





Abstract
This study investigated whether patients developing pulmonary arterial hypertension (PAH) after exposure to the appetite suppressants fenfluramine and dexfenfluramine have mutations in the bone morphogenetic protein receptor 2 (BMPR2) gene, as reported in primary pulmonary hypertension.
BMPR2 was examined for mutations in 33 unrelated patients with sporadic PAH, and in two sisters with PAH, all of whom had taken fenfluramine derivatives, as well as in 130 normal controls. The PAH patients also underwent cardiac catheterisation and body mass determinations.
Three BMPR2 mutations predicting changes in the primary structure of the BMPR-II protein were found in three of the 33 unrelated patients (9%), and a fourth mutation was found in the two sisters. No BMPR2 mutations were identified in the 130 normal controls. This difference in frequency was statistically significant. Moreover, the mutation-positive patients had a somewhat shorter duration of fenfluramine exposure before illness than the mutation-negative patients, a difference that was statistically significant when the two sisters were included in the analysis.
In conclusion, the present authors have detected bone morphogenetic protein receptor 2 mutations that appear to be rare in the general population but may combine with exposure to fenfluramine derivatives to greatly increase the risk of developing severe pulmonary arterial hypertension.
This study was supported by grants from NIH-HBLI-60056, NIH-DK-31813, INSERM, AFM, and Université Paris-Sud. Z. Deng was supported by a PHA fellowship award.
Exposure to appetite suppressants aminorex, fenfluramine and dexfenfluramine are known risk factors for pulmonary arterial hypertension (PAH) 1. Increased risk for PAH was first reported in the late sixties with exposure to aminorex 2 and in the mid-nineties with fenfluramine or dexfenfluramine 3–5. However, the exact mechanism(s) by which fenfluramine derivatives promote PAH has not been established 6. Individual susceptibility factors are likely to play an important role since the absolute risk in the general population is thought to be low. For example, the proportion of individuals developing PAH among all individuals taking fenfluramine derivatives, has been estimated as ∼1 in 10,000 for overweight individuals exposed to fenfluramine derivatives for >12 months 3–5 (S. Rich, Rush Heart Institute Center for Pulmonary Heart Disease, Rush-Presbyterian-St. Luke's Medical Center, Chicago, IL, USA, personal communication). Presumably this proportion is even lower for individuals who have a shorter exposure to fenfluramine derivatives.
PAH can occur in individuals who have no known risk factors to develop this condition (primary pulmonary hypertension (PPH)). PPH is a rare condition, with a poor long-term outcome, despite recent therapeutic advances such as continuous intravenous epoprostenol and lung or heart/lung transplantation. Familial PPH (autosomal dominant inheritance with incomplete penetrance) maps to chromosome 2q33 7, 8. Mutations of the gene encoding bone morphogenetic receptor II (BMPR-II) were recently identified as the cause of some familial 9–11 and some sporadic PPH 12. BMPR-II is a cell-surface receptor belonging to the superfamily of receptors for ligands of the transforming growth factor (TGF)-β family 13. The observed missense, nonsense and frameshift mutations coding for BMPR2 were predicted to alter the bone morphogenetic protein and TGF-β1/SMAD signalling pathways, resulting in proliferation rather than apoptosis of vascular cells 9–14. In an effort to determine whether BMPR2 mutations are a risk factor for appetite suppressant-associated PAH, the gene was screened in 33 unrelated PAH patients and in two sisters with PAH, all 35 of whom had a history of fenfluramine or dexfenfluramine exposure, and in 130 normal controls. Both patients and controls were from France.
Methods
Patient selection
The study group consisted of 35 PAH patients who had taken the appetite-suppressant drugs fenfluramine, dexfenfluramine or both, and who subsequently developed symptomatic PAH. The study was approved by the Institutional Review Board of Columbia University and by Hôpital Antoine Béclère. The 33 unrelated cases and two affected sisters, referred between 1987 and 2000 for evaluation of pulmonary hypertension, were recruited from the Centre for Pulmonary Vascular Disease, Hôpital Antoine Béclère, France. The first sister was referred to the centre for severe PAH associated with fenfluramine derivatives, and her younger sister was hospitalised 2 yrs later, with the same diagnosis. Patients who had used only amphetamines were excluded, although four patients who used amphetamines concomitant with fenfluramines were included. Evaluation and work-up ruled out all other causes of pulmonary hypertension 1, 15. The controls consisted of an ethnically matched sample of 130 healthy blood donors collected in the same hospital in France.
