





Abstract
Carcinoma of the bronchus is the most common malignancy in the Western world. It is also the leading cause of cancer-related death accounting for 32% of all cancer deaths in males and 25% in females 1. In the USA it causes more deaths than cancers of the colon, breast and prostate combined 2. Disappointingly, in a recent UK survey of improvements in cancer survival 3, carcinoma of the bronchus showed the smallest percentage reduction in the number of deaths avoided between 1981–1990 (0.2%). This compares badly with breast (11% reduction) and melanoma (32%). The overall 5‐yr survival for lung cancer diagnosed between 1986–1990 was only 5.3% (against 66% for breast and 76% for melanoma). It is on this background that the radiologist remains actively employed in the detection, diagnosis, staging and review of this common malignancy.
- bronchial carcinoma
- computed tomography
- diagnostic imaging
- magnetic resonance imaging
- positron emission tomography
- staging
Lung cancer, in theory, should lend itself to screening. The disease is very common and in its earliest stages ≤70% of cases can be cured by surgery 4. Despite this, lung cancer has an overall prognosis so dismal that incidence exceeds prevalence 5. The main risk factor, smoking, is easily identifiable and noninvasive screening tests such as chest radiography and sputum cytology are widely available.
Why is screening not performed? Three large American screening programmes in the 1970s sponsored by the National Institute of Health 6–9 and another in Czechoslovakia in the 1980s 10 screened high-risk populations using chest radiography and sputum analysis. All showed increased detection of early-stage lung cancer, more resectable cancers and improved 5‐yr survival rates in the screened versus control groups. Critically, however, none showed a statistically significant reduction in overall mortality.
In the last 5 yrs three nonrandomized trials incorporating low-dose computed tomography (CT) have reported prevalence screening data 11–13. Their findings are summarized in (table 1⇓). Also included in the table is preliminary data from two ongoing trials in the USA and Germany. These trials show that CT detects many more lung nodules than chest radiography. However, only a small percentage of these nodules turn out to be lung cancer. In the Mayo Clinic trial 7 for example, over one-half of all patients had at least one nodule. The logistics of differentiating benign from malignant nodules therefore becomes a very real issue and there have been concerns about the number of biopsies that may need to be performed. However, by assessment of patterns of calcification at both low-dose and high-resolution CT (HRCT) and repeat scanning after an interval, the Early Lung Cancer Action Project (ELCAP) group had only one incidence of biopsy performed for a benign, noncalcified nodule 11. In this study, the cancer detection rate was 2.7% but it was <0.5% for the two other published studies (table 1⇓). Although this seems low, it should be remembered that breast-cancer screening has a detection rate of only 0.6–0.7% 14.
The importance of rigorous study design cannot be overemphasized when assessing the validity of these large and expensive trials. Although survival from the time of diagnosis of the disease is commonly reported it is not an appropriate measure of a diagnostic screening test and may be misleading as it is subject to lead-time bias, length-time bias and overdiagnosis bias. Change in mortality rather than survival is necessary to validate such screening methods 2. Although low-dose CT can detect early stage disease 6–10 times more frequently than chest radiography 11, 15, there has not as yet been a similar fall in the prevalence of advanced disease 2. This lack of so-called “stage shift” again questions the ability of low-dose CT screening to decrease overall mortality. Cross-contamination between the screened and control arms of the study is also a problem in these large trials, especially as the public at large become more aware of health issues. Individuals in the control-arm trials may worry that they are missing out on optimal treatment and manoeuvre their way into the screened population.
In an attempt to overcome these various difficulties, groups sponsored by the Medical Research Council in the UK and the National Cancer Institute in the USA are currently piloting prospective, randomized, controlled trials of 40,000 and 88,000 patients respectively using low-dose CT. The latter should have the power to detect a 20% reduction in mortality 2.
Radiological characteristics by cell type
Adenocarcinoma
Adenocarcinoma represents 31% of all lung cancers, including bronchoalveolar carcinoma 16. Adenocarcinomas are typically peripherally located and measure <4 cm in diameter 17; only 4% show cavitation 18. Hila or hila and mediastinal involvement is seen in 51% of cases on chest radiography 19 and a recent study describes two characteristic appearances on CT: either a localized ground glass opacity which grows slowly (doubling time >1 yr) or a solid mass which grows more rapidly (doubling time <1 yr) 20.
Bronchoalveolar carcinoma
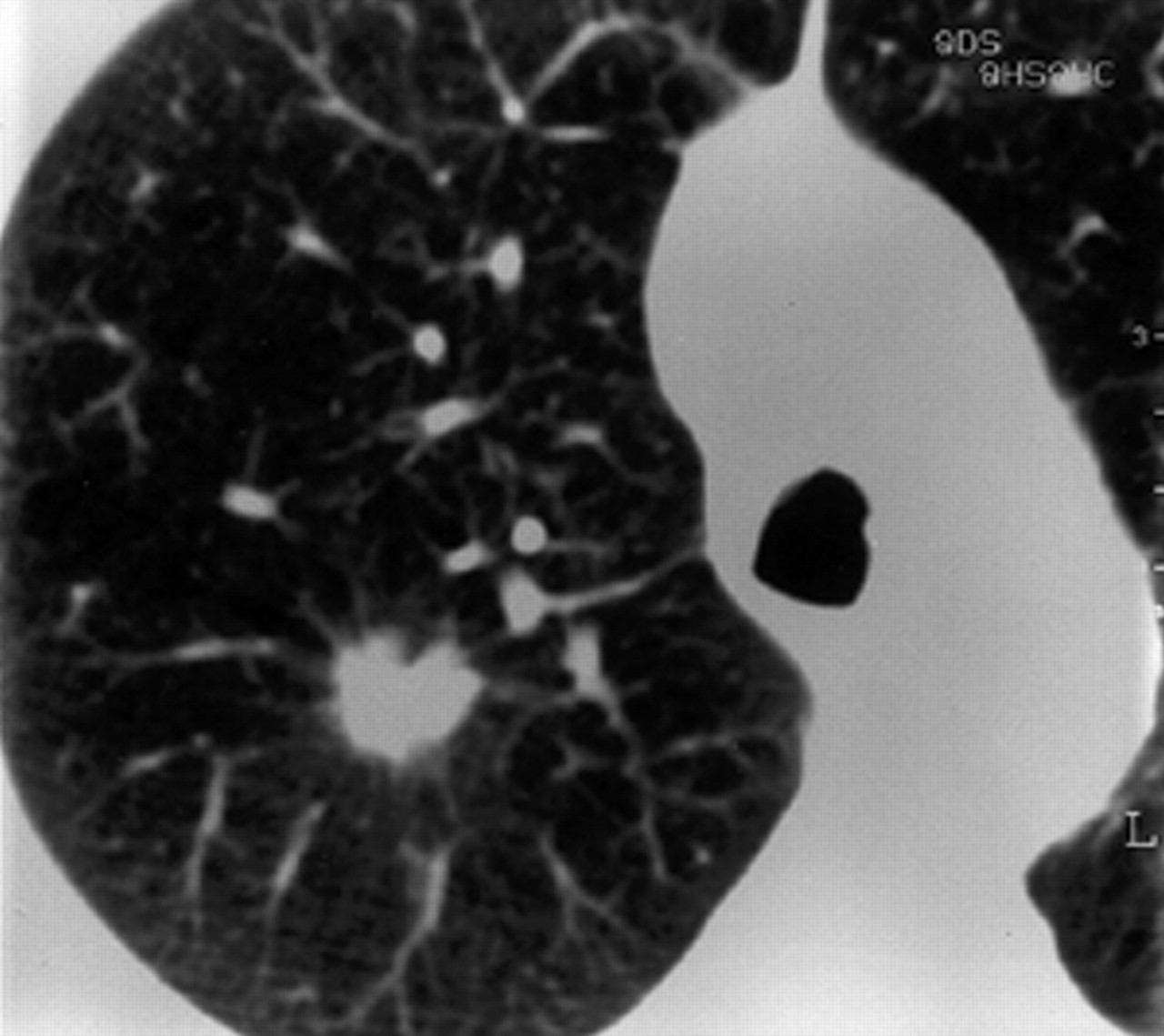
This is regarded as a subtype of adenocarcinoma and represents 2–10% of all primary lung cancers. There are three characteristic presentations: most common is a single pulmonary nodule or mass in 41%; in 36% there may be multicentric or diffuse disease; finally, in 22% there is a localized area of parenchymal consolidation 21. Bubble-like areas of low attenuation within the mass (fig. 1⇓) are a characteristic finding on CT 22. Hilar and mediastinal lymphadenopathy is uncommon 23. Persistent peripheral consolidation with associated nodules in the same lobe or in other lobes should raise the possibility of bronchoalveolar carcinoma 24.
