





Abstract
Lung function in chronic obstructive pulmonary disease (COPD) can be improved acutely by oral corticosteroids and bronchodilators. Whether clinical improvement can be maintained by subsequent inhaled therapy is unknown.
COPD patients (n=1,022, mean prebronchodilator forced expiratory volume in one second (FEV1) 36% predicted) initially received formoterol (9 µg b.i.d.) and oral prednisolone (30 mg o.d.) for 2 weeks. After this time, patients were randomised to b.i.d. inhaled budesonide/formoterol 320/9 µg, budesonide 400 µg, formoterol 9 µg or placebo for 12 months.
Postmedication FEV1 improved by 0.21 L and health-related quality of life using the St George's Respiratory Questionnaire (SGRQ) by 4.5 units after run-in. Fewer patients receiving budesonide/formoterol withdrew from the study than those receiving budesonide, formoterol or placebo. Budesonide/formoterol patients had a prolonged time to first exacerbation (254 versus 96 days) and maintained higher FEV1 (99% versus 87% of baseline), both primary variables versus placebo. They had fewer exacerbations (1.38 versus 1.80 exacerbations per patient per year), had higher prebronchodilator peak expiratory flow, and showed clinically relevant improvements in SGRQ versus placebo (−7.5 units). Budesonide/formoterol was more effective than either monocomponent in both primary variables.
Budesonide/formoterol in a single inhaler (Symbicort®) maintains the benefit of treatment optimisation, stabilising lung function and delaying exacerbations more effectively than either component drug alone or placebo.
- exacerbations
- health-related quality of life
- health status
- inhaled corticosteroids
- long-acting β2‐agonists
Several randomised, controlled trials have shown that long-acting, inhaled β2-agonists improve lung function in chronic obstructive pulmonary disease (COPD) irrespective of disease severity 1, and improve health-related quality of life (HRQL) 2, 3. These improvements equal or exceed those seen with ipratropium 3 or theophylline 4. Only two studies have followed the effects of treatment with long-acting, inhaled β2-agonists over 1 yr 5, 6. The results confirmed the effect on spirometry, but the change in HRQL was smaller than expected.
The role of inhaled corticosteroids (ICS) in COPD is more controversial. Corticosteroids do not appear to affect the rate of decline of forced expiratory volume in one second (FEV1) 7–10. However, ICS increased postbronchodilator FEV1 in two studies 8, 9, and reduced the severity 11 and frequency of exacerbations when this end-point could be reliably assessed 9. These observations have led to ICS being recommended for COPD patients with FEV1 <50% predicted who show a spirometric response 12. In two 1‐yr studies, the clinical effect of ICS on exacerbations requiring oral steroids was confirmed 5, 6; the reduction in exacerbation frequency was less evident for patients taking ICS alone in the study by Szafranski et al. 5. These results may suggest that sicker patients require more than just ICS in their treatment for COPD.
Combining a long-acting β2‐agonist and an ICS as maintenance therapy has been very successful in managing bronchial asthma 13, 14, but less is known about this treatment strategy in COPD. Lung function (prebronchodilator FEV1) is improved when these drugs are combined, compared with monotherapy 15, and recent studies have found that combining therapies is also associated with fewer exacerbations and improved HRQL, compared with placebo treatment 5, 6.
Patients with more severe COPD (Global Initiative for Obstructive Lung Disease (GOLD) stages III and IV) frequently experience exacerbations, which impact on their HRQL 16. Prolonging the time to exacerbation may delay the deterioration of the disease and help maintain health status, an important aim in the treatment of COPD. Moreover, it can be difficult to separate the improvement in health status that occurs at the start of a clinical trial, due to closer medical attention, from the effects of treatment itself, and this caveat can reduce the power of the study to assess the true therapeutic effect on this outcome. To address this difficulty, a clinical trial was conducted in which inhaled formoterol and oral corticosteroids were administered during a short run-in period, to ensure that patients' treatment was optimised before entry into the trial. During the 12‐month, randomised treatment period in patients with COPD, an ICS (budesonide) and a long-acting β2‐agonist (formoterol) given in the same inhaler were compared with the component drugs given separately and with placebo. The primary outcomes were time to first exacerbation and change in FEV1. Data were also recorded on HRQL, peak expiratory flow (PEF), symptoms, use of reliever medication and adverse events (AEs). This protocol allowed the authors to test a clinically relevant situation, namely whether the short-term improvement that follows a period of treatment optimisation can be maintained over a longer time by inhaled therapy, and to investigate which drugs change what aspect of patient well-being.
