





Abstract
T-helper (Th)2 cytokines play a central role in asthma. Therefore, a double-blind randomised study was conducted to investigate whether heat-killed Mycobacterium vaccae (SRL172), a potent downregulator of Th2 cytokines, can reduce allergen-induced airway responses in patients with atopic asthma.
A total 24 male asthmatics participated in this study. A bronchial allergen challenge was performed along with early (EAR) and late asthmatic responses (LAR) 2 weeks before and 3 weeks after a single intradermal injection of SRL172 or placebo. Before and after treatment, serum immunoglobulin (Ig)E levels and in vitro production of interleukin (IL)-5 by peripheral blood lymphocytes were studied.
Neither treatment affected the EAR. SRL172 caused a mean 34% reduction of the area under the curve of the forced expiratory volume in one second (FEV1) changes during the LAR, which failed to reach conventional statistical significance when compared with placebo. SRL172 also caused a mean 25% decrease in the maximum fall in FEV1 during LAR, but this was not significantly different from placebo. SRL172 caused a reduction in serum IgE and IL-5 synthesis in vitro 3 weeks post-treatment (p=0.07).
This study shows a trend toward significance for the effects of heat-killed Mycobacterium vaccae (SRL172) on allergen-induced airway responses. Further clinical trials, involving multiple dosing, are needed.
Bronchial asthma is characterised by chronic airway inflammation that is orchestrated by activated T-helper (Th)2 cells producing interleukin (IL)-4 and -5, which promote airways eosinophilia and Immunoglobulin (Ig)E synthesis 1. Whilst, in healthy individuals, Th2 cells are normally in balance with Th1 cells, which produce IL-2 and interferon (IFN)-γ, in atopic asthmatics their frequency and activity within the airways is increased 2.
The reasons for the recent rise in asthma prevalence remain unclear. Recent epidemiological studies have suggested the “hygiene hypothesis”, according to which the increased prevalence of atopic diseases has been, at least in part, due to reduced early childhood exposure and subsequent inadequate development of immunity to infectious agents 3–6. Many bacteria and their components can exert modulating effects on immune cells, including cell wall components of Gram-negative bacteria (lipopolysaccharide), mycobacteria 7 and deoxyribonucleic acid (DNA) containing immune-stimulating sequences (ISS, CpG motifs) 8. Mycobacteria may be one of the agents that may have the potential to protect against development of Th2 diseases 7. The reactivity of mycobacteria has been shown to be associated with a lower risk of atopy 9. As a consequence of changes in lifestyle, and changes in the bacilli Calmette-Guérin (BCG) vaccination programmes in the industrialised world, exposure to mycobacteria may have decreased whilst exposure to allergens has increased. This may have impaired the natural maturation of the immune system that occurs in childhood from a predominant Th2 response to a balanced Th1- and Th2-type immunity 10, 11, or alternatively, it may have impaired maturation of immunoregulation 7.
This study tested the hypothesis that the nonpathogenic mycobacterial species Mycobacterium vaccae can attenuate asthmatic reactions that occur following allergen challenge. Asthmatic volunteers received a single intradermal injection of SRL172, a preparation containing 1×109 (1 mg) heat-killed M. vaccae (SRL172) has been used in previous clinical studies involving patients with pulmonary tuberculosis 12, melanoma 13, cancers of the prostate 14 and cancer of the lung 15, 16, where the aim has been to promote Th1 cytokine-dependent immune defences. Following observations that M. vaccae suppresses established IL-5 and IgE synthesis in ovalbumin-sensitised mice 17 and evokes regulatory T-cells that downregulate Th2 responses 18, it was further hypothesised that it may be able to reduce Th2 responses not only in developing allergic disease but also in chronic adult asthma. In addition to testing the effect on the magnitude of the airways response, this study conducted an exploratory investigation into the ability of SRL172 to reduce serum IgE levels and downregulate allergen-induced in vitro synthesis of IL-5 by peripheral blood mononuclear cells (PBMC).