Adenosquamous carcinoma
Adenosquamous carcinoma represents 2% of all lung cancers 16. This cell type is typically identified as a solitary, peripheral nodule. Over one-half are 1–3 cm in size and cavitation is seen in 13%. Evidence of parenchymal scars or fibrosis in or next to the tumour is seen in 50% 25.
Squamous cell carcinoma
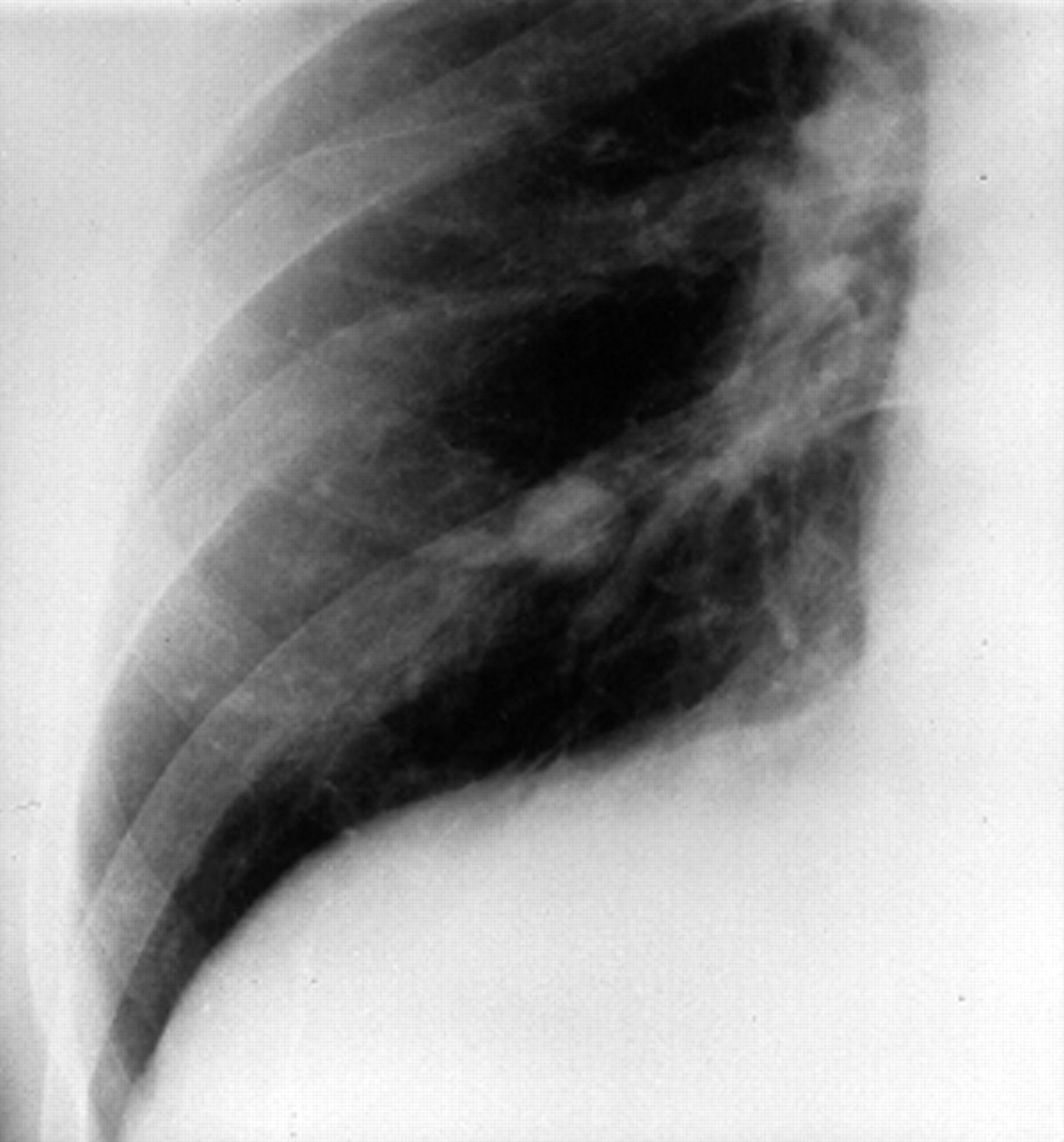
Squamous cell carcinoma represents 30% of all lung cancers 16. These tumours are more often centrally located within the lung and may grow much larger than 4 cm in diameter 17. Cavitation (fig. 2⇓) is seen in up to 82% 18. They commonly cause segmental or lobar lung collapse due to their central location and relative frequency 26.
Small cell lung cancer
Small cell lung cancer (SCLC) represents 18% of all lung cancers 16. SCLC often present with bulky hila and mediastinal lymph node masses (fig. 3⇓) 27, 28. A noncontiguous parenchymal mass can be identified in up to 41% at CT 28 that very rarely cavitates 18. They form the malignant end of a spectrum of neuroendocrine lung carcinomas with typical carcinoid tumours being at the more benign end 27. A mass in or adjacent to the hilum is characteristic of SCLC and the tumour may well show mediastinal invasion 17.