Methods
Patients
Outpatients with COPD (GOLD stages III and IV) 12 were recruited based on the following criteria: aged ≥40 yrs, COPD symptoms for >2 yrs, smoking history of ≥10 pack‐yrs, FEV1/vital capacity (VC) ≤70% prebronchodilator, FEV1 ≤50% of predicted normal value prebronchodilator, using inhaled bronchodilators as reliever medication, ≥1 COPD exacerbation requiring a course of oral corticosteroids and/or antibiotics 2–12 months before the first clinic visit.
Principal exclusion criteria were: a history of asthma/seasonal allergic rhinitis before the age of 40 yrs, any relevant cardiovascular disorders or significant disease/disorder, which may have put patients at risk or influenced the results of the study, an exacerbation of COPD requiring medical intervention within 4 weeks prior to enrolment and/or during run-in, use of oxygen therapy, β-blocking agents or nonallowed medications. All patients gave written, informed consent and the study was approved by an Ethics Committee for each centre.
Study design
This was a randomised, double-blind, placebo-controlled, parallel-group study involving 109 centres in 15 countries or regions. All medication was from AstraZeneca, Lund, Sweden, and delivered via a dry powder inhaler (Turbuhaler®; AstraZeneca). During the 2‐week run-in, patients received oral prednisolone (30 mg) o.d. and inhaled formoterol (Oxis®) 2×4.5 µg b.i.d., and terbutaline (Bricanyl®) 0.5 mg as needed. Patients were then randomised to 12 months of treatment with either budesonide (Pulmicort®) 2×200 µg b.i.d., formoterol 2×4.5 µg b.i.d., budesonide/formoterol (Symbicort®; this Turbuhaler® delivers the same amount of budesonide and formoterol as the corresponding Turbuhaler® monoproducts) 2×160/4.5 µg b.i.d., or placebo (lactose monohydrate) b.i.d with terbutaline 0.5 mg as needed.
Certain medications were allowed, with restrictions, after randomisation. Courses of oral corticosteroids (maximum 3 weeks per course) and antibiotics were allowed in the event of exacerbations. Parenteral steroids and/or nebulised treatment (single injections/inhalations) were allowed at emergency visits.
The following medications were disallowed from recruitment: inhaled steroids (except the study medication), disodium cromoglycate, leukotriene antagonists or 5‐lipoxygenase (5‐LO) inhibitors, bronchodilators (other than study medication and terbutaline 0.5 mg (Bricanyl®) as needed), antihistamines, any medication containing ephedrine, and β‐blockers, including eye-drops.
The following medications were withheld prior to recruitment: short-acting inhaled or oral β2‐agonists (6 h before), inhaled or oral long-acting β2‐agonists (48 h), inhaled short-acting anticholinergics (8 h), inhaled long-acting anticholinergics (7 days), xanthine-containing derivatives o.d. (48 h), xanthine-containing derivatives b.i.d. (24 h), leukotriene antagonists or 5‐LO inhibitors (48 h).
Assessments
Patients attended the clinics at recruitment, randomisation and after 1, 2, 3, 6, 9 and 12 months of treatment. The primary variables were time to first exacerbation and change in postmedication FEV1. The secondary variableswere number of exacerbations, time to and number of oral corticosteroid-treated episodes, morning and evening PEF, slow VC, HRQL, symptoms, use of reliever medication andAEs.
Exacerbations requiring medical intervention (oral antibiotics and/or corticosteroids or hospitalisation) were recorded at each visit after randomisation. The time to and number of exacerbations and oral corticosteroid-treated episodes were analysed.
Predicted FEV1 was calculated at recruitment using European Respiratory Society (ERS) equations 17. FEV1 was measured before and 15 min after two inhalations of terbutaline 0.5 mg and the per cent increase from baseline in FEV1 was calculated. Spirometry (FEV1 and slow VC) measured after study medication and at least 6 h postreliever, at each clinic visit, met ERS standards 17. Wherever possible, spirometry was performed at the same time of day, using the same spirometer (calibrated on each study day in accordance with the trademark specification), and supervised by the same well-trained study staff. Patients were instructed to rest for 15 min before measurement and spirometry was performed in a sitting position whilst wearing a noseclip. All spirometers met or exceeded the American Thoracic Society recommendations.
Prebronchodilator PEF, measured using a Mini‐Wright® peak flow meter (Clement Clark, Harlow, UK), was recorded daily in a diary, in the morning and evening as the best of three attempts before inhalation of the study medication.
The St George's Respiratory Questionnaire (SGRQ) 18 was used to assess HRQL. Questionnaires were completed at recruitment, at randomisation, and at 6 and 12 months; a Total score was calculated. A lower score indicates better health, while a change of ≥4 units indicates the minimal clinically important difference relevant to the patient 19. Symptoms of shortness of breath, cough, chest tightness and night-time awakenings (on a 5‐point scale from 0 (none, unaware of symptoms) to 4 (severe)), as well as use of reliever medication, were recorded daily in a patient diary. AEs were monitored at each postrandomisation visit by asking a standard question.