Methods
Subjects
A total of 24 male atopic asthmatics (mean age 34.8 yrs, range 20–53 yrs) with mild-to-moderate disease were recruited (table 1⇓). All the subjects demonstrated an early (EAR) and late airway response (LAR). The subjects either had mild asthma (n=15), requiring only inhaled β2-agonists, or moderately severe asthma (n=9), with daily symptoms requiring the use of low-to-moderate doses of inhaled corticosteroids (<600 µg of beclomethasone dipropionate or equivalent per day). Individuals with a history of smoking during the previous 12 months, alcohol or drug abuse, or serious adverse reactions to medications were excluded. None of the subjects reported a respiratory infection or required prescription medication, other than that for asthma, within 14 days prior to the study and none of the subjects had used oral corticosteroids within the previous 6 months.
Subject characteristics
The study was approved by the Southampton University (Southampton, UK) and the Hospital Ethics Committee and subjects gave their written informed consent.
Study design
This was a randomised, placebo-controlled, parallel-group Phase I study. Subjects attended the department on nine separate occasions (fig. 1⇓).

Study design. SRL172: Mycobacterium vaccae; PBMC: peripheral blood mononuclear cells; IgE: immunoglobulin E.
At the first screening visit, medical history was taken and a physical examination, routine haematological and biochemical tests, urinalysis and skin-prick tests were performed. In addition, baseline responsiveness to histamine was measured. After the first visit there was a run-in period of 28 days where the disease activity was recorded on diary cards in order to ascertain asthma stability. The first allergen challenge was performed at visit 2 using an incremental-dose challenge protocol. The following day (visit 3) subjects underwent a histamine challenge to assess any change in responsiveness, secondary to allergen challenge. Two weeks later (visit 4) blood was drawn for the first in a series of three PBMC cultures and serum IgE measurements. Subjects then received an intradermal injection of 0.1 mL (1 mg) of SRL172 or placebo into the lateral aspect of the deltoid muscle region on the left arm. After 3 days they returned to the department for recording of any local reaction (visit 5). Eighteen days after injection (visit 6), haematology and biochemistry blood tests, urinalysis and serum IgE measurement were repeated. At visit 7 (3 weeks after the injection), a second blood sample was taken for PBMC culture and allergen challenge was repeated. This was followed by a histamine challenge the next day (visit 8). Subjects were followed-up until 42 days postinjection (visit 9) when a full medical examination was conducted, a third blood sample was taken for serum IgE, PBMC culture, haematology, biochemistry and urinalysis was performed.
In order to avoid observer bias, a pharmacist at the Southampton General Hospital prepared the study medication and a physician blinded to the study administered the injections. Furthermore, the site of injection was concealed from other investigators with a bandage.
Allergen and histamine inhalation challenge
Allergen challenge was performed using a modification of an established protocol 19. If subjects were taking regular inhaled beclomethasone they stopped treatment 5 days before allergen challenge to enable an LAR to develop. Allergens that produced the greatest wheal response were used. After taking five breaths of physiological saline to ensure the absence of nonspecific airways irritability, subjects inhaled increasing concentrations of allergen solution (Aquagen: ALK, Horsholm, Denmark). Beginning with 1 Standardised Quality Units (SQ)·mL−1 and increasing 10-fold at 15 min intervals up to 10,000 SQ units·mL−1 or until a fall in forced expiratory volume in one second (FEV1) of ≥25% from postsaline baseline had been achieved (EAR). FEV1 measurements were recorded at 20, 30, 45 and 60 min and, thereafter, hourly for 8 h. An LAR was defined as a fall in FEV1 >15% from postsaline baseline between 3 and 8 hr postchallenge. Subjects were then routinely given 2.5 mg of nebulised salbutamol and allowed home. They returned the following morning for histamine challenge using a previously reported protocol 19. A second allergen challenge was performed 3 weeks after the injection, using an identical increasing concentration regimen and the same total dose as used on the first occasion.