Molecular methods
Genetic variation in both the coding sequence and the intron/exon boundaries of BMPR2 was assayed by denaturing high performance liquid chromatography (dHPLC) using a WAVE® Nucleic Acid Fragment Analysis System (Transgenomics, Inc., Omaha, NE, USA), as per the manufacturer's directions and as described previously 9, 16, 17. Polymerase chain reaction amplification products (max size=602 base pairs) were run with up to three melting profiles for fragments with multiple melting domains. In addition, deoxyribonucleic acid (DNA) sequence determination of all fragments (exons 1–13) from each individual, whether or not they contained potential variants, was performed by cycle sequencing using Big DyeTM terminators (Applied BioSystems (ABI), Inc., Foster City, CA, USA) and sequencing products were resolved and detected with an ABI Model 3100 DNA sequencer (ABI). The resulting DNA sequence traces were analysed using Vector NTI suite 6.0 (Informax Inc., Bethesda, MD, USA), as were the protein sequence alignments.
Statistical methods
Statistical analyses used Fisher's exact test and the nonparametric Mann-Whitney U-test, as appropriate.
Results
Thirty-four of the 35 patients were female: 32 White, two Black, and one Indian. Their ages ranged from 18–70 yrs, mean age 50±13. Their body mass indices ranged 20–40, mean pulmonary artery pressures between 5.3–12.1 kPa (40–91 mmHg), cardiac indices between 1.15–4.28 L·min−1·m−2, and total pulmonary vascular resistance between 559–2504 dynes·sec·cm−5. Twenty-two patients took dexfenfluramine, 12 fenfluramine, and one used both drugs.
Four BMPR2 mutations that predict changes in the primary structure of the BMPR-II protein were found; three in the 33 unrelated patients (frequency 9%), and the fourth in the two sisters. The two sisters with familial BMPR2 mutations did not differ from the remaining patients in the series, in that symptomatic PAH developed only after the use of fenfluramine derivatives. One of the unrelated patients used dexfenfluramine for 5 months and had an A to C change in exon 2 at position 246. This DNA sequence change predicts a substitution in the primary amino acid sequence of the receptor from an uncharged glutamine to a positively charged histidine (Q82H) in the extracellular domain that is responsible for ligand binding and dimerisation. The second unrelated patient took fenfluramine for 2 months and had a change from G to A in exon 5 at position 545. This mutation predicts a protein sequence change of an uncharged glycine at position 182 to a negatively charged aspartic acid (G182D) in the kinase domain of the protein. The third unrelated patient took fenfluramine for 1 month and had a T to C mutation in exon 11 at position 1447. This mutation predicts a protein sequence change of an uncharged cysteine to a positively charged arginine (C483R). Of interest, the first two mutations change amino acids to ones that are invariant in a few of the other known BMPR-II receptors (figs 1⇓ and 2⇓), whereas the third mutation, involving an evolutionarily conserved amino acid, is not found in any of the known type-II receptors belonging to the TGF-β superfamily. The two affected sisters had a history of 1 and 2 months' dexfenfluramine exposure, respectively, before being diagnosed with PAH. They each had a stop codon 631C>T, resulting in a nonsense (R211X) mutation in exon 6 predicted to produce a truncated protein. These mutations were not observed in a sample of 260 ethnically matched chromosomes. The first two of these mutations have not been reported previously 9–12, and identical DNA mutations have been observed for the latter two in sporadic PPH (C483R) 12 and familial PPH (R211X) 11.
The difference in frequency of mutation between the studied patients and the 130 French controls was statistically significant, whether the two sisters were excluded (comparing 3 out of 33 versus 0 out of 130, p=0.015, Fisher's exact test, 2-sided), or whether they were counted as a single independent observation (4 of 34 versus 0 of 130, p=0.003). Moreover, none of these changes have been reported in 350 normal chromosomes in the literature 9–12.
The duration of anorexigen use had a median of 1 month in mutation-positive patients (range 1–5 months) and a median of 4 months in the mutation-negative patients (range 1–60 months, with one outlier of 180 months). Eight patients (four mutation-positive and four mutation-negative) had an exposure of <3 months.
The patients with a mutated BMPR2 gene had similar clinical and haemodynamic characteristics when compared to the patients with no mutations, except that a shorter duration of exposure to fenfluramine derivatives was found in the patients with BMPR2 mutations. Two analyses were performed, comparing duration of exposure between the mutation-positive patients and the 30 mutation-negative ones: one comparing the durations themselves, and the other comparing the proportion of patients with <3 months versus ≥3 months exposure. Both analyses yielded statistically significant results if the two sisters were included as independent observations or if they were treated as a single observation with a duration of 1.5 months (table 1⇓).