Carcinoid tumour
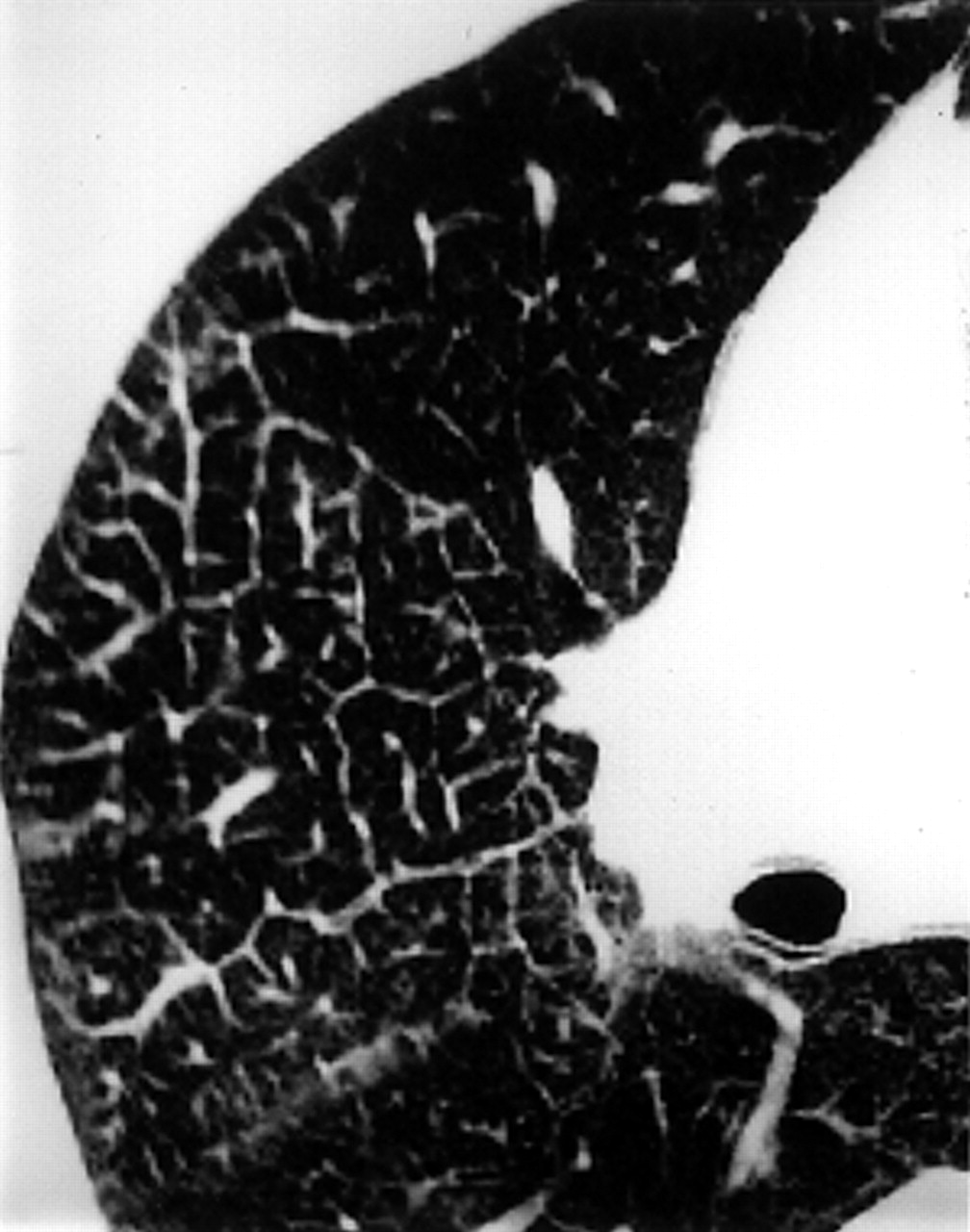
Carcinoid tumour represents 1% of all lung cancers 16. Atypical carcinoid tumours tend to be larger (typically >2.5 cm at CT) with typical carcinoid tumours being more often associated with endobronchial growth (fig. 4⇓) and obstructive pneumonia 27. Carcinoids tend to be centrally rather than peripherally located and calcification is seen in 26–33% 29. The 5‐yr survival for typical carcinoids is 95% against 57–66% for atypical carcinoids 29.
Large cell carcinoma
Large cell carcinoma represents 9% of all lung cancers 16. Large or giant cell carcinoma is a poorly differentiated nonsmall cell carcinoma (NSCLC) and is diagnosed histologically after exclusion of adenocarcinomatous or squamous differentiation 16. It may grow extremely rapidly 30 to a large size but metastasizes early to the mediastinum and brain 31.
It should be noted that there seems to be a change occurring in the prevalence of the described histological subtypes. Two large recent trials have reported prevalences for adenocarcinoma of 78% and 58% whilst squamous cell carcinomas accounted for only 4% and 11% respectively 11, 13.
Imaging techniques
Chest radiography
Due to its widespread availability, including to primary care physicians, the chest radiograph is often the first imaging modality to suggest the diagnosis of bronchogenic carcinoma. Lung cancer may present as a straightforward spiculated mass but its presence may also be inferred from other appearances such as an unresolving pneumonia or lobar collapse (fig. 5⇓). In some situations, no further imaging will be necessary when bulky contralateral mediastinal adenopathy is present or when an obvious bony lesion is identified. However, CT scanning of the chest is often needed because of the lack of sensitivity of the chest radiographs in detecting mediastinal lymph node metastases and chest wall and mediastinal invasion 32.
Computed tomography
CT can identify specific features in lung nodules that are diagnostic, e.g. arteriovenous fistulae, rounded atelectasis, fungus balls, mucoid impaction and infarcts. High-resolution scanning further refines this diagnostic process 33. The ability of CT scanning to evaluate the entire thorax at the time of nodule assessment is of further benefit.
Spiral or helical CT is advantageous as small nodules are not missed between slices as may happen on older, nonspiral machines. It also increases the detection rate of nodules <5 mm in diameter, especially when viewed in cine-format on a workstation 34, 35. The acquisition of continuous volume data sets permits three-dimensional image reconstruction and multiplanar (i.e. nonaxial) reformatting (fig. 6⇓). These techniques have been shown to improve the detection of pleural invasion by tumour and clarify the origin of peridiaphragmatic tumours respectively 36, 37. Further manipulation of raw data sets enables the technique of virtual bronchoscopy. An interactive, simulated bronchoscopy can be performed with the added benefit of simultaneous information on adjacent mediastinal structures. This technique has far reaching potential both as a teaching tool and as a means of evaluating patients' thoracic and bronchial anatomy prior to interventional procedures and stent placement 38.
The recent advent of multislice scanners has seen advances in image resolution with a substantial reduction in both tube loading and scanning time as up to four slices can be acquired simultaneously 39, 40. Both spiral and multislice machines suffer less from respiratory motion artefact due to their shorter scanning times.
Spiral CT with a bolus injection of intravenous iodinated contrast medium affords “dynamic scanning”. A recent study of 84 patients with NSCLC found no difference in radiological stage when noncontrast enhanced scans were compared with contrast enhanced scans in 80 patients (95%), recommending that nonenhanced CT through the thorax and adrenals was sufficient for staging patients with newly diagnosed NSCLC 41. However, another study of 50 patients comparing both techniques found an 11% higher detection rate of enlarged mediastinal nodes after contrast enhancement and recommended its routine administration (figs. 7 and 8⇓⇓) 42. Many centres perform hepatic and adrenal scans having given intravenous contrast.