In vitro interleukin-5 responses to allergen
PBMC were isolated from 20 mL of heparinised venous blood by Ficoll-Hypaque gradient centrifugation (Lymphoprep Nycomed Pharma AS, Oslo, Norway). Cells were washed twice and resuspended at 2×106 cells·mL−1 in Rosswell Park Memorial Institute (RPMI) 1640 medium supplemented with 1 mM sodium pyruvate, 2 mM l-glutamine, 100 U·mL−1 penicillin, 100 µg·mL−1 l streptomycin, 50 µM 2-mercaptoethanoll (all from GibcoBRL, Life Technologies, Paisley, UK), and 5% heat-inactivated human AB serum (SIGMA Ltd, Poole, UK), and cultured for 48 hr at 37°C in 5% carbon dioxide (CO2) in the presence or absence of house dust mite allergen extract (Dermatophagoides pteronyssinus; ALK) at a concentration of 5,000 SQ units·mL−1. The dose of allergen was chosen from pilot experiments as causing the greatest increase in IL-5 synthesis. Culture supernatants were assayed by commercial enzyme-linked immunosorbent assay (ELISA) kits for IL-5 levels (CytoScreenTM; BioSource International, Inc. Camarillo, CA, USA) with sensitivity at 4 pg·mL−1.
Serum immunoglobulin E
The total serum IgE was measured by the Regional Immunology Laboratory, Southampton General Hospital, by ELISA, using a monoclonal anti-IgE antibody developed in-house and a commercially available anti-IgE antibody (Dako, High Wycombe, UK).
Statistical analysis
The principal outcome variables were as follows: maximum percentage fall in FEV1 during the first 2 h following allergen challenge (EAR) and between 3 and 8 h after allergen challenge (LAR), and changes in histamine responsiveness 24 h postallergen challenge. The primary outcome on which power calculation was performed was the maximum fall in FEV1 during the LAR. Studies of intersubject variability and reproducibility of late-phase responses have shown that in order to demonstrate a 30% reduction in the LAR, with 95% power and probability of <5% of the difference occurring by chance, 12 subjects are needed 20. The changes in FEV1 were also expressed as areas under the curve (AUC) for the EAR and LAR. The AUC was calculated using trapezoid integration as the area between the curve and the x-axis and divided by the duration (first 2 h for the EAR and 3–8 h for the LAR) over which the AUC was calculated. Comparisons of changes in maximum percentage falls in FEV1, AUC for the EAR and LAR, and provocative dose causing a 20% fall in FEV1 (PC20) as a result of treatment with SRL172 or placebo