





Abstract
Nitric oxide (NO) is believed to be involved in the pathophysiology of sepsis. This study evaluated the activity of the NO pathway in a human endotoxin model.
At baseline and after endotoxin, on-line measurements of exhaled NO (eNO) were made using a chemiluminescence technique with a single-breath method. NO-free air was inhaled prior to exhalation against a resistance. NO in orally and nasally exhaled air and in rectal gas was investigated. Plasma nitrite, nitrate, and guanosine 3′, 5′-monophosphate (cGMP) and the events after diclophenac administration were also studied.
Endotoxin infusion resulted in tachycardia and fever. An early increase in oral eNO concentration was observed and oral eNO decreased after diclophenac administration. NO exhaled nasally, NO in rectum gas and nitrite/nitrate levels remained unchanged over the study period. cGMP increased after 4 h.
These findings suggest an early increase in nitric oxide production from the lungs, probably due to increased activity of the constitutive nitric oxide synthase upon endotoxin stimulation. In contrast, nitric oxide production in the upper airways, measured as nasally exhaled nitric oxide and nitric oxide in rectal gas, remained unchanged. Further studies will elucidate if exhaled nitric oxide is a valuable marker of sepsis-induced lung injury and if monitoring of treatment is possible.
This study was supported by grants to A. Sollevi from the Swedish Medical Research Council, project numbers 7485 and project number 12586, and to E. Weitzberg from the Swedish Heart Lung Foundation.
Sepsis and the systemic inflammatory response syndrome, with subsequent multiple organ failure, are often the major causes of mortality among severely ill patients in intensive care units. The pathophysiology of sepsis involves activation of vascular endothelium and leukocytes, which results in synthesis and release of various mediators, e.g. cytokines, nitric oxide (NO), endothelin and reactive oxygen species 1. As a local marker of inflammation, NO gas can be used and measured noninvasively. NO production from the respiratory tract, gut and urinary bladder has been shown to reflect inflammation in these organs 2–4. In addition, it has recently been shown that exhaled NO (eNO) from the lungs increases in mechanically ventilated patients with pneumonia 5.
Endogenous NO is continuously produced in small amounts as a natural vasodilator by endothelial cells. Epithelial cells in lungs and gut, for example, also produce NO. The vasorelaxing effect of NO is mediated through the activation of the enzyme guanate cyclase, which leads to production of guanosine 3′, 5′-monophosphate (cGMP).
The production of NO from various cells is difficult to measure in vivo, due to the short half-life of NO. Therefore, nitrite/nitrate (more stable oxidation products of NO) or cGMP in plasma are often measured as markers of NO production. In most biological fluids NO is rapidly scavenged, whereas it remains remarkably stable in the gaseous phase. This has allowed the development of novel techniques to measure NO in the airways and the gastrointestinal tract by analysing the NO content in exhaled air (fractional exhaled nitric oxide (FENO)) or in gas from the gastro-intestinal lumen.
NO is produced by specific enzymes, NO synthases (NOSs) 6, in low (picomolar) concentrations by constitutive NOSs (cNOSs and eNOSs, type-1 and type-3 NOSs). In addition, after inflammatory stimulus, cells such as macrophages produce NO in high amounts 7 via the expression of the inducible NOS (iNOS, type-2 NOS), a process reported to take 6–12 h 8. Such high concentrations of NO are some of the mediators causing the severe vasodilation that result in hypotension and septic shock 9. In addition, iNOS has been shown to be expressed in particular tissues, e.g. the hepatic epithelium and in the epithelium of the paranasal sinus 10.
Increased levels of eNO have been observed in various animals, such as dogs and pigs 11, 12 and, in one study, healthy human volunteers subjected to endotoxaemia 13. In the septic pig, NO release from the gut is unchanged 14 or even reduced 15.
The purpose of this study was to investigate if endotoxin infusion in humans would increase NO levels in the upper and lower airways and in the gut. Nitrite/nitrate and cGMP in plasma were also analysed. Healthy volunteers were exposed to 4 ng·kg−1 Escherichia coli endotoxin, a dose that induces a prominent inflammatory response without being hazardous to the subject 16.