Slice thickness and interval should be ≤10 mm and extend from the lung apices to the adrenal glands 16. It is now common practice to perform 5‐mm slices through the hila and aortopulmonary regions to improve delineation of local lymph nodes and the origins of the lobar bronchi. The field of view should include the contiguous chest wall 16.
Magnetic resonance imaging
Magnetic resonance imaging (MRI) is becoming more available but pressure on MRI scanning time is so intense that it is usually used for problem solving and where administration of contrast media is contraindicated. MRI can be more accurate than CT in separating stage IIIa (resectable) from IIIb (generally unresectable) tumours in selected patients due to its ability to detect invasion of major mediastinal structures, i.e. T4 disease 43.
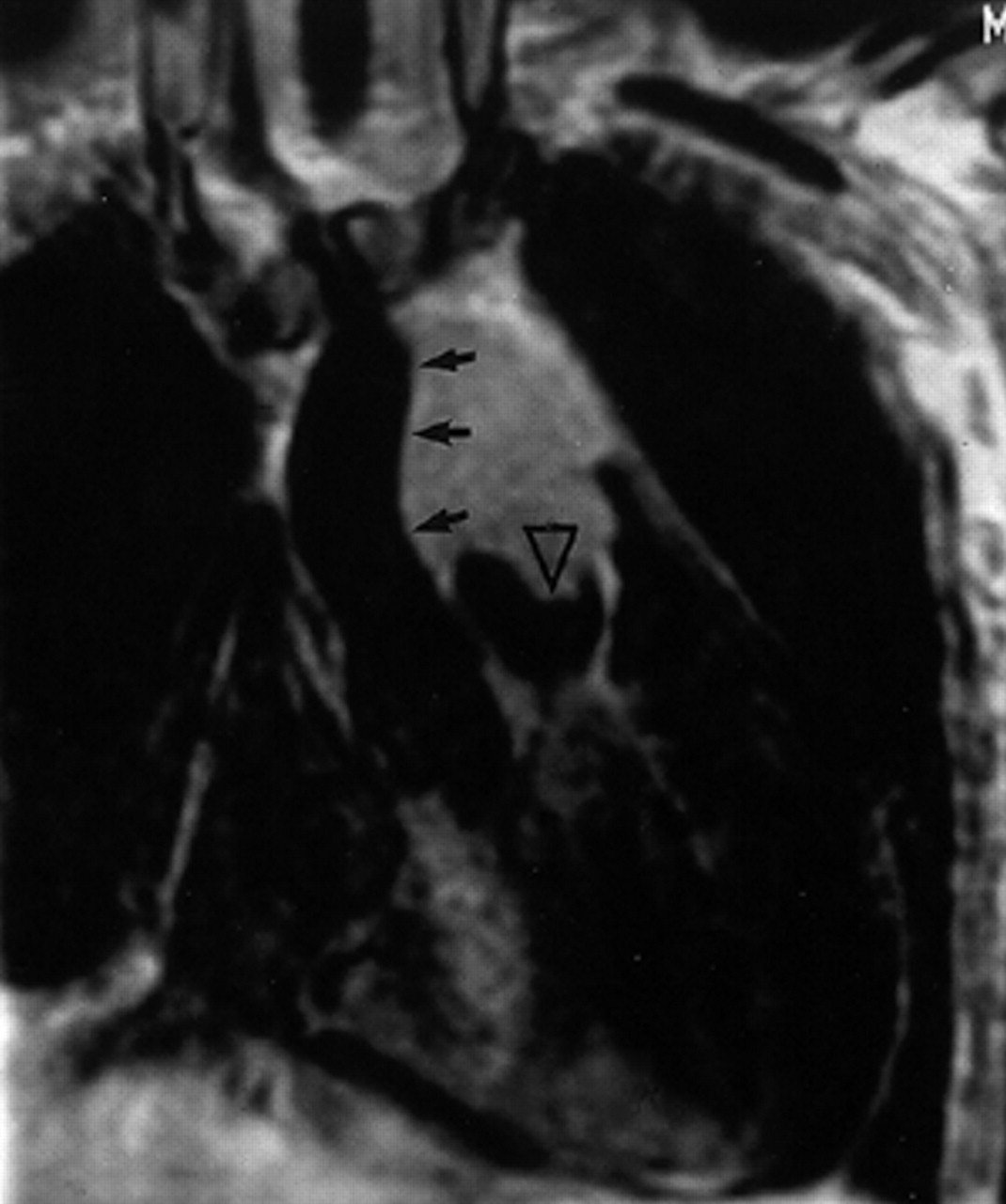
The advantages MRI has over CT include: better soft tissue contrast, multiplanar imaging capability, and therefore useful for superior sulcus tumours and evaluation of the aortopulmonary window (fig. 9⇓), and cardiac gating which enables excellent delineation of the heart and great vessels and removes cardiac pulsation artefact 44, 45.
MRI is also useful in the assessment of mediastinal and chest wall invasion by virtue of its ability to determine fat-stripe invasion (fig. 10⇓) and involvement of the diaphragm and spinal canal. In addition, it has been shown to aid in differentiating lymph nodes from hila vessels due to the “flow void” phenomenon 46, 47.
MRI has disadvantages compared to CT, being slower and more expensive with poorer spatial resolution and providing limited lung parenchyma information. MRI can overestimate lymph node size because of respiratory movement, causing the blurring together of discrete nodes into a larger, conglomerate mass 44. MRI is also poorly tolerated by claustrophobic patients and is contra-indicated in patients with indwelling electromagnetic devices and some prosthetic heart valves.
T1‐weighted sequences are used for the visualization of fat planes and improved spatial resolution. T2‐weighted sequences are useful for detection of high-signal tumour infiltration. Gadolinium enhancement can further enhance the diagnostic yield 48.
Positron emission tomography
Positron emission tomography (PET) scanning is a new imaging modality whose role in the assessment of lung cancer is still being determined. Its advantage over other modalities lies in its sensitivity in detecting malignancy and its ability to image the entire body in one examination.
PET is a physiological imaging technique that uses radiopharmaceuticals produced by labelling metabolic markers such as amino acids or glucose with positron-emitting radio nuclides such as fluorine‐18. The radiomarker is then imaged by coincidence detection of two 511 KeV photons that are produced by annihilation of the emitted positrons. The radiopharmaceutical, 18F‐2‐deoxy‐d‐glucose (FDG) is ideally suited for tumour imaging. PET performed with this agent exploits the differences in glucose metabolism between normal and neoplastic cells, allowing accurate, noninvasive differentiation of benign versus malignant abnormalities 49. Uptake of FDG is known to be proportional to tumour aggressiveness and growth rates 50. FDG uptake can be assessed visually on PET images (fig. 11⇓) by comparing the activity of the lesion with the background or by semiquantitative analysis using calculated standardized uptake ratios. An uptake ratio of <2.5 is considered indicative of a benign lesion 51, 52.