were performed using formal analysis of variance models (ANOVA). Within-group changes in the same were made by paired t-test. The changes during the course of the study in IL-5 production in vitro and serum IgE levels relative to the first measurement were expressed as AUC by trapezoid integration of the percentage change at the three time-points. This test was used as it takes into account the dynamics of IgE and IL-5 over the whole course of the study and does not rely on individual time-points alone. The AUC in the two treatment arms were then compared by Mann-Whitney U-test, assuming a non-normal distribution. The changes in IgE levels and IL-5 synthesis in the two treatment groups were also compared using the Fisher's exact test.
Results
Treatment was well tolerated by all subjects and all the haematological, biochemistry tests or urinalysis were normal throughout the study.
Baseline airways responses
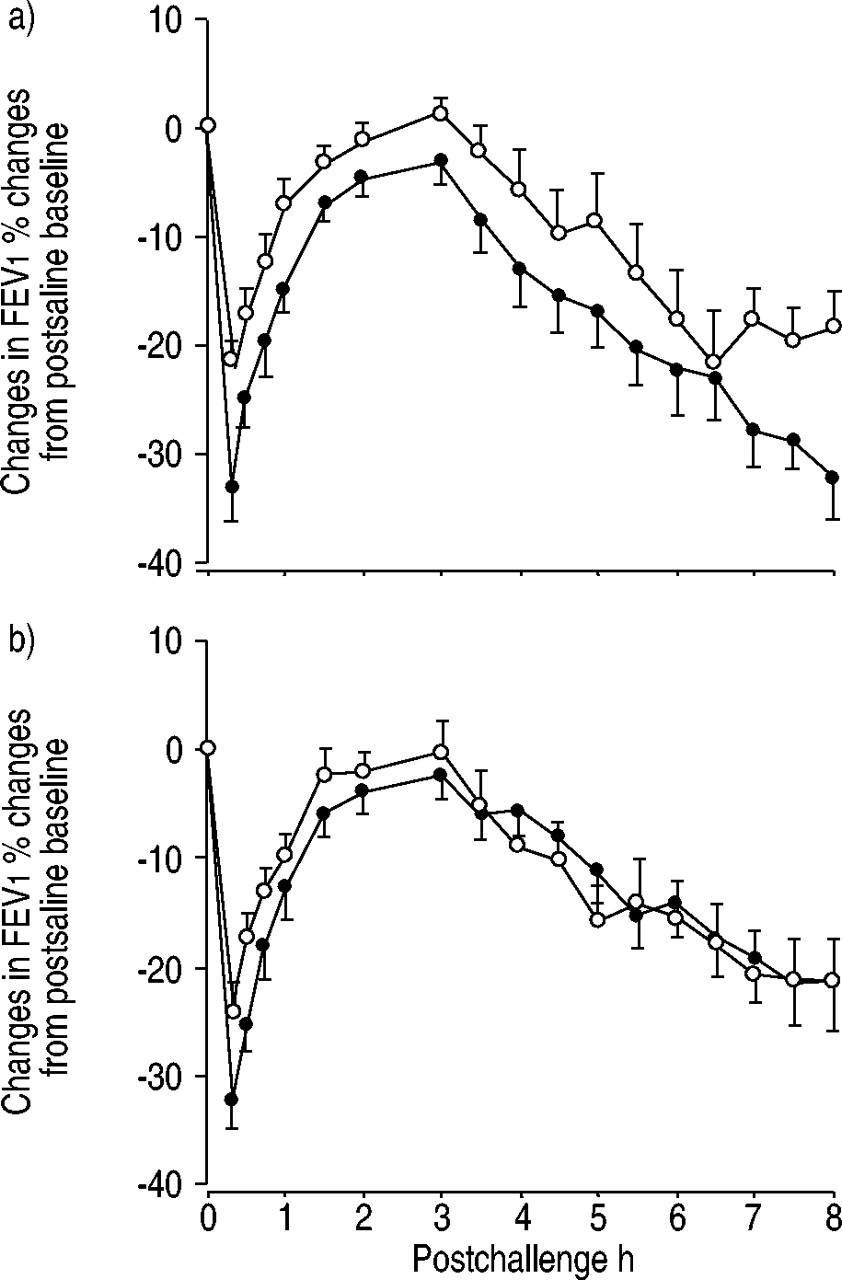
At baseline, all the subjects developed both an EAR and LAR. The mean (range) maximum percentage falls during the EAR were 33% (20.6–50.6) and 33% (20.6–42.7) in the SRL172 and placebo groups, respectively. During the LAR, the mean (range) maximum percentage FEV1 fall was 35.8% (16.5–66.7) in subjects receiving SRL172 and 29.5% (16.9–39.4%) in subjects receiving placebo (fig. 2⇓).

Effects of a) Mycobacterium vaccae (SRL172) and b) placebo on allergen-induced airway responses. •: pretreatment; ○: post-treatment. The maximum fall in forced expiratory volume in one second (FEV1) and the area under the curve of the FEV1 changes during the late asthmatic response were significantly reduced after treatment with SRL172 (p=0.005 and p=0.02, respectively) but not after placebo.
Baseline geometric mean (range) PC20 histamine, although lower in the subjects treated with SRL172 (1.17 mg·mL−1 (0.65–2.69 mg·mL−1)) when compared with those receiving placebo (1.82 mg·mL−1 (0.35–13.49 mg·mL−1)), was not significantly different (p=0.23).
Effects of treatment on airway responses to allergen challenge
Treatment with placebo or SRL172 had no significant effect on the EAR either in terms of the maximum percentage falls in FEV1 or AUC. However, treatment with SRL172 caused a significant (p=0.005) reduction in the maximum fall in FEV1 during the LAR from a mean (range) of 35.8% (16.5–66.7) before treatment to 26.7% (3.6–60.6) after injection of SRL172, a mean relative reduction of 25.4% (fig. 3⇓).