Materials and methods
Study design
Eleven males (age 21–43, mean 29.5 yrs) with good health, as confirmed by history, physical examination, electrocardiogram and haematological screening, participated in the study. None had taken any medication during the 2 months preceding the study. Approval was given by the Ethics Committee of the Huddinge University Hospital, Karolinska Institutet (Stockholm, Sweden) and all subjects gave their informed consent before participating. The subjects were admitted to the Intensive Care Unit at Huddinge University Hospital (Stockholm, Sweden) 2 h after a light breakfast. Intravenous and radial artery catheters were inserted. Electrocardiogram was performed constantly and body temperature was measured by ear thermometer. A 30-min rest period followed the placement of catheters, and thereafter, baseline blood samples were collected from the radial artery catheter and endotoxin was administered intravenously. Blood samples for nitrite/nitrate were collected at baseline, 4 and 6 h and for cGMP at baseline and 4 h. After 4 h the subjects received 50 mg diclophenac rectally and after 6 h the experiment was terminated. Blood pressure, heart rate and temperature were registered hourly. Measurements of FENO and NO in rectal gas and sampling for blood gas content and haemoglobin were performed every hour.
Four healthy male volunteers (age 22–23, mean 22.5 yrs) also without medication for 2 months, served as controls for eNO and possible effects of time and supine position. Four healthy subjects (two males and two females, age 37–46, mean 43.2 yrs) served as controls for hyperventilation and oral eNO. These subjects had their end-tidal carbon dioxide (CO2) measured (Datex end-tidal CO2 monitor; Datex-Ohmeda, Helsinki, Finland). Initially, eNO was measured at rest and then at hyperventilation until side-effects appeared (i.e. 5 min, then NO measuring, then repeated hyperventilation and another NO measuring). After recovery, with normocapnia, the last NO measurement was performed. The control subjects did not receive an artery catheter, endotoxin or diclophenac, or any rectal catheter for measuring NO.
Measurements of nitric oxide in exhaled air
On-line measurements of NO levels were made using a chemiluminescence technique according to the recommendations described for measurement of eNO in the European Respiratory Society Task Force Report using a single-breath method 17. Compressed NO-free air was continuously introduced into a nondiffusing gas collection bag (Hans Rudolph Inc., Kansas City, KS, USA) at a rate of 2–3 L·min−1. The bag was connected via an antiviral filter to a three-way non-rebreathing valve (Hans Rudolph Inc.), which in turn was connected to another antiviral filter. This filter was either directly used as a mouthpiece or was connected to a nose mask. The subject was asked to inhale NO-free air via the nose or mouth and immediately exhale via the same route at a flow of 0.10±0.02 L·s−1 against a resistance of 100 cm·H2O·L·s−1 for a period of 15 s. The exhaled air passed through a linear pneumotachymeter (Hans Rudolph Inc.) after which the resistor (Hans Rudolph Inc.) was connected. Exhaled air was continuously sampled into the NO analyser (77 AM; Eco Physics, Dürnten, Switzerland). The signal outputs from these devices were connected to a computer-based system (Exhaled Breath Analyser; Aerocrine AB, Stockholm, Sweden), yielding an instant on-screen display of flow for biofeedback. NO concentration (FENO) (parts per billion (ppb)=nl·L−1) and NO output were calculated using the equation:  where V′NO is the amount of NO exhaled per unit time.
where V′NO is the amount of NO exhaled per unit time.
The NO concentration FENO showed a stable plateau after an initial peak in all measurements. eNO through the mouth was measured while exhaling through a mouthpiece and eNO through the nose was measured, with a closed mouth, through a nose mask. Nasal values are presented as nasal values minus mouth values, according to a method described by Palm et al. 18. All exhaled measurements were made in duplicate and each data point represents the average of both measurements. The detection limit for NO was 1 ppb.