Discussion
This study describes the first genetic mutations, namely in BMPR2, detected in individuals displaying PAH after exposure to fenfluramine derivatives. Two of the four mutations found here in the PAH patients with exposure to fenfluramine derivatives are new and have not been reported previously in any disease state 9–12. The mutations were rare, three mutations in BMPR2 in 33 unrelated patients with sporadic PAH (9%) and another mutation in two sisters with familial PAH. Two of the unrelated patients had missense mutations found to be invariant in all vertebrate nonhuman BMPR-type II receptors that have been sequenced, and in the case of the (Q82H) mutation, other members of the TGF-β type-II receptor superfamily as well (fig. 1⇓ and 2⇓). The Q82H mutation is also the first noncysteine amino acid substitution to be described in the ligand binding domain of BMPR2 9–12, however, the mutation does not appear to change the secondary structure of the region. The missense mutation in the third unrelated patient was not found in other BMPR-type II receptors and involved an evolutionally conserved amino acid. Both sisters had the same stop codon mutation and are predicted to produce a truncated protein that may act via the mechanism of haploinsufficiency. Unfortunately, there were no additional samples from family members of the three unrelated cases; therefore it was not possible to determine if the mutations arose de novo. Experiments are in progress to test the physiological implications of these mutations.
Moreover, a short exposure to fenfluramine derivatives may be sufficient to induce or accelerate the progression of the disease in certain BMPR2 mutation-positive individuals. Recently, PAH has been classified into unexplained pulmonary hypertension, or PPH and PAH of certain known aetiologies such as collagen vascular diseases, human immunodeficiency virus infection, portal hypertension, congenital systemic to pulmonary shunts and anorexigen exposure 1. The finding of BMPR2 mutations in anorexigen-induced PAH adds this predisposition to pulmonary vascular disease to that originally found in PPH 9–12, suggesting that gene mutations might provide a better classification of PAH.
The International Primary Pulmonary Hypertension Study found an association between appetite suppressants and PPH, with odds ratio (relative risk estimates) of 6.3 (95% confidence interval (CI) 3.0–13.2); 90% of cases for whom a defined product could be traced had used a fenfluramine derivative 3. The risk increased markedly with duration of use (relative risk estimate of 23.1 for >3 months, 95% CI 6.9–77.7) 3. However, some patients developed severe PAH even with short-term use of fenfluramine, emphasising the relevance of individual susceptibility to fenfluramines 3, 18. Similarly, the patients with BMPR2 mutations studied here appeared to have a shorter duration of exposure to fenfluramine derivatives when compared to patients without evidence of mutations.
Several unknowns prohibit a more thorough evaluation of the 9% frequency of BMPR2 mutations in PAH after fenfluramine derivatives observed here. First, the methods used here could have missed large deletions of BMPR2, and mutations in the promoter and large introns were not screened. Second, the frequency of BMPR2 mutations in the general population is unknown (however, based on the present authors' observation of no new BMPR2 mutations in 610 control chromosomes (the 260 normal chromosomes studied, plus the literature 9–12, plus another 350 French chromosomes determined here) the present authors can form an exact one-sided 95% CI of 0–0.0049, i.e. an upper 95% confidence limit of ∼1/200 for allele frequency, or ∼0.01 for carrier frequency, although the present authors surmise that the actual frequency is well below this (see Appendix)). Third, the penetrances of these mutations are unknown and may vary. The age of onset of disease both within families and between subjects carrying identical but recurrent mutations is variable. The previously reported large number of individuals nonpenetrant for the disease phenotype points to the potential requirement for additional factors, either environmental or genetic in the pathogenesis of the disease. Fourth, the distinction between sporadic and familial PPH can be hard to discern, as illustrated by the two sisters. The first sister was classified as having sporadic anorexigen associated PPH until the second sister developed the same disease. Unfortunately, the present study was unable to obtain additional family members from any of the BMPR2 mutation-positive individuals. In the sporadic cases this would help to determine if the observed mutations are de novo and in the family the observation of an individual with the mutation with no exposure to fenfluramine derivatives and no PAH would support the hypothesis that exposure is increasing the penetrance of these mutations. A greater understanding of the effects of appetite suppressant exposure in BMPR2 mutants will require an examination of a much larger sample of human chromosomes to determine their frequencies and the construction of transgenic animals with mutations for use in models of appetite suppressant-induced PAH.