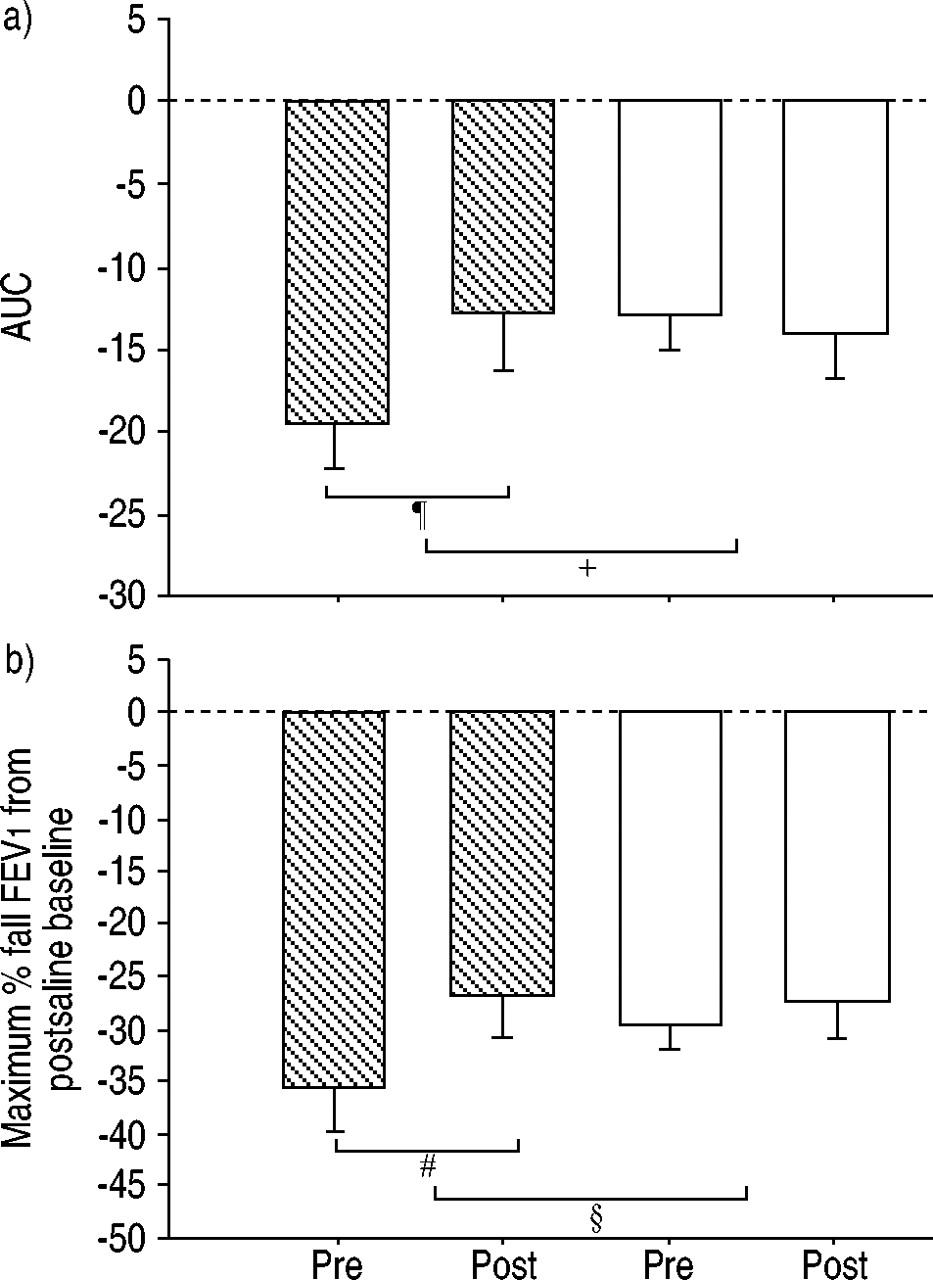
Effects of Mycobacterium vaccae (SRL172) on a) the area under the curve (AUC) and b) the maximum fall in forced expiratory volume in one second (FEV1) during allergen-induced late phase asthmatic responses. ┘: SRL172; □: placebo. The AUC was calculated by trapezoid integration of the area between the curve and the x-axis, taking 3–8 h as the period of analysis. #: p=0.005; ¶: p=0.002; +: p=0.06; §: p>0.1. The p-values of 0.06 and 0.1 denote levels of significance when comparing the two groups with respect to the changes in AUC and maximum fall in FEV1, respectively.
Similarly, the AUC of the percentage fall in FEV1 was reduced significantly (p=0.02) from 19.4% (5.8–41.4) to 12.8% (0.4–39.1), a mean relative reduction of 34%. In contrast, in the subjects receiving placebo there was no significant change in either the maximum percentage fall in FEV1 or AUC of the LAR. When comparing the magnitude of changes in the groups of subjects receiving SRL172 and those receiving placebo by ANOVA, the effect on the AUC during the LAR failed to reach the conventional 5% significance level (p=0.06), and the effect on the maximum percentage fall in FEV1 was not significant.