Analysis
With 150 patients per group, a difference in survival curves could be detected with 80% power if 66% exacerbated in the reference group and 50% in the comparative group. Adjusting for a 35% dropout rate implied ∼230 patients per group.
An intention-to-treat analysis was used and all hypothesis testing was with two-sided alternative hypotheses; p<0.05 was considered statistically significant. Time to first exacerbation was analysed using a log-rank test and described further by hazard rates from a Cox proportional hazards model, with treatment as factor and stratifying by country. The number of exacerbations was analysed using a Poisson regression model (expressed as mean rate i.e. mean number of exacerbations per patient per year). Treatment and country were used as factors, time in study as an offset variable, and confidence intervals were adjusted for overdispersion. Oral corticosteroid courses were analysed similarly to exacerbations. The FEV1 and VC end-points were the mean of all available measurements during the treatment period, analysed in a multiplicative analysis of variance (with logarithm of values) with treatment and country as factors, and the randomisation value as a covariate. The mean ratios were presented as per cent increases. Both primary variables were required to give statistical significance at the 5% level in order to keep the overall significance level to 5% in the final conclusion 20. Differences in subgroup response were addressed using standard “treatment by subgroup” interaction analyses. SGRQ was analysed in a similar manner to FEV1 but based on the last available measurement on treatment. Diary-card variables were also analysed in a similar manner to FEV1 but with an additive model.
Results
Patients
Of 1,141 patients enrolled into the study, 119 (10%) withdrew during run-in; 26% of these were due to COPD worsening and 24% due to AEs other than COPD worsening. Following run-in, 1,022 patients were randomised, of whom 629 (62%) completed the study (table 1⇓). Mean demographic and baseline characteristics were similar across all treatment groups (table 2⇓) and correspond in general to GOLD stages III and IV COPD 12. After the initial period of treatment optimisation, the group mean FEV1 had increased by (mean±sd) 0.21±0.32 L and the SGRQ Total score decreased by 4.5±10.7 units.
Withdrawal from study
The budesonide/formoterol group had a lower risk of withdrawing from the study compared with the placebo, budesonide and formoterol groups (table 1⇓). There was no significant difference in withdrawal rates versus placebo in either the budesonide group or the formoterol group.
After randomisation, 393 patients withdrew from the study; 193 of these were due to COPD worsening, 72 withdrew because of AEs other than COPD worsening, and 128 for other reasons (table 1⇓). Significantly fewer withdrawals due to COPD worsening were reported in the budesonide/formoterol group compared with the placebo, budesonide and formoterol groups (table 1⇓).
Exacerbations
Budesonide/formoterol prolonged time to first exacerbation compared with all other treatments (all p<0.05, log-rank test; fig. 1⇓). Hazard rate analysis showed that the risk of having an exacerbation while being treated with budesonide/formoterol was reduced by 22.7%, 29.5% and 28.5% versus budesonide, formoterol and placebo, respectively. The exacerbation rate with budesonide/formoterol was reduced compared with placebo (23.6%) and formoterol (25.5%) but not with budesonide alone (13.6%) (table 3⇓). Neither budesonide nor formoterol affected either measure of exacerbation compared with placebo.
When the analysis was restricted to oral corticosteroids given due to exacerbations, the lowest rates were found in the budesonide/formoterol and budesonide treatment groups (table 3⇓). Budesonide/formoterol prolonged the time to first course of oral corticosteroids after randomisation; risk reductions were 32.7% and 33.8% versus budesonide and formoterol, respectively (both p<0.01), and 42.3% versus placebo (p<0.001). Budesonide/formoterol also reduced the rate of oral corticosteroid courses by 28.2%, 30.5% and 44.7% versus budesonide, formoterol and placebo, respectively; budesonide alone reduced the number of oral corticosteroid courses compared with placebo but formoterol did not (table 3⇓).
Lung function
After the optimisation period, the improvement in FEV1 seen during run-in was maintained with budesonide/formoterol treatment throughout the study. In contrast, FEV1 declined greatly and rapidly with all other treatments. This difference was significant with budesonide/formoterol compared with placebo (14%), budesonide (11%) and formoterol (5%), and with formoterol versus placebo (8%), but not with budesonide versus placebo (2%) (fig. 2⇓).
Changes in VC closely followed those of FEV1. Budesonide/formoterol and formoterol improved VC versus placebo (both p<0.001), while budesonide/formoterol also improved VC versus budesonide (p<0.001). Budesonide/formoterol therapy was also associated with higher morning PEF compared with all other treatments, and higher evening PEF compared with placebo and budesonide (fig. 3⇓).