Measurements of rectal nitric oxide
Rectal NO was measured using the technique described by Herulf et al. 19. An all-silicon catheter (Argyle, No 14; Sherwood Medical, Tullamore, Ireland) equipped with an inflatable balloon was inserted 10–12 cm into the rectum by the volunteers themselves. Lubricating gel free from local anaesthetic was used. The balloon was then inflated with NO-free air and incubated in the rectum for 10 min, allowing NO to diffuse into the balloon. The sample was aspirated and analysed immediately by a chemiluminescence NO analyser (AM 77; Eco Physics). The peak NO concentration was registered. The detection limit for NO was 1 ppb.
Endotoxin administration
The lipopolysaccharide used was National Reference Endotoxin, E. coli (Lot G 1; United States Pharmacopeial Convention Inc., Rockville, MD, USA). The endotoxin was given at a dose of 4 ng·kg−1, made in 0.9% saline solution (1 mL·kg−1) and administered intravenously over 5 min, followed by a flush of 20 mL saline.
Nitrite, nitrate and cGMP in plasma
Nitrite and nitrate concentrations in plasma were analysed with a fluorometric nitrite/nitrate assay kit (Cayman Chemical, Ann Arbor, MI, USA) according to the manufacturers' instructions. cGMP was assayed in plasma after ethanol extraction using a cGMP radioimmunoassay kit (Amersham Biosciences, Uppsala, Sweden) according to the manufacturers' instructions (sensitivity 0.006 nmol·L−1, range 0.02–1.3 nmol·L−1). Blood for analysing nitrite, nitrate and cGMP was collected with a VacutainerTM (Becton-Dickinson Vacutainer Systems Europe, Plymouth, UK) in 5 mL standard ethylenediamine tetraacetic acid tubes.
Haemoglobin and arterial carbon dioxide tension
Blood gas samples were analysed with a Rapidlab 855 blood gas instrument (Bayer Diagnostics®; Tarrytown, NY, USA) and haemoglobin was analysed using an Advia 120 haematology instrument (Bayer Diagnostics®).
Statistics
Descriptive statistics are presented as mean±sem. Statistical analysis was performed using single-factor repeated measures used for evaluation by Friedman's analysis of variance. For cGMP, a paired t-test was used.
Results
Physiological variables
