, such as those seen in asthma, without the radiation risks associated with current techniques.
Acknowledgments
The authors wish to acknowledge the assistance of the Southampton General Hospital Wellcome Clinical Research Facility, Southampton, UK and the research nurse J. Sones.
- Received October 27, 2003.
- Accepted February 11, 2004.
- © ERS Journals Ltd
References