For both exacerbations and FEV1, interaction analyses between treatment and sex, smoking status/history, reversibility or use of ICS at entry, were performed in order to investigate differences in treatment response. There was no evidence of heterogeneity in the treatment differences with respect to the primary variables in any of these categories, i.e.the results in these groups were consistent with the main analysis.
Health-related quality of life
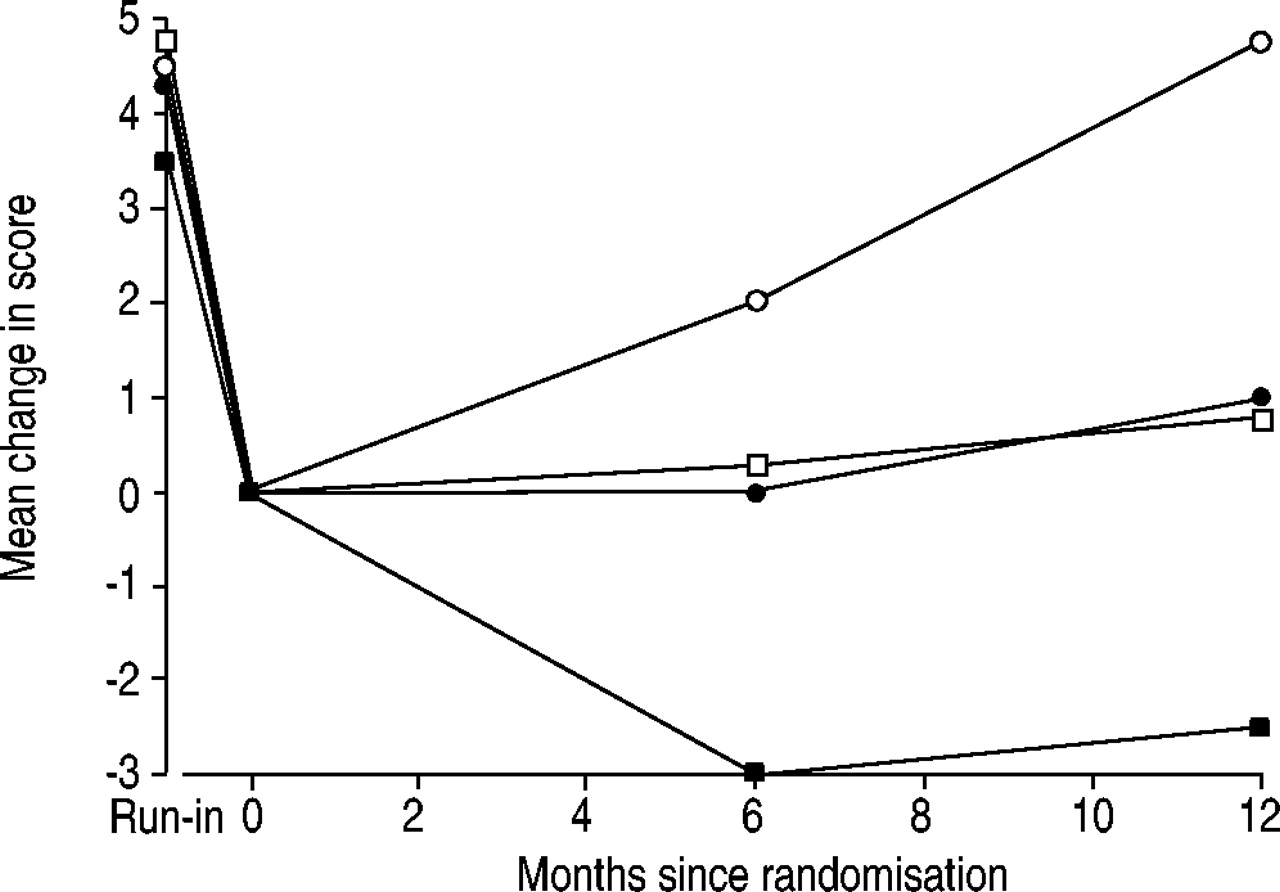
Baseline values for the SGRQ Total score were similar in each group and high, indicating poor HRQL (table 2⇓). At the end of the run-in period, Total scores had improved by a mean of 4.5 units (range 3.6–4.8; fig. 4⇓). During the treatment period, the Total scores fell further in the budesonide/formoterol group, representing an additional improvement beyond that achieved during run-in. Treatment with budesonide or formoterol allowed the initial improvement in HRQL to be maintained, while HRQL in the placebo group deteriorated to the original (prerun-in) values (fig. 4⇓). Thus, all active treatments improved the Total score versus placebo, with the greatest improvement occurring with budesonide/formoterol (differences at 12 months of −7.5, −3.0 and −4.1 versus placebo for budesonide/formoterol, budesonide and formoterol, respectively). Similarly, Symptoms, Activity and Impacts domain scores were each improved by ≥5.5 units inthose patients receiving budesonide/formoterol compared with the placebo group (p<0.01). In addition, budesonide/formoterol showed improvements versus monocomponents inthe Activity (changes of −3.6 versus budesonide and −3.5 versus formoterol, both p<0.05) and Impacts (changes of −5.7 (p<0.001) versus budesonide, and −3.7 (p<0.05) versus formoterol) domains, but not in the Symptoms domain (−2.8 versus budesonide and −0.6 versus formoterol).