The findings of the present study suggest there are additional mechanisms triggering the occurrence of the disease. Firstly, fenfluramines and aminorex inhibit potassium current flux in pulmonary vascular smooth muscle and may therefore stimulate pulmonary vasoconstriction 19. Secondly, it has been speculated that patients who develop pulmonary hypertension while taking an anorectic agent could have a pre-existing diminished nitric oxide activity 20. Such a defect has been demonstrated in a small series of patients displaying fenfluramine-associated PAH 20. Thirdly, poor metabolisers of fenfluramine derivatives may have a more pronounced exposure to the drug and could be more prone to develop the condition 21. Lastly, drug-induced alteration of the serotonin pathway might promote the occurrence of PAH 22, 23. By interacting with the serotonin transporter, fenfluramine derivatives release serotonin from platelets and inhibit its reuptake into platelets and pulmonary endothelial cells 22. As a consequence, the whole blood serotonin concentration increases with fenfluramine treatment 23. Serotonin is known to be a powerful pulmonary vasoconstrictor and can induce platelet aggregation 24. Moreover, serotonin is a growth factor for pulmonary smooth muscle cells 25. The possible relevance of the serotonin hypothesis in fenfluramine-induced PAH is supported by the fact that a decrease in platelet serotonin storage with enhanced blood concentration of free serotonin has been reported in sporadic cases of PPH, and fenfluramine derivatives induce valvular heart disease very similar to carcinoid syndrome 26–28.
Further investigations should determine whether abnormal transforming growth factor-β signalling alone, or in combination with other factors, plays a role in the occurrence of pulmonary hypertension associated with fenfluramine derivatives. However, it is becoming more apparent that the pathogenesis of pulmonary arterial hypertension is complex 29 and may sometimes require two hits, genetic and/or environmental, as has been found for neoplasia 30. The mutations detected in bone morphogenetic protein receptor 2 in the present study may be among the genetic “hits” needed to develop severe pulmonary arterial hypertension, particularly in combination with exposure to fenfluramine derivatives.
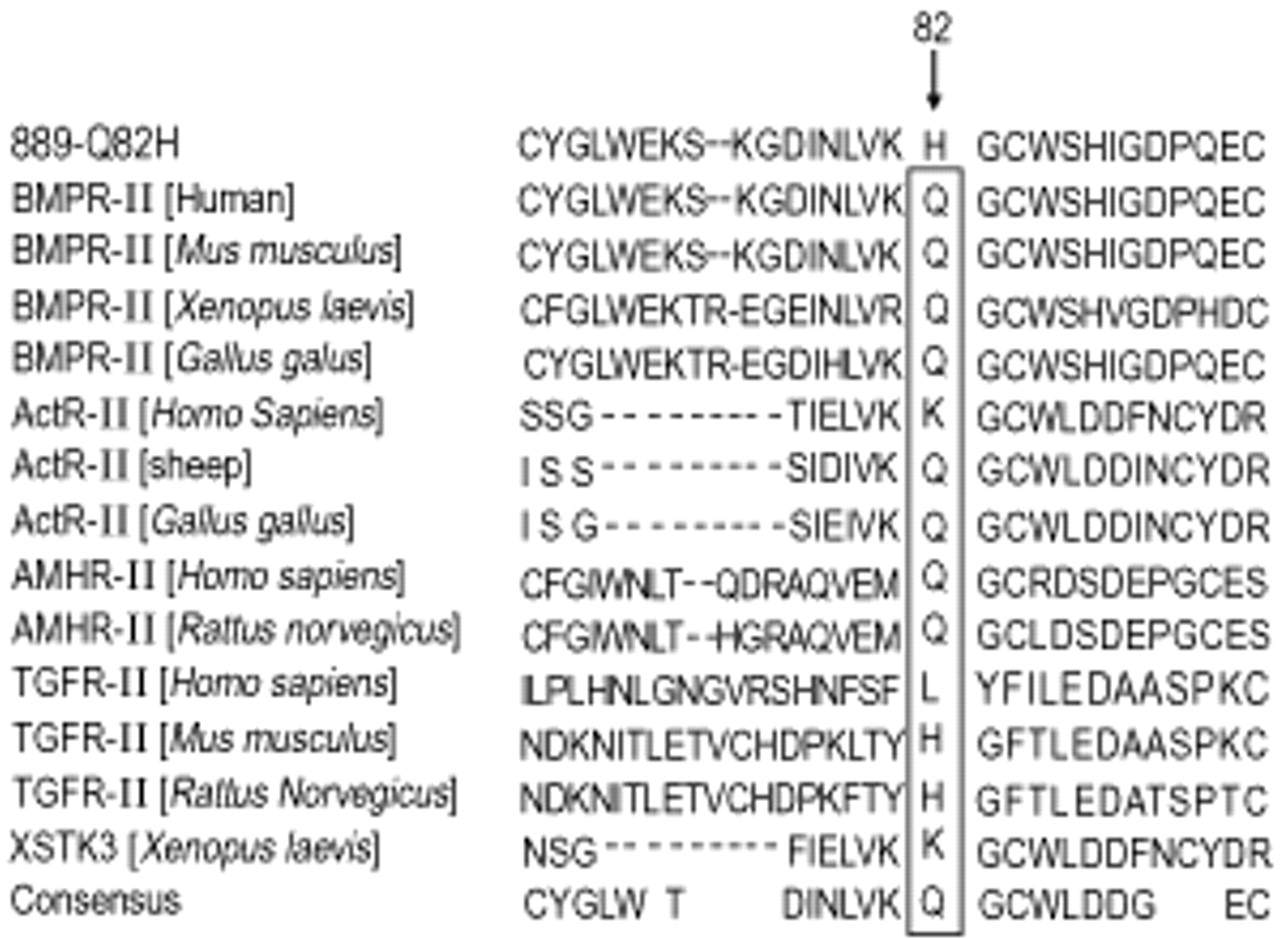
Sequence alignment of the type II transforming growth factor (TGF)-β-superfamily receptors surrounding Q82 in bone morphogenetic protein receptor 2 (BMPR-II). #889: patient with mutation; Act-R II: activin receptor type II; AMHR-II: anti-mullerian hormone type II receptor; TGFR-II: TGF-β type II receptor; XSTK3: Xenopus activin receptor.

{kind=link}
{kind=link}
Sequence alignment of the type II transforming growth factor (TGF)-β-superfamily receptors surrounding G182 in bone morphogenetic protein receptor 2 (BMPR-II). #1004: patient with mutation; AMHR-II: anti-mullerian hormone type II receptor; ActR-II: activin type II receptor; TGFR-II: TGF-β type II receptor; XSTK3: Xenopus activin receptor.