PET scanning detects malignancy in focal pulmonary opacities with a sensitivity of 96%, specificity of 88% and an accuracy of 94% in lesions of ≥10 mm 53–58. However, compared to CT, PET has poorer spatial resolution, which precludes it from accurate anatomical assessment of primary tumour status 59. False-positive PET findings in the lung are seen in tuberculous infection, histoplasmosis and rheumatoid lung disease. False negatives are seen with carcinoid tumours, bronchoalveolar carcinoma and lesions <10 mm in size 58–61.
PET is more accurate than CT in the detection or exclusion of mediastinal nodal metastases: sensitivities are 67–100% and 50–63% respectively whilst specificities are 81–100% and 59–94% 62–65. PET has been shown to correctly increase or decrease nodal staging as initially determined by CT in 21% of presurgical patients 66. In a study of 50 patients where PET and CT findings were reported jointly, the sensitivity rose to 93%, specificity 97% and accuracy 96% in the detection of mediastinal nodal disease 63. PET has been shown to detect occult extrathoracic metastases in 11–14% of patients selected for curative resection and alter management in up to 40% of cases 66–68.
In a recent study of 100 patients comparing whole body PET with conventional imaging (thoracic CT, bone scintigraphy, and brain CT or MRI) in staging bronchogenic carcinoma PET accurately staged NSCLC in 83% of cases when compared with pathological stage 69. The figure for conventional imaging was 65%. PET identified nine patients with metastases that were missed on conventional imaging whilst 10% of patients suspected of having metastases conventionally, were shown not to have by PET. PET was more sensitive and specific than bone scintigraphy for the detection of bone metastases and had a 100% positive predictive value for the presence of adrenal deposits as against 43% for conventional imaging. The technique faired poorly in the detection of brain metastases (60% sensitivity) prompting the authors to recommend the continued use of conventional imaging for routine staging of the brain. However, the negative predicative value of PET for N3 disease was identical to that of mediastinoscopy (96%) prompting the statement that patients with negative mediastinal PET findings could go directly to surgical resection of the primary lesion 69. This approach has been supported by other authors 59, 68. Positive PET findings however warrant nodal biopsy, as guided by the areas of increased FDG uptake, in order to exclude false positives. Causes include infection, inflammation, hyperplasia and sarcoidosis 59.
The main disadvantage for PET is the lack of availability and relatively high cost of each examination. However, decision analysis models indicate that combined use of CT and PET imaging for evaluating focal pulmonary lesions is the most cost-effective and useful strategy in determining patient management with a pretest likelihood of having a malignant nodule of 0.12–0.69 70.
PET is more accurate than conventional studies in detecting recurrent lung cancer and appears to be superior in distinguishing persistent or recurrent tumour from fibrotic scars 59, 71. However, false-positive studies do occur secondary to postirradiation inflammatory change and delaying the examination until 4 or 5 weeks postirradiation is recommended 72.
A recent study of 114 patients with solitary pulmonary nodules, ≤6 cm in diameter, highlighted the usefulness of single photon emission computed tomography using the 99mTechnetium-labelled somatostatin analogue, Depreotide 73. The sensitivity and specificity for this method in determining benign from malignant nodules was 97% and 73% respectively. These results are comparable with FDG‐PET imaging and can be performed using a standard gamma camera.
The solitary pulmonary nodule
Only 20% of carcinomas are resectable at diagnosis 74 and 50% of “coin lesions” on chest radiography are malignant: 40% representing primary lung cancers whilst the other 10% are solitary metastases 75. However, 20–30% of all cancers present as a solitary pulmonary nodule (SPN) of which 88% are resectable with a 5‐yr survival rate around 50% 74. The early identification and correct assessment of such nodules is therefore of the utmost importance.
Benign nodules
Chest radiography
A number of findings enable a nodule to be classed as benign on the basis of chest radiographical findings. 1) Age <35 yrs, no history of cigarette smoking and no history of extrathoracic malignancy 76. 2) Comparison with old films and establishment of no growth over at least a 2‐yr period 32. 3) If the nodule contains fat density or a benign pattern of calcification such as central nidus-type, popcorn, laminated or diffuse (fig. 12⇓) 33. Note should be made that eccentric or stippled calcification is seen in ∼10% of lung cancers 76. An appropriate history such as fever or chest pain may promote the likelihood of a benign process such as focal pneumonia or an infarct presenting as an SPN. A repeat radiograph should be performed at 2–6 weeks to assess resolution 76.
Computed tomography scanning, densitometry and enhancement
CT scanning can further refine the detection of calcification and fat within nodules. A total 22–38% of noncalcified nodules on chest radiographs appear calcified on CT 76. Using CT densitometry, a “pixel map” of a nodule can be created with Hounsfield Unit (HU) values, >200 being indicative of calcification 77, 78. Only characteristic patterns of calcification such as central, diffuse, laminar or popcorn are indicative of benignity 33. The presence of fat (−40–−120 HU) or calcification or a combination of the two has been shown to correctly identify 30 of 47 patients (64%) with hamartomas on 2‐mm section CT in one series 79. However, at least one-third of hamartomas in this series contained neither fat nor calcium leading to an indeterminate assessment.
Changes in attenuation after intravenous contrast administration at CT can also be used to distinguish benign from malignant parenchymal nodules. In a recent study of 356 nodules (5–40 mm) containing neither fat nor calcification, enhancement of <15 HU postcontrast administration was strongly predictive of benignity 80. By retrospectively reducing the cut-off threshold to 10 HU it was possible to increase the technique's sensitivity in excluding malignancy from 98 to 100%.
Malignant nodules
A nodule size >3 cm is associated with malignancy in 93–99% of cases 81. If the nodule is spiculated (fig. 13⇓) 88–94% will be malignant 82–84 although 11% of malignant nodules do have distinct margins 74. The presence of calcification in larger (>3 cm) and spiculated nodules should not be viewed as indicative of benignity.
Indeterminate nodules
Small size should not be used as a discriminator for exclusion of malignancy. One in seven nodules <1 cm in size have been shown to be malignant 81 and in a recent study of nodules resected at video-assisted thoracoscopic surgery, 31% of nodules <1 cm in size in patients with no known malignancy were malignant 85. Cavitation and lobulation are not helpful discriminators in favour of malignancy as granulomas and hamartomas can both have these appearances 74.
Central tumours
Distinct from the SPN, central lung cancers often present radiographically as a hila mass or as collapse and consolidation of lung beyond the tumour with accompanying volume loss. Air bronchograms may be seen at CT 17.
Differentiating central tumours from distal collapse can be difficult but is facilitated by bolus contrast administration followed by prompt CT scanning at the level of abnormality (fig. 14⇓). The lung is appreciably enhanced whilst tumour enhancement is minimal and delayed. The most marked difference between the two is seen from 40 s to 2 min after contrast injection 86.
Differentiating central lung tumours from mediastinal masses can also be problematic. In a study of 90 central lung and mediastinal masses, the single most useful CT finding in distinguishing between the two was the “mass-lung interface”. Marginal spiculation, nodularity or irregularity between the mass and the surrounding lung almost always indicated the mass had arisen in the lung. A smooth interface suggested that the mass was mediastinal in location. A notable exception was Hodgkin's lymphoma which may occasionally cross the pleura, invade the lung and result in a poorly marginated mass, mimicking a lung mass 87.