Symptoms
Budesonide/formoterol and formoterol improved the total symptom score and the individual symptom scores for shortness of breath, chest tightness and night-time awakenings compared with placebo. Budesonide also improved the night-time awakenings score compared with placebo. None of the treatments significantly improved the cough score. Mean data for changes from run-in to end of treatment in symptom scores and differences between groups are shown in table 4⇓.
Use of reliever medication
Budesonide/formoterol significantly reduced the use of reliever medication by 0.8 inhalations per day versus both budesonide and placebo (both p<0.001), and by 0.3 inhalations per day versus formoterol (p<0.05), and formoterol reduced reliever medication intake by 0.4 inhalations per day versus placebo (p<0.01). Budesonide alone had no effect on this variable compared with placebo.
Safety
No further safety issues for budesonide/formoterol were identified in this study compared with what is previously known for budesonide/formoterol, budesonide and formoterol in COPD and asthma. The mean number of AEs experienced with budesonide/formoterol was no different from that with placebo (5, 5, 6 and 5 AEs per 1,000 treatment days for the budesonide/formoterol, budesonide, formoterol and placebo groups, respectively), and the most frequently reported AEs were similar across the treatment groups (table 5⇓). The lowest number of withdrawals was in the budesonide/formoterol group (table 1⇓) and the lowest number of serious AEs other than deaths were in the budesonide/formoterol and placebo groups (65, 88, 85 and 66 in the budesonide/formoterol, budesonide, formoterol and placebo groups, respectively). The number of serious AEs related to COPD was 40, 40, 55 and 38 in the budesonide/formoterol, budesonide, formoterol and placebo groups, respectively. The numbers of deaths were 5, 6, 13 and 5 in the budesonide/formoterol, budesonide, formoterol and placebo groups, respectively. Most of the deaths were events related to COPD and only a few were related to cardiovascular events.
Discussion
Many clinicians manage newly referred COPD patients by intensifying their treatment, often including a period of oral corticosteroid therapy with the hope of selecting individuals who are “corticosteroid responders”. A substantial number of patients show spirometric improvements with either a β2‐agonist or oral corticosteroids, or both 21. Unfortunately, neither the presence of a “positive” or “negative” oral corticosteroid response in patients with more severe COPD predicts future response to inhaled therapy 9. Whether these improvements in lung function are accompanied by changes in symptomatic end-points like HRQL has not been studied, nor has the ability of inhaled drugs to maintain these effects been assessed, although results from observational studies suggest that at least ICS may be beneficial 22. This study shows that significant short-term improvements in lung function (both FEV1 and PEF) and HRQL occur after optimised treatment with formoterol and oral corticosteroids, and that these improvements can be maintained for a year using budesonide and formoterol in the same inhaler.
This is the first study to show that after an intensification regimen, administration of an ICS and long-acting β2‐agonist in a single inhaler prolongs the time to a first COPD exacerbation, compared with monocomponents. Moreover, these data add further strong support to recent studies where these drug treatment classes have been combined and therapy has initially been withdrawn, rather than optimised, during the run-in phase 5, 6. The exacerbation frequency in this study was almost identical to that reported in the previous study of budesonide/formoterol in COPD patients of a similar disease severity 5, and the effects of each treatment were the same in both studies. In this study, budesonide/formoterol was clearly better than monocomponents at preventing exacerbations, while budesonide had a small effect on episodes where oral corticosteroids were considered necessary. The lack of effect of formoterol may reflect the more severe nature of the episodes used as the outcome here (i.e. requiring medical intervention) rather than the “bad days” used as a surrogate for exacerbations in other studies 3. The similarities of the data presented in this paper to those of Szafranski et al. 5 indicate that prior treatment optimisation does not influence this outcome. The more severe disease in the patients studied (FEV1 36% pred) is the likely explanation of the greater number of episodes seen here compared with other studies 6, 9, a difference that increases the power of the study to detect an effect of treatment. The 24% reduction in exacerbations with budesonide/formoterol compared with placebo may translate into worthwhile improvements in patient well-being. Furthermore, the reductions are probably underestimated since the lowest withdrawal rate occurred in the budesonide/formoterol group. It is likely that the most severely ill patients dropped out first, potentially leading to a lower number of exacerbations in the other groups. To some extent, this bias applies to lung function and HRQL differences as well.