All volunteers that entered also completed the study. There were no unexpected side-effects. Systolic blood pressure increased significantly (p<0.001) and diastolic blood pressure decreased significantly (p<0.001) after 2 h. Heart rate and body temperature increased significantly (p<0.001). The carbon dioxide tension (Pa,CO2) decreased after 2 h and remained unchanged throughout the study period. Haemoglobin decreased from the fourth to sixth hour (table 1⇓).
Body temperature, haemodynamic parameters, arterial carbon dioxide tension (Pa,CO2) and haemoglobin at baseline and after endotoxin infusion
Nitric oxide in exhaled air and from the rectal catheter
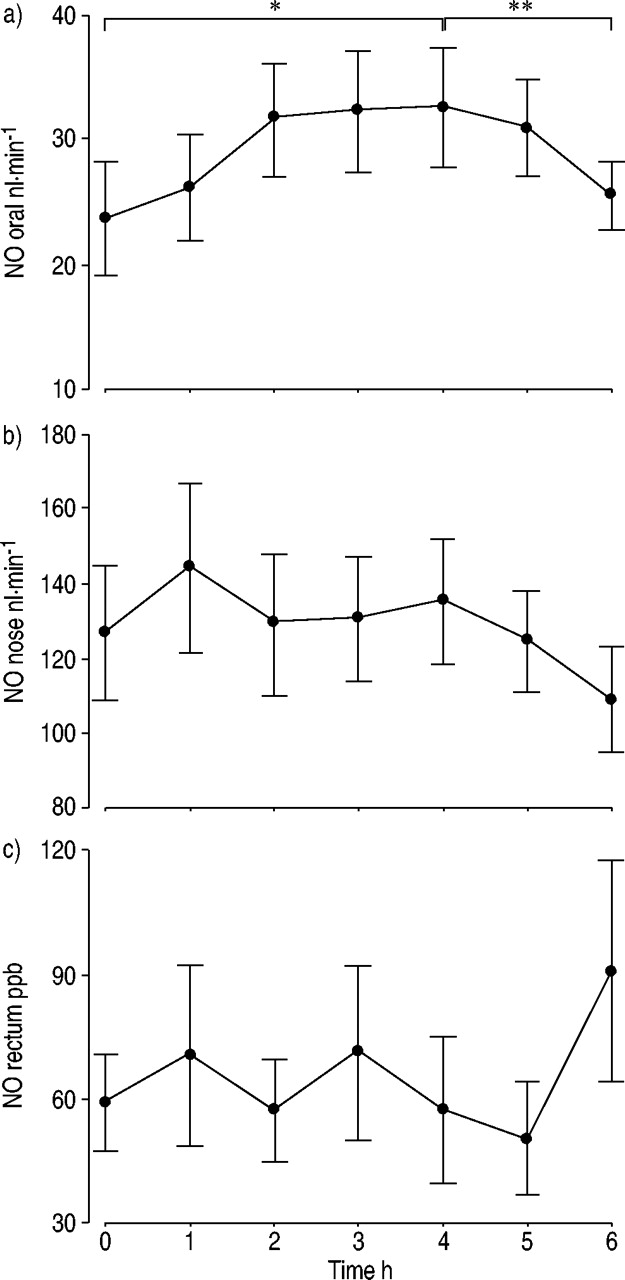
Oral eNO, VNO, increased in all 11 subjects (fig. 1a⇓). Mean values increased by 33% (p<0.001) from baseline, 24±5 nL·min−1 to 32±4 nL·min−1, after 2 h and then reached a plateau. Oral VNO showed a significant (p<0.05) decrease back to baseline values observed 1 and 2 h after diclophenac administration.

Nitric oxide (NO) concentrations in a) orally and b) nasally exhaled air. c) NO concentration measured from the rectum. Measurements were performed before and every hour, during the 6 h after endotoxin infusion. Diclophenac (50 mg rectally) was administered after 4 h. NO exhaled nasally and NO in rectum gas did not change significantly over the study period. Each value indicates mean±sem. *: p<0.001; **: p<0.05.
Nasal eNO did not change during the course of the experiment (p=0.52). Baseline values were 127±18 nL·min−1 and 135±17 nL·min−1 at 4 h. Nasal eNO did not decrease after diclophenac administration (p=0.06) and at 6 h was 109±14 nL·min−1 (fig. 1b⇑). The control group showed no statistical change over the study period in oral eNO or nasal eNO. Oral eNO was 28.9±5.2 nL·min−1 at baseline and 30.5±4.1 nL·min−1 at 4 h. Nasal VNO was 72±8 nL·min−1 at baseline and 95±26 nL·min−1 at 4 h. The controls regarding hyperventilation had at-rest end-tidal CO2 of 5.0±0.28 kPa, then 2.5±0.13 kPa after the first period of hyperventilation, 2.3±0.12 kPa after the second and 4.8±0.35 kPa after recovery. Oral eNO values were 33±10 nL·min−1, 28±8 nL·min−1, 32±10 nL·min−1 and 31±10 nL·min−1, respectively. Basal levels of rectal NO were 59±11 ppb, then 58±18 ppb at 4 h and 91±26 ppb at 6 h, and did not show any significant difference (p=0.46) over the study period (fig. 1c⇑).