Effect of treatment on airway responsiveness
The two groups of subjects were not different in respect of baseline PC20 histamine. Allergen challenge performed before any treatment caused a significant (p=0.007) change in PC20 from a geometric mean (range) of 1.17 mg·mL−1 (0.64–-2.72 mg·mL−1) to 0.55 mg·mL−1 (0.1–1.68 mg·mL−1) in the subjects that subsequently received SRL172 and a significant change (p=0.02) from 1.81 mg·mL−1 (0.35–13.63 mg·mL−1) to 0.78 mg·mL−1 (0.16–8.84 mg·mL−1) in the subjects that received placebo. The changes in PC20 between the two treatment groups were not significantly different (p=0.98). Comparisons of the geometric means for postallergen challenge PC20 recorded before and after treatment with placebo or SRL172 using ANOVA showed no difference between the two treatment arms, with the mean value changing from 0.55 mg·mL−1 to 0.76 mg·mL−1 in the actively treated subjects and from 0.77 to 1.41 mg·mL−1 in the subjects receiving placebo.
Effect of treatment on IL-5 synthesis in vitro and serum IgE levels
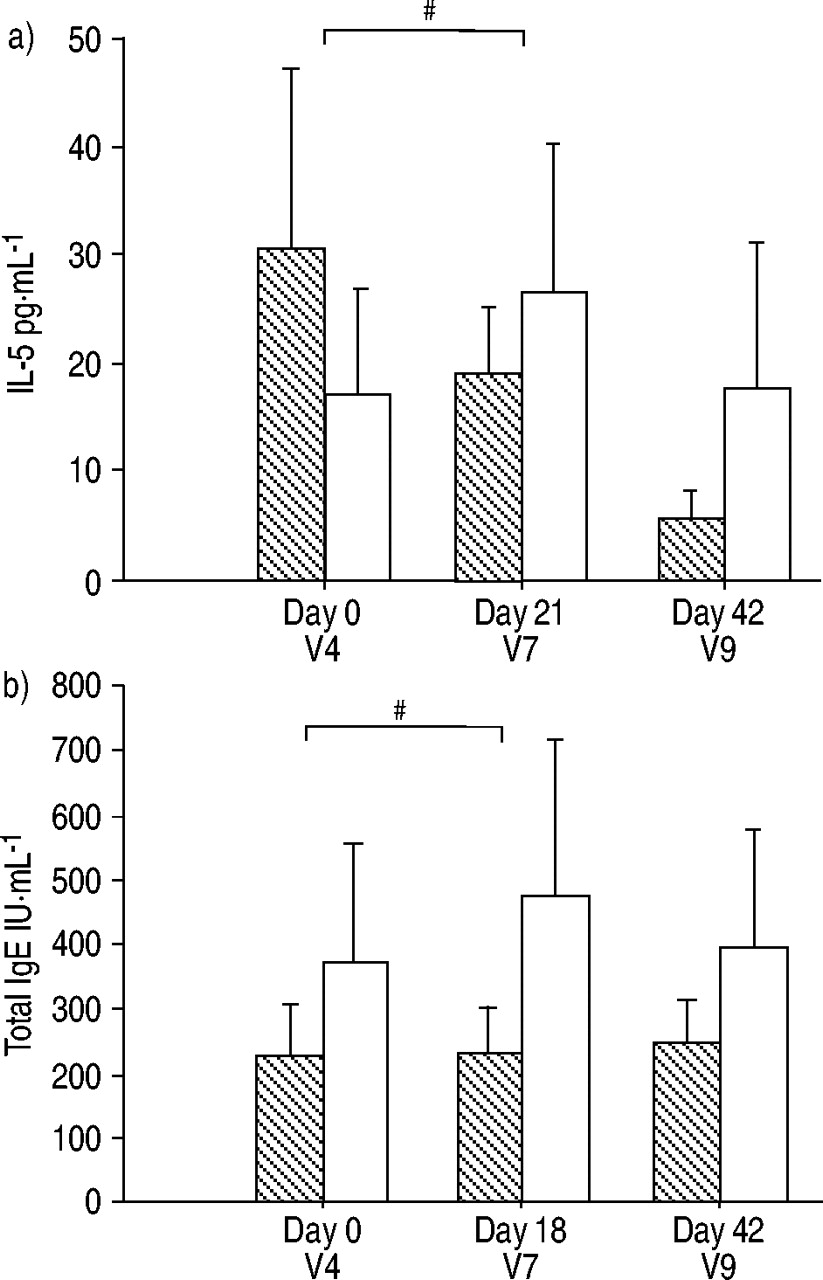
Cultures of PBMC were performed on all three occasions in 19 subjects (10 treated with SRL172 and nine subjects receiving placebo). Subjects who were randomised to receive active treatment had a tendency to exhibit higher IL-5 responses to allergen in vitro, but these were not significantly different from subjects receiving placebo (fig. 4⇓).