Budesonide/formoterol was able to maintain FEV1 at the run-in level over the study year. In contrast, lung function (both FEV1 and PEF) returned to baseline by 1 month in patients treated with either placebo or budesonide and, as judged by the PEF data from the daily diary cards, this change occurred within 2 weeks of randomisation to these treatments. Numerically, the formoterol data lay between those of the other treatment limbs, but the values were significantly smaller than those measured using budesonide/formoterol. The size of the spirometric changes, comparing budesonide/formoterol with placebo and individual components, was almost identical to that seen when combination therapy was introduced after a period of treatment withdrawal 5, 6, rather than after the intensification regimen used here. The PEF data also show that within 2 weeks of stopping intensified therapy, clinical benefits of treatment optimisation were diminished in all patients not taking budesonide/formoterol.
Budesonide/formoterol produced significant improvements in daily symptom scores compared with placebo, as did formoterol versus placebo (except for cough, which was unchanged). The absolute changes were similar to those seen by Szafranski et al. 5 who used the same questionnaire. Even modest improvements in symptom scores are likely to lead to improved mobility and an increased level of activity. However, there were statistically and clinically significant differences between treatments in their ability to sustain the HRQL improvement after optimisation of therapy. Budesonide/formoterol treatment was associated with the largest difference in the SGRQ Total score compared with placebo, which clearly exceeded the minimum clinically important difference of 4 units 19. Improvements in Total score compared with placebo were also clinically important with formoterol alone, and approached clinical relevance for budesonide alone. The additional effect of budesonide/formoterol on HRQL compared with monocomponents is likely to reflect the lower number of exacerbations experienced by these patients, since HRQL is known to be worse in frequent exacerbators 16.
All the active treatments had some positive effect on HRQL; the change seen over the year in the budesonide group being almost identical to that seen in the less spirometrically impaired Inhaled Steroids in Obstructive Lung Disease study patients, who were also studied after an initial course of prednisolone 9. Inclusion of an optimised treatment phase may overcome problems in assessing HRQL in clinical studies as it reduces the immediate effect of withdrawing ICS that has been associated with more frequent exacerbations 23, 24. This approach should permit a more realistic comparison to be made of treatment effect on HRQL and overcomes the “clinical-trial effect” seen in the placebo limb of other 1‐yr trials 6.
In this study, AEs were monitored by specific enquiry at each visit. No new safety issues related to treatment with budesonide/formoterol were identified during 12‐months treatment. The incidence of AEs related to COPD was clearly lower in the budesonide/formoterol group compared with the other groups, and overall, a low incidence of hoarseness and moniliasis was reported.
This study did not collect bone mineral density data, although the dose of budesonide used did not affect this variable during 3 yrs of treatment in patients with less advanced COPD 25. As expected when studying a COPD population of this severity, a number of deaths occurred. The number of serious AEs and deaths reported were highest in the formoterol treatment group and most of these were events related to COPD. An investigation into the individual causes of death did not give an explanation for the apparent difference between the groups, and no increase in mortality during formoterol treatment without ICS was observed in aprevious study with a similar patient population 5. Conversely, increased disease severity/mortality has been reported in some recently published studies with bronchodilators alone 26–28. These observations, together with the potential seriousness of severe exacerbations, suggest that a combination of a long-acting bronchodilator and an ICS maybe particularly appropriate in patients with this severity of COPD.
The reasons for the improved efficacy of budesonide/formoterol are not yet clear, although corticosteroids can upregulate the number of β2‐receptors on the cell membrane and β2‐agonists may increase the nuclear localisation of glucocorticoid receptors 29. It also seems that formoterol and budesonide in combination are more effective at reducing proliferation of airway smooth muscle than either drug alone, as a result of synchronised cellular signalling 30. Clinically, each type of drug appears to add something to the combined effect with the improvement in symptoms, lung function (FEV1, PEF), and HRQL associated with formoterol being complemented by the reduction in exacerbations and better HRQL seen with budesonide. Whether these effects are merely additive or represent true synergy cannot be established here, but the difference in treatment withdrawal between the group taking budesonide/formoterol and those taking the other treatments is likely to be explained by these multiple beneficial actions.