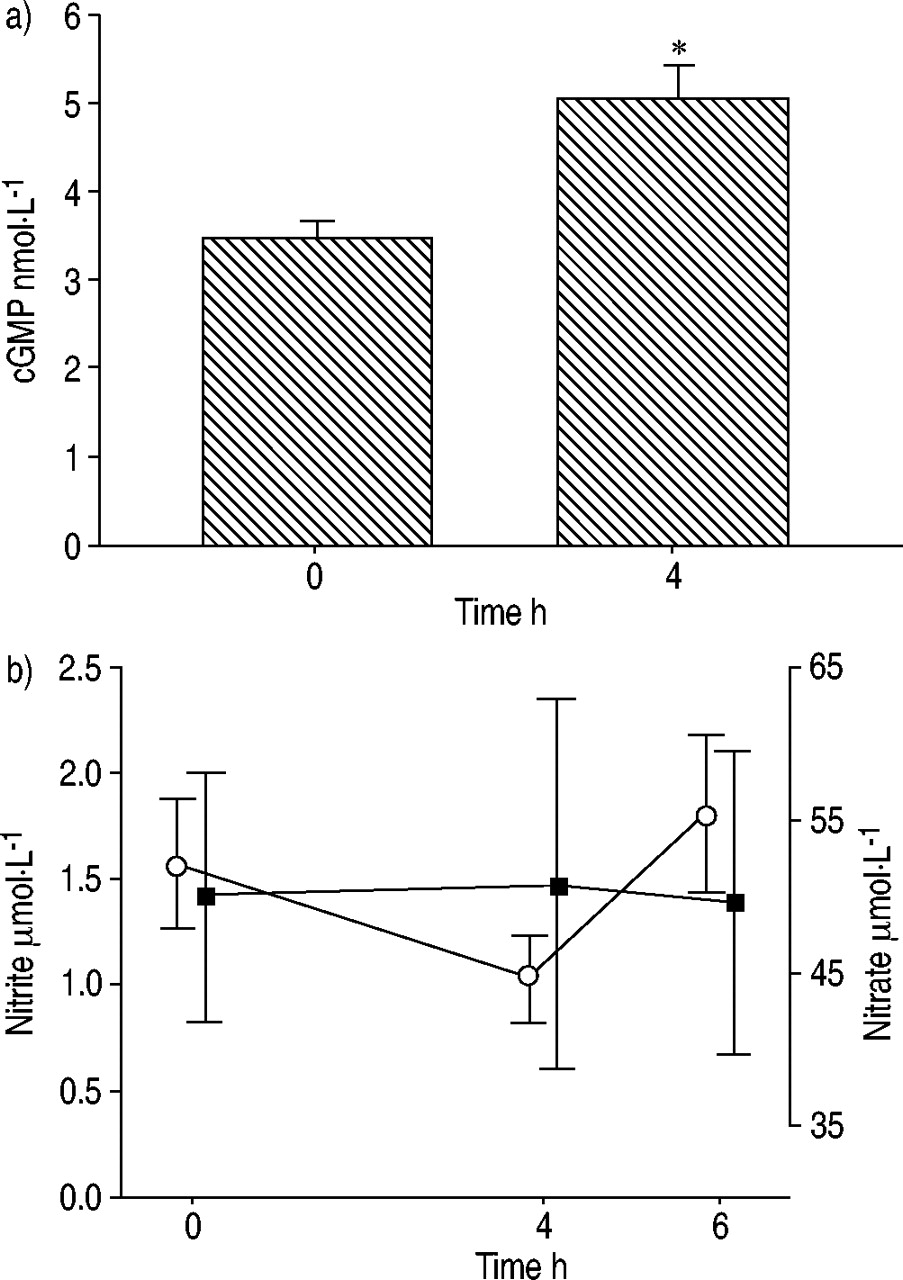
cGMP, nitrite and nitrate
cGMP increased in all 11 subjects, from 3.46±0.19 nmol·L−1 at baseline to 5.06±0.35 nmol·L−1 4 h after endotoxin (p=0.02, fig. 2a⇓). Nitrite and nitrate levels in plasma were not significantly changed over the study period (fig. 2b⇓). Nitrite baseline levels were 1.57±0.31 µmol·L−1, 1.03±0.20 µmol·L−1 after 4 h and 1.8±0.36 µmol·L−1 at 6 h. Nitrate baseline levels were 50.1±8.1 µmol·L−1, 50.8±12.0 µmol·L−1 after 4 h and 49.6±9.9 µmol·L−1 at 6 h.