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Effects of Mycobacterium vaccae (SRL172) on allergen-induced a) interleukin (IL)-5 generation by peripheral blood mononuclear cells and b) total serum immunoglobulin (Ig)E levels during the study. V: visit. ┘: SRL172; □: placebo. #: p=0.07. The p-values indicate significance levels when comparing the changes in IL-5 and IgE concentrations in the SRL172 group with those in the placebo group that had occurred between day 0 and day 21 using the Fisher's exact test.
In seven out of 10 subjects treated with SRL172 there was a gradual decline in IL-5 synthesis over the course of the study. In contrast, there was a decrease in IL-5 in only two subjects receiving placebo. In the latter group, there was a tendency towards a transient increase at visit 7, i.e. just before the second allergen challenge, which was followed by a return to baseline levels at the end of the study. Comparisons by Mann-Whitney U-test of AUC of IL-5 changes that had occurred between visits 4 and the subsequent visits showed a tendency towards significant differences (p=0.07 for differences in AUC between visit 4 and 7 and 0.08 for the whole time course, i.e. between visits 4 and 9). Comparison of the changes in IL-5 and IgE concentrations in the SRL172 group with those in the placebo group that had occurred between visits 4 and 7 using the Fisher's exact test also showed a tendency for significant differences (p=0.07). Similar trends were seen for total serum IgE levels when comparing placebo and SRL172 treatment groups (p=0.07 when comparing visits 4 and 7 by Fisher's exact test; fig. 4⇑). Comparison of AUC showed no difference between the two treatment groups.
Discussion
This study has shown that a single intradermal injection of SRL172 in allergic asthmatics has a small effect on the allergen-induced LAR, which is associated with a tendency for reduced IL-5 synthesis by T-cells stimulated with allergen in vitro. Although the difference between active treatment and placebo failed to reach conventionally accepted 95% significance levels (the p-value was 0.06), these findings suggest that SRL172 may have the potential to modulate both the airways reaction to specific allergens and the associated upregulation of Th2-type cytokines that is typical of atopic asthma.
It was recognised that the comparison of the effects on airway responses of SRL172 with those of placebo failed to reach the significance levels usually sought in clinical trials. However, the high significance of the comparisons of both the maximum fall in FEV1 and the AUC of the LAR within the group of subjects treated with SRL172 suggests that M. vaccae has effects that deserve further study.
One difficulty with the design of this study has been the lack of sufficient knowledge about the therapeutic dose and time-course of action of SRL172. The dose of SRL172 was selected as the largest dose used in humans, giving a Th1 pattern of response to mycobacterial antigen that did not cause unacceptable local inflammation. The timing of the challenge in relation to the injection of SRL172 was based on the attenuating effect of SRL172 in the murine ovalbumin-sensitised mouse seen 3 weeks after administration of M. vaccae 17. However, recent evidence suggests that 3 weeks was too soon to seek maximal effect 21. It is also possible that the immunomodulatory capacity of SRL172 varies considerably from mildly to highly allergic individuals. Therefore, a greater degree of confidence in the biological effect might have been seen in the present study if more subjects had been included to take into account this variability. Finally, it is also possible that a greater effect may have been observed with multiple injections.