p-Values (two-sided) for analyses comparing duration of exposure between mutation-positive and mutation-negative patients
Appendix
To determine population carrier frequency (x) directly, one would have to test large numbers of control individuals for BMPR2 mutations, an expensive task. However, there is also an indirect approach that can estimate the lower bound of this frequency that can be used in the absence of a large amount of data: it can be shown that  where z is defined as the proportion of individuals who develop PAH, among all individuals taking fenfluramine derivatives; p is the proportion of mutation carriers, among affected individuals who were exposed to fenfluramine derivatives; and Pen (penetrance) is defined as the risk of developing PAH for individuals who carry one of the mutations and who have been exposed to appetite suppressants. (Mathematical details are not shown but are available from Dr. Hodge upon request.) The authors have an estimate of p=3/33=0.091 from the present study's data (not including the two sisters). It is known that Pen cannot >1.0, but actually, the authors anticipate it may be <0.3. Thus, if, for example, z were known to be 1 in 10,000 (see text), then carrier frequency x would have to equal at least 0.0000091=1/110,000 (based on Pen=100%), but could be as high as 1/22,000 or 1/11,000, if Pen were as low as 20% or 10%. Thus, it could be helpful to future investigators of PAH if a more precise estimate of z could be determined.
where z is defined as the proportion of individuals who develop PAH, among all individuals taking fenfluramine derivatives; p is the proportion of mutation carriers, among affected individuals who were exposed to fenfluramine derivatives; and Pen (penetrance) is defined as the risk of developing PAH for individuals who carry one of the mutations and who have been exposed to appetite suppressants. (Mathematical details are not shown but are available from Dr. Hodge upon request.) The authors have an estimate of p=3/33=0.091 from the present study's data (not including the two sisters). It is known that Pen cannot >1.0, but actually, the authors anticipate it may be <0.3. Thus, if, for example, z were known to be 1 in 10,000 (see text), then carrier frequency x would have to equal at least 0.0000091=1/110,000 (based on Pen=100%), but could be as high as 1/22,000 or 1/11,000, if Pen were as low as 20% or 10%. Thus, it could be helpful to future investigators of PAH if a more precise estimate of z could be determined.
Acknowledgments
The authors are indebted to S. Rich, for aiding their understanding of the risk of pulmonary arterial hypertension in those taking fenfluramine derivatives and to Y. Enson for his cogent suggestions.
- Received March 1, 2002.
- Accepted May 22, 2002.
- © ERS Journals Ltd
References