The following features can be viewed as suspicious for an obstructing neoplasm when associated with a pneumonia. 1) The “S” sign of Golden, indicating a fissure deviated around a central tumour mass (fig. 15⇓). 2) Pneumonia confined to one lobe (or more if supplied by a common, obstructed bronchus) especially if >35‐yrs-old and accompanied by volume loss or mucus filled bronchi with no air bronchograms present 17. In an analysis of 50 patients with segmental or lobar atelectasis, 27 (54%) were caused by an obstructing tumour, all of which were detected at CT 88. 3) Localized pneumonia that persists for >2 weeks or recurs in the same lobe.
Hila enlargement is a common presenting feature in patients with lung cancer 17. In the Mayo Clinic series, 38% of patients with lung cancer had a hila or peri-hila mass 89. More recently, 14 of 25 patients (56%) with CT performed for an abnormal hilum were found to have bronchogenic carcinoma 90. The presence of a tumour mass or enlarged lymph nodes will give a dense hilum. Generally speaking the more lobular the shape the more likely that adenopathy is present 17.
Staging nonsmall cell lung cancer
The revised international system for staging lung cancer 4 incorporates the tumour, node, metastasis (TNM) subset system (tables 2 and 3⇓⇓) and shows improved survival rates with more accurate staging and appropriate selection of patients for definitive surgical treatment by distinguishing the IIIa from the IIIb group (table 4⇓). Percentage survival at 5 yrs by clinical stage for the more advanced stages remains poor, emphasizing the importance of early detection.
The overall UK 5‐yr survival of only 5.3% serves to underline the preponderance of advanced-stage disease at presentation 3. Precise tumour (T) and nodal (N) staging is imperative as it determines subsequent treatment, especially when considering neo-adjuvant therapy for IIIa and IIIb disease. Only approximately one-half of the TNM stages derived from CT agree with operative staging, with patients being both under and over staged 91, 92. However, quick access to investigation, high histological confirmation rates (at bronchoscopic/transthoracic biopsy or at thoracotomy), routine CT scanning and review of every patient by a thoracic surgeon is known to substantially increase successful surgical resection 93.
Tumour status
The distinction between T3 and T4 tumours is critical because it separates conventional surgical and nonsurgical management 17. T4 tumours may be readily identified by virtue of their invasion of a vertebral body (fig. 16⇓), obvious invasion of the mediastinum or heart (fig. 17⇓) or the presence of lung parenchymal metastases. T3 tumours can however be more difficult to grade principally because of the difficulties of distinguishing simple extension of the tumour into the mediastinal pleura or pericardium (T3) from actual invasion (T4).
Mediastinal invasion
Minimal invasion of mediastinal fat is considered resectable by many surgeons 94. Contact with the mediastinum is not enough to diagnose mediastinal invasion 17. In Glazer's series of 80 CTs considered indeterminate for direct mediastinal invasion, 60% were resectable at thoracotomy with no evidence of mediastinal invasion, 22% did invade the mediastinum but were still technically resectable and only 18% were nonresectable 95. In fact only one of the 37 masses was not resectable provided that the pre-operative CT demonstrated at least one of the following: 1) ≤3 cm contact of the mass with the mediastinum; 2) <90° contact with the aorta; 3) fat visible between the mass and mediastinal structures. Importantly however, this information does not identify inoperable tumours (thus avoiding unnecessary thoracotomy) because ∼50% of the technically resectable tumours had >3 cm of mediastinal contact or loss of the clear fat plane. Artificial pneumothoraces have been used to improve detection of both mediastinal and chest wall invasion by examining whether or not the pleura peels away from the relevant structure. Although one study demonstrated 100% accuracy for chest wall invasion, its accuracy for mediastinal involvement was only 76% 96. Another study was 100% sensitive for mediastinal and chest wall invasion but only 80% specific 97. This again indicated that the technique cannot be categorical about the presence of unresectability.
The Radiologic Diagnostic Oncology Group 98 compared CT and MRI in 170 patients with NSCLC, 90% of whom went on to thoracotomy. There was no significant difference between the sensitivity of the two modalities (63% and 56% respectively) or the specificity (84% and 80%) for distinguishing between T3–4 and T1–2 tumours, except when receiver operating characteristic analysis was performed on the statistics. These showed that MRI is better than CT at diagnosing mediastinal invasion. MRI is particularly useful in determining invasion of the myocardium or tumour extension into the left atrium via the pulmonary veins 76.
Chest wall invasion
CT assessment of tumour chest wall invasion is variable with quoted sensitivities ranging from 38–87% and specificities from 40–90% 94. Invasion of the chest wall by a mass results in a T3 score. This does not mean the mass is irresectable per se but en bloc resection of the mass and adjacent chest wall is necessary which carries an associated increase in mortality and morbidity 99. As well as the technique of inducing artificial pneumothoraces as described earlier, dynamic expiratory multisection CT (viewed as a cine loop) has also been evaluated. In a study of 15 patients, this was found to be 100% accurate for chest wall and mediastinal fixation at pathological examination 100. With conventional CT imaging, the only reliable criterion for establishing definite invasion is bony destruction with or without tumour mass extending between the ribs and into the chest wall (fig. 18⇓) 94.
Ultrasound has been cited as an additional technique for chest wall assessment (fig. 19⇓). In a series of 120 patients with contiguity between the tumour and the chest wall at CT, 19 patients were judged to have invasive tumour on ultrasound with a sensitivity and specificity of 100% and 98% respectively as compared with operative findings 101.
MRI is a useful technique in establishing chest wall invasion. It relies on the demonstration of infiltration or disruption of the normal extra pleural fat plane on T1‐weighted images or parietal pleural signal hyperintensity on T2 weighting. The diagnostic yield is further improved by intravenous gadolinium contrast medium 48. Sagittal and coronal MRI better display the anatomical relationships at the lung apex as opposed to axial CT (fig. 20⇓). In superior sulcus or Pancoast tumours detection of tumour invasion beyond the lung apex into the brachial plexus, subclavian artery or vertebral body by MRI has been found to be 94% accurate as opposed to 63% for CT 102, 103, although multislice CT with nonaxial reconstruction may improve this figure. Surface coils and thin sections (5 mm) are advised for MRI of such tumours.
Pleural invasion
Effusions in lung cancer patients can be benign, especially with a postobstructive pneumonia or malignant due to pleural metastases, often characterized by pleural nodularity 94. Such an effusion renders the tumour T4 and irresectable, though this should be confirmed by thoracocentesis or pleural biopsy.
Nodal status
The most important predictor of outcome in the majority of patients with lung cancer limited to the chest is the presence or absence of involved mediastinal lymph nodes 17. N3 nodal disease is not an option surgically whilst the management of N2 disease is debatable. Mediastinoscopy and CT are recognized to be the most valuable techniques for evaluation of mediastinal lymph node metastases 104 but the arrival of PET has begun to influence patient management in the limited number of centres where it is available.