While it can be accepted that a different study design could have shown a better inhibitory effect, it is still a fact that the clear efficacy of M. vaccae seen in animal models has not yet been reproduced in human asthma. In the ovalbumin-sensitised mouse model, M. vaccae dramatically reduces serum IgE and IL-5 release from the spleen 17 as well as blood and lung eosinophilia and bronchial hyperresponsiveness 18, 22, 23. Critically, these inhibitory effects can be passed onto nonimmunised animals using passive transfer of regulatory T-cells 18. The greater efficacy in animal models could have several explanations. It may be that M. vaccae is more potent at preventing sensitisation, which would explain the efficacy in animal models or inhibiting inflammatory changes caused by intermittent allergen exposure. The latter explanation finds support in a recent study showing that intradermal administration of SRL172 can reduce the requirement for bronchodilators in mild pollen-induced seasonal asthma 24. A further explanation may be that SRL172 is more effective in conditions that are strongly dependent on atopy. Consistent with this is the finding that SRL172 markedly reduced the intensity of atopic dermatitis in children 25. The most plausible explanation for the relatively small effects in the current study may be that higher and/or more frequent doses have to be given for greater efficacy. A study by Shirtcliffe et al. 21, using half the dose applied in the current study and a different strain of M. vaccae (ATCC 15483), failed to reach statistical significance with regard to the number of clinical asthma outcomes.
Following on from animal studies showing significant effects of M. vaccae on cytokine responses 17, 18, 22, 23, an exploratory study was conducted to seek evidence for effects on the Th2 cytokine IL-5 and IgE. Whilst this part of the study was not performed with the aim of providing a definitive answer, a trend towards a significant effect of a single injection of SRL172 to reduce the capacity of peripheral blood T-cells from allergic individuals to generate IL-5 in response to specific allergen was seen. In contrast to the transient rise in allergen-induced IL-5 synthesis in vitro that could be seen in subjects receiving placebo, there was a steady decline in IL-5 synthesis in seven out of 10 subjects treated with SRL172. This would suggest a protective effect against allergen exposure. In the absence of PBMC culture at the beginning of the study, i.e. before the first allergen challenge, there is no definitive explanation for the time-course of IL-5 synthesis and therefore, it was speculated that the transient rise in placebo-treated subjects was a consequence of the first allergen challenge, with the potential for IL-5 generation returning to baseline at the end of the study. By way of its effects on the maturation of eosinophils from bone marrow-derived precursors and their activation and prolonged survival in the affected organ, IL-5 is one of the key cytokines in allergic diseases. However, it is becoming apparent that IL-5 is not the only cytokine involved. Indeed, a recent clinical trial using a humanised anti-IL-5 antibody has shown no significant reduction in the LAR 26. It is therefore important to appreciate that unlike agents that target single mediators, M. vaccae has a wider effect through its ability to reduce both IL-4 and IL-5 17 and IL-13 (L. Rosa Brunet, SR Pharma, London, UK. personal communication) and to induce regulatory T-cells that downregulate Th2 via a mechanism involving IL-10 and T-cell growth factor (TGF)-β 18.
The results of this study also lend some support to the hygiene hypothesis. The strong negative association between delayed hypersensitivity to M. tuberculosis and atopic disease seen in Japanese children 9 and the increase in IgE levels following successful treatment of pulmonary tuberculosis in South Africa 27 suggest that immune responses to mycobacteria are an important means of inhibiting allergic responses. However, it should be appreciated that M. vaccae is unique in its ability to modulate immune responses. Its Th1 adjuvant property is unaffected by killing, whereas other mycobacteria, such as BCG, have little Th1 adjuvant effect when dead 28. M. vaccae also downregulates pre-existing Th2 responses in a manner that appears to be independent of its ability to enhance Th1 responses 17. This effect has now been attributed to induction of CD4+CD45RBlow regulatory T-cells that can suppress allergic inflammation and airway hyperreactivity when transferred to allergic recipients 18. The recent recognition of regulatory T-cells of this phenotype in human peripheral blood 29 suggests that further studies of the regulatory function of M. vaccae should be undertaken in human disease.
In conclusion, the results of this study provide some evidence that Mycobacterium vaccae (SRL172) may be able to modulate the way in which the airways and the immune system respond to allergenic stimuli. It is acknowledged that the findings from this study are not definitive, but the authors believe that they justify the need for further clinical trials involving multiple dosing to study the potential of SRL172 as a treatment for chronic asthma.
- Received May 22, 2002.
- Accepted September 22, 2002.
- © ERS Journals Ltd
References