{kind=link}
{kind=link}
a) Cyclic guanosine monophosphate (cGMP) in plasma before and 4 h after endotoxin. b) Mean±sem plasma levels of nitrite (○) and nitrate (▪) before and 4 and 6 h after endotoxin challenge, there was no significant change over the study period. Diclophenac (50 mg rectally) was administered after 4 h. *: p=0.02.
Discussion
The primary finding of this study was that oral eNO increased upon endotoxin administration, indicating enhanced production of NO from the lower airways. Nasal eNO was not significantly changed by endotoxin. Further, plasma cGMP increased 4 h after endotoxin compared to baseline levels, whereas nitrite/nitrate in plasma was unchanged. Increased heart rate, fever and blood pressure response indicate that the volunteers responded to the endotoxin.
eNO has been extensively studied, mainly in patients with asthma showing increased levels corresponding well with the grade of inflammation and anti-inflammatory treatment with steroids 2. Further, NO in exhaled air has been shown to increase early after endotoxin challenge in animal models 11.
In a study by Vandivier et al. 13, eNO increased ∼3 h after endotoxin infusion in healthy volunteers, which is in accordance with the findings of this study. Vandivier et al. 13 performed measurements with a noseclip and without exhalation against an expiratory resistance. Such an approach would greatly increase the risk of contamination with nasal NO to orally exhaled levels 20. In the present study, the highly standardised method for eNO recommended by the European Respiratory Society and the American Thoracic Society was used 17, 21. This includes exhalation against a resistance at a fixed flow rate and allows for good separation of lower airway NO from nasal NO. It is therefore very likely that the increased oral NO observed in the current study derives from the lower airways or the lungs. This study found a decrease in Pa,CO2, indicating hyperventilation. However, this decrease lasted throughout the study period, while the levels of eNO started decreasing and returned to near baseline values after 6 h. Hence, the authors suggest that there is no connection between the decrease in Pa,CO2 and the increase in eNO. It appears that the levels of eNO are not due to hyperventilation per se, provided the measurements are performed using a constant flow. It is important to stress that during flow-controlled single-breath exhalations hyperventilation should not influence eNO. To the authors' knowledge there are no such studies in the literature. However, it could be argued that the decrease in oral eNO observed from 4–6 h is connected to the decrease in hyperventilation expected when the CO2 production decreases in parallel with fever reduction. In the four control subjects, no indication of correlation between hyperventilation and oral eNO was found. The early increase in NO production after endotoxin seen in this study, within 2 h after triggering the inflammatory reaction, indicates that there is an augmented activity of cNOS in the lungs rather than an upregulation of iNOS expression, since iNOS induction upon endotoxin and/or cytokines, in the experimental setting, is known to take ≥6–12 h 8. These findings are in line with previous studies in animal endotoxin models. Hussain et al. 12 found elevated levels of eNO in endotoxic dogs within 30 min, while there was no evidence of iNOS induction. The increase in eNO after endotoxin in rats can be blocked by NOS inhibitors, such as N-nitro-l-arginine methyl ester 22. Taken together, these data suggest increased activity of cNOS in the lower airways and lungs, which of course does not exclude iNOS derived eNO in the later phases of the systemic inflammatory response.
Previous studies have suggested that oral eNO represents NO from the lower airways 23. However, it has been shown that oral NO production exists and is dependent on intake of nitrate, which is reduced to nitrite and further to NO by bacteria in the oral cavity 24. Recently, the authors observed that the oral cavity and oropharynx contributes to approximately half of the NO levels in orally exhaled air, shown by measuring NO production from tracheotomised patients 25. The authors therefore cannot disregard the fact that the increase in oral eNO after endotoxin challenge derives from NO produced in the mouth. However, the volunteers 2-h fast in the current study is a contradicting factor. In addition, plasma levels of nitrite and nitrate remained stable, which argues against an increased secretion of nitrate into the oral cavity. Therefore, the authors hypothesise that the increase in orally exhaled levels of NO measured in the current study is a sign of inflammatory response and reflects a change in NO production in the lower airways. It is known that endotoxin challenge to human volunteers increases cardiac output but does not influence mean pulmonary artery pressure during the first 3 h 26. The possible effects of alterations in the pulmonary blood flow on eNO have previously been investigated in humans. Changing pulmonary blood flow had no effect on this mechanism 27. An increase in pulmonary blood flow would allow haemoglobin to bind more NO per time unit, which, theoretically, could result in a decrease in eNO.