The enthusiasm for the usefulness of CT in assessing nodal status grew throughout the 1980s. In 1984, Libshitz and McKenna 105 demonstrated CT sensitivity and specificity of 67% and 66% respectively using a nodal size of 1 cm to distinguish between benign nodes and those seeded with metastases. In 1988 Staples et al. 106 demonstrated 79% sensitivity and 65% specificity for CT using a 1‐cm long axis nodal cut-off measurement. A meta-analysis in 1990 of 42 CT studies assessing mediastinal lymph node metastases from NSCLC described an overall sensitivity of 0.79, a specificity of 0.78 and an accuracy of 0.79 107. However, in 1992 McLoud et al. 108 using a nodal short axis measurement of 1 cm in 143 patients, returned to less inspiring figures of 64% sensitivity and 62% specificity, respectively. These studies 105, 106, 108 all examined patients with presumed operable lung cancer in whom complete nodal sampling was performed either at mediastinoscopy or thoracotomy. Both Libshitz and McKenna 105 and McLoud et al. 108 observed an increase in false-positive nodes in patients with obstructive pneumonia. McLoud et al. 103 also found that 37% of nodes, which were 2–3 cm in diameter, did not contain metastases at thoracotomy. More recently in a study of hila and mediastinal nodes at CT compared to pathological examination, sensitivities and specificities for metastatic involvement were only 48% and 53% with an overall accuracy of 51% 92. Despite these statistics, CT is still recommended as the standard strategy for the investigation of lung cancer by the Canadian Lung Oncology Group 109 after the study of 685 patients, CT and mediastinoscopy in all patients proving too expensive. They recommended that mediastinoscopy and biopsy be reserved for nodes with a short axis diameter of >1 cm in size (fig. 21⇓). Further refinements of indications for mediastinoscopy have been recommended with its omission in patients with T1 lesions and negative nodes at CT, unless the cell type is adeno- or large cell carcinoma 104. However, using a CT short axis diameter of 1 cm, Seely et al. 110, whilst examining 104 patients with T1 lesions found nodal metastases at surgery in 21% of cases of which one-third were squamous cell carcinoma.
Others suggest that a negative nodal CT scan does not require mediastinoscopy because even if micro-metastases are present, these patients can expect to have better survival if treated surgically than those denied such treatment 76. Also N2 disease not apparent on CT has been shown to be resectable with up to 30% 5‐yr survival 16, 94.
Hila nodes (N1) can usually be resected from hila vessels. Therefore, although pre-operative detection of hila nodes is useful, it is not generally crucial in directing surgical treatment. Moreover, the presence or absence of hila node metastases is an unreliable indicator of mediastinal nodal metastases (N2 disease) 111, 112.
CT may help to serve as a road map to guide fibreoptic bronchoscopy and biopsy and help identify enlarged nodes that are beyond the reach of the mediastinoscope 16. It also alerts the surgeon to the presence of anatomical anomalies. No significant difference has been found between the ability of CT and MRI to detect N2 or N3 mediastinal metastases 98. The combination of respiratory movement artefact and poorer spatial resolution 47 inherent with MRI can mean that small discrete nodes as seen on CT can appear as a larger, indistinct, single nodal mass on MRI, leading to the erroneous diagnosis of nodal enlargement. MRI is also poor at detecting nodal calcification and may thus misclassify enlarged benign nodes as malignant 94.
Metastatic status
A meta-analysis of 25 studies evaluating clinical examination and imaging findings (CT head, abdomen or bone scintigraphy), found the risk of metastases detected by imaging to be <3% if clinical examination is normal 113. If clinical examination is positive for metastatic disease then metastases will be found by imaging in ∼50% of patients. Sider and Horejs 114, found extrathoracic metastases in 25% of patients with stage I disease at thoracic CT, brain 11%, bone 8%, liver 6% and adrenals 6% (some patients having more than one site of metastatic spread). Clinically occult metastases were present in only 4% of patients. Grant et al. 115, found distant metastases in patients with no CT evidence of mediastinal disease spread in three of 114 patients (2.5%). Another meta-analysis of 16 studies found that 113 of 2,426 potentially operable patients (4.7%) became inoperable as a consequence of findings at CT scanning of the head and abdomen, ultrasound of the abdomen or scintigraphy of the bone and liver 116.
Liver imaging
Quint et al. 117, found distant metastases in 21% of all NSCLC patients. Relative frequencies were brain 10%, bone 7%, liver 5% and adrenals 3%. Isolated liver metastases were uncommon whilst metastases isolated to the brain were more common leading to the recommendation that CT scanning of the abdomen was not an effective screening method if chest CT is performed.
Imaging of the liver by CT or ultrasound in the absence of clinical signs, symptoms or laboratory abnormalities is controversial and generally not recommended 76. However, if the adrenals are routinely included on the CT chest scan, as is common practice, then the liver is included by default.
Brain imaging
Two studies have identified 21–64% of brain metastases to be clinically occult prior to CT scanning 118, 119. Kormas et al. 120, found metastases in 3% of 158 pre-operative patients after negative clinical and laboratory examination. These and other studies 115 recommend CT of the brain routinely in pre-operative patients (fig. 22⇓). More recently however, using a standardized clinical neurological examination as opposed to the Karnofsky et al. 121 performance scale used in previous studies, Colice et al. 122 found that routine CT of the brain was not indicated with a normal clinical examination. Knowledge of the primary tumour cell type may be helpful in reaching a decision. A recent meta-analysis 113 has found that adenocarcinoma and SCLC are statistically more likely to metastasize to the brain than squamous cell carcinoma. Finally, in a study using contrast enhanced MRI in patients suspected of having surgically resectable NSCLC, localized to the lung or lung and regional nodes, occult brain metastases were identified in 17% of patients with primary tumours >3 cm 123.