This study has a number of implications. It provides further and clearer evidence of the effectiveness of ICS and long-acting β2‐agonists on health status, exacerbations, lung function (FEV1 and PEF) and HRQL, in COPD (GOLD stages III and IIV), and of their additional clinical benefit when combined in a single inhaler. Secondly, standardising therapy for a period before entry into a long clinical trial allowed greater improvements in HRQL than seen in similar trials that did not include this run-in treatment. This is a novel approach that may allow for easier interpretation of this end-point, and merits further study.
Finally, this study provides evidence that intensifying treatment in stable chronic obstructive pulmonary disease may be a useful way of rapidly improving patient well-being and that this approach merits future study as an alternative to stepwise increments in treatment intensity.

Kaplan-Meier plot of time to first exacerbation by treatment group. Log-rank tests of budesonide/formoterol (–––) versus budesonide (═), p=0.037; budesonide/formoterol versus formoterol (–– ‐), p=0.002; budesonide versus placebo (- - -), p=0.796; formoterol versus placebo, p=0.490; and budesonide/formoterol versus placebo, p<0.05.
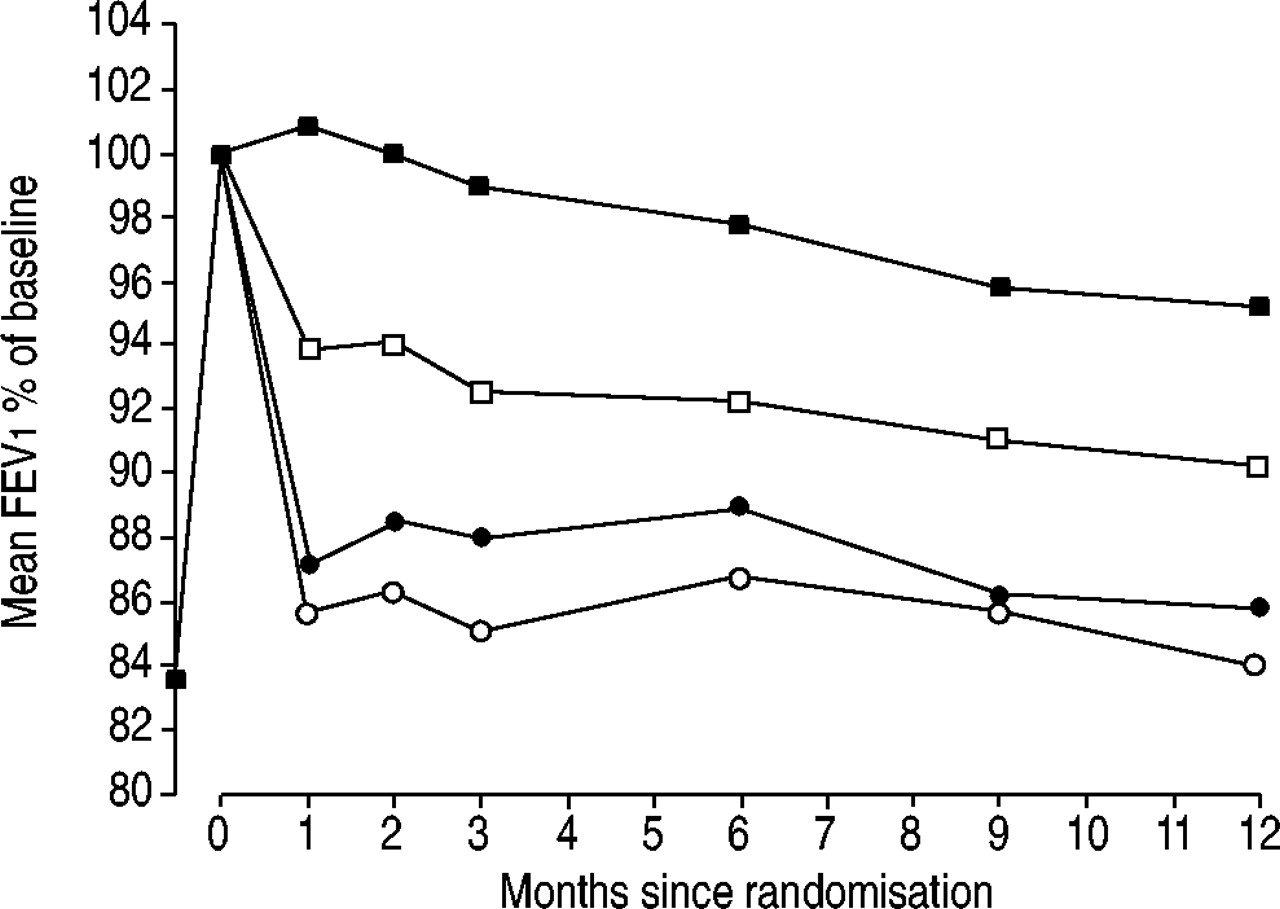
Changes in mean forced expiratory volume in one second (FEV1) in the four treatment groups from randomisation to the average of all available measurements during the 12‐month treatment period. Budesonide/formoterol (▪) versus budesonide (•), p<0.001; budesonide/formoterol versus formoterol (□), p=0.002; budesonide versus placebo (○), p=0.145; formoterol versus placebo, p<0.001; budesonide/formoterol versus placebo, p<0.001.