No significant change in nasal NO production upon endotoxin challenge was found. The method of subtracting the orally from the nasally exhaled levels was used 18. This method is proposed to reflect upper airway NO production although several other methods have been suggested 21. The amount of NO exhaled from the nose is approximately five times higher compared to NO exhaled from the mouth. The authors speculate that such a relatively small amount of increase as seen in the orally measured NO would easily be blunted by the background NO in the nose.
The decrease in NO production from the lungs after diclophenac administration shown in the current study is in accordance with previous findings where a cyclo-oxygenase inhibitor (ibuprofen) decreased alveolar NO flow rates 13. These findings give further strength to the possibility that a nonsteroid anti-inflammatory drug (NSAID) inhibits the activity of eNOS or iNOS or both, as previously shown in in vitro studies 28 and in pigs 29. With the present study design, it was not possible to draw any conclusions of the effect of diclophenac on NO production. However, it could be speculated that there is NOS expressed in the lungs, with a decreased activity regulated by NSAID.
There was no change in NO levels from the gut after endotoxin challenge or after diclophenac administration. In local inflammatory diseases, NO from the gut lumen is markedly increased 30. In porcine inflammatory models, NO release from the gut is unchanged 14 or even reduced 15. The difference in results might be due to the difference in local versus systemic inflammation or, as previously mentioned, the time for the expression of iNOS. Species-specific conditions may also play a role. The dose of endotoxin should be considered, as in pigs it can reach 20 µg·kg−1·h−1 compared to human volunteers who receive 4 ng·kg−1 once.
The increase in plasma cGMP 4 h after endotoxin is contrary to that reported by Vandivier et al. 13, where both urinary and plasma levels of cGMP were unaltered by endotoxin and by endotoxin combined with an NO donor. The current study used a radioimmunoassay, whilst Vandivier et al. 13 used an enzyme immunoassay method to analyse cGMP. Both are well known, widely used methods and, according to the manufacturer, comparable. It is not apparent why different results are obtained. However, the current study used different lots of E. coli, which might have implication 16. In septic patients, plasma cGMP increases 31 and, in volunteers, NO inhalation increases plasma cGMP in a dose-dependent manner 32. Further studies to assess the effect of endotoxin challenge on cGMP seem warranted.
As in the study by Vandivier et al. 13, nitrite/nitrate levels in plasma remained unchanged after endotoxin challenge. This is contrary to previous in vitro findings 33 as well as findings from studies in patients with septicaemia 34. Other authors have stated that the plasma nitrite/nitrate levels may not always reflect NO production 35. In addition, the authors have previously found that nitrite/nitrate levels remain unchanged 1–4 h after endotoxin challenge in healthy volunteers (A. Soop, unpublished results). However, Vandivier et al. 13 found elevated urinary levels of nitrite/nitrate in the late follow-up time, which might reflect an activation of iNOS.
In summary, this study found enhanced nitric oxide production from the lungs after endotoxin challenge in healthy human volunteers. Advantages of measuring nitric oxide in exhaled air are that the method is noninvasive and provides immediate and continuous results. Further studies will reveal whether this method has a place in the intensive care unit monitoring arsenal to measure inflammatory response during sepsis.
Acknowledgments
The authors would like to thank I. Hellström and C. Nihlén for skilful technical assistance.
- Received March 27, 2002.
- Accepted October 22, 2002.
- © ERS Journals Ltd
References