Change in peak expiratory flow (PEF) from randomisation to the average of all available measurements during the 12‐month treatment period (from daily diary-card data). Budesonide/formoterol (top line) therapy was associated with a) higher morning PEF versus placebo (bottom line; 18 L·min−1 difference, p<0.001), budesonide (line third from top; 15 L·min−1, p<0.001) and formoterol (line second from top; 7 L·min−1, p=0.007). Formoterol versus placebo p<0.001. b) Budesonide/formoterol therapy was associated with higher evening PEF versus placebo (14 L·min−1, p<0.001) and budesonide (12 L·min−1, p<0.001), but not versus formoterol (5 L·min−1) and this improvement was sustained throughout the treatment phase. Formoterol was also associated with placebo (p<0.001).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
Time course of the change in St George's Respiratory Questionnaire Total scores relative to first attendance measured at clinic visits. At 12 months, budesonide/formoterol (▪) versus budesonide (•), p=0.001; budesonide/formoterol versus formoterol (□), p=0.014; budesonide versus placebo (○), p<0.05; formoterol versus placebo, p<0.01; and budesonide/formoterol versus placebo, p<0.001.
Patient flow and withdrawals
Patient demographic and baseline characteristics (at enrolment, unless otherwise stated)
Analysis of exacerbations and oral corticosteroid courses due to exacerbations
Mean changes from run-in to end of treatment in symptom scores
The most frequently reported adverse events (AEs)
Acknowledgments
The authors would like to acknowledge T. Bengtsson and T. Ekström for their contribution to the study design, and thank all of the investigators who recruited and treated patients at the 109 centres involved in this study: Belgium R. Deman, P.J.C. Lorimier, P. Ortmanns, D. Rozen; Brazil J.C. Corrêa, Á. Cruz, J.C.A. de Oliveira, C.C. Fritscher, J.R. Jardim, S. Menna Barreto, R. Stelmach, R. Stirbulov; China P. Chen, X. Hou, S. Niu, L. Yang, N. Zhong; France S. Boutet, T. Brunet, J. Igual, F. Lenique, Y. Martinat, D. Murciano, D. Muller, Y.Pacheco, H. Pegliasco, S. Taieb, P. Zuch; Greece U. Anagnostopoulou, A. Rasidakis; Hungary Z. Cseke, Á.Dévai, G. Juhász, P. Mihalik, É. Molnár, K. Puha, M. Schreiner, Z. Szalay; Malaysia A. Ahmad Mahayiddin; Norway A. Eivindson, G.Gerhardsen, Å.N. Hansen, S. Humerfelt, K.E. Langaker, T. Naustdal, N. Ringdal, T.J.Rødølen, A. Sundset, T. Tomala; Poland M. Czajkowska-Malinowska, M. Gretschel, E. Gross-Tyrkin, P. Kuna, J. Malolepszy, D. Malosek, G. Mincewicz, J. Nowak, Z. Sankowski, P.Sliwinski, T. Stelmasiak, W. Szafranski, M.Szmidt, W. Terlecka; Portugal J.P. Gomes,F. Maria João, A. Marques; South Africa M.S. Abdool-Gafar, C.T. Bolliger, C. Duvenage; Sweden P. Arvidsson, P. Hellke, P. Jakobsson, Å. Johansson, G. Johansson, A. Lindberg, J. Löfvenberg, M. Lundborg, P. Montnémery, E. Piitulainen, K. Ström, M. Tendler, B. Tilling, J. Ziegler; Taiwan J‐F. Shih, H‐C. Wang, C‐P. Wu; Thailand W. Boonsawat, A. Nana; UK A.D. Bremner, M.Britton, R. Brownlie, D. Brydie, T.Evans, J. Gibson, J. Gravil, P. Hardy, B.Hopwood, D. Howarth, D. Keating, K.A. Lindsay, C. Mckinnon, S. O'Hickey, N. Patel, C.Selby, P. Shearer, C. Stenton, D.G. Stoddart, N.C. Thomson, R. Weir.
Footnotes
-
↵ For editorial comments see page 874.
- Received March 11, 2003.
- Accepted July 4, 2003.
- © ERS Journals Ltd
References