Adrenal imaging
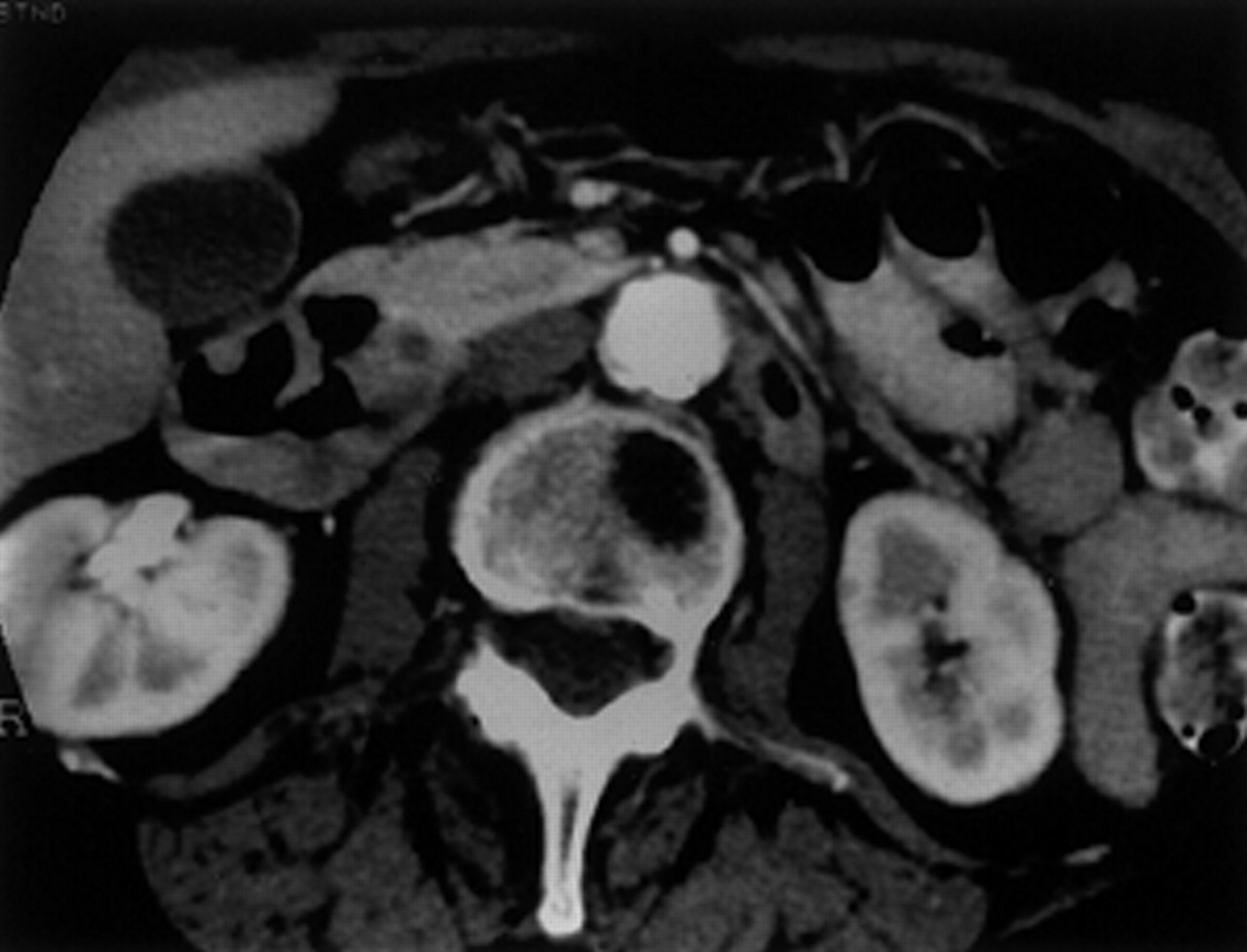
In one meta-analysis study up to 7% of patients with carcinoma of the bronchus had adrenal metastases 113. However, up to 10% of the general population have benign adrenal adenomas 32. It has been recommended that CT of the adrenals be performed as part of a staging CT of the chest 16. It involves a minimum amount of extra time, slices and dose to the patient, and is the most cost-effective strategy for evaluating an adrenal mass in a patient with newly diagnosed NSCLC 124. Gillams et al. 125 found 4% of 546 patients with lung cancer had solid adrenal tumours. Of these, 23% were proven to be due to malignant infiltration. Benign adenomas tended to be <2 cm in size, of low attenuation, well defined or to involve only part of the gland. Malignant glands tended to be >5 cm and of irregular or mixed attenuation (fig. 23⇓). It was recommended that all indeterminate glands i.e. 2–3 cm, undergo fine needle aspiration (FNA) in patients being considered for surgery. This approach is supported elsewhere 16, 32 but it should be noted that MRI can provide additional information via chemical or phase shift-imaging regarding the possibility of benignity in such adrenal masses 126, 127. PET may also have a role to play and has been shown to have a sensitivity of 100% and a specificity of 80% in the detection of metastatic adrenal infiltration in a study of patients presenting with bronchogenic carcinoma and an adrenal mass 128.
Bone imaging
Most bony metastases are symptomatic and bone scintigraphy offers a quick and inexpensive survey of all the bones that is sensitive if not very specific 129. Alternatively, the presence of a pathological fracture, raised serum alkaline phosphatase and calcium or other nonspecific findings of metastatic disease should similarly prompt a bone scan 16. Metastases may also be detected on staging thoracic CTs (fig. 24⇓).
Lymphangitis carcinomatosa
Malignant infiltration of the lymphatics and perilymphatic connective tissue is typically asymmetrical and nodular and must be differentiated from left ventricular failure. It is best demonstrated on HRCT scanning (fig. 25⇓).
Staging small cell lung cancer
SCLC is distinguished from NSCLC by its rapid tumour doubling time, development of early widespread metastases and almost exclusive occurrence in smokers 130. It is divided into two stages: limited disease, which is confined to the ipsilateral hemithorax within a single, tolerable radiotherapy port and extensive disease which covers all other disease including distant metastases. Systemic therapy is required for all patients with SCLC, even those with limited disease. Mediastinal radiotherapy is not always indicated in patients with extensive disease making the distinction between the two stages important. To avoid an exhaustive search for extensive disease (e.g. chest, liver, adrenal and cranial CT, bone scans, marrow aspirates etc.) an alternative approach is to allow clinical symptoms to direct imaging, terminating on the discovery of extensive disease 130. Given the fact that cranial CT in SCLC is positive in ∼15% of patients at diagnosis, one-third of whom are asymptomatic and that early treatment of brain metastases yields a lower rate of chronic neurological morbidity, it seems reasonable to begin any extrathoracic staging with brain imaging 32, 130.
Image guided needle biopsy
Transthoracic needle biopsy of a primary lung tumour is controversial when considering a solitary nodule or mass. A negative biopsy needs repeating and the patient will invariably proceed to surgery unless a positive benign result is obtained. Biopsy is useful in determining cell type in inoperable disease to guide further therapy and is essential to confirm the presence of distant metastatic disease.
Needle biopsy is usually performed under either ultrasound or CT guidance. Ultrasound guided biopsy is quick and allows the operator to guide the needle under direct vision but can only be used with peripheral tumours that abut the pleura or invade the chest wall. It is then usually possible to obtain a tissue core using an 18‐gauge cutting needle although FNA may be used. CT guided biopsy takes longer and systemic analgesia and sedation may be necessary to maintain patient compliance.
CT affords good visualization of all thoracic structures and CT guided biopsy has an accuracy for diagnosing malignancy of 80–95% 131, 132. It is the procedure of choice for sampling peripheral nodules (<2 cm in diameter) as the yield for transbronchial needle biopsy, in the absence of an endobronchial lesion, falls from 92–95% to 50–80% 132. FNA is the preferred sampling method of parenchymal nodules in order to reduce the incidence of complications and is known to have a similar sensitivity in detecting malignancy as core biopsy 131. However, small tissue fragments for histological evaluation can generally be obtained with 19–22 gauge needles in 40–75% of patients 132. Such evaluation is valuable because it lends confidence to a cytological diagnosis of cancer, to cell-type determination and to the reliability of a negative result 131, 132. When a cavitatory or necrotic lesion is encountered, sampling of the wall is recommended to obtain viable tumour material. A single negative biopsy does not exclude malignancy and should prompt a repeat biopsy.
When performing biopsies of mediastinal lesions it is usually possible to use an 18‐gauge cutting needle after selecting a safe route. This is especially important in the diagnosis of lymphomas. Cutting needles are also employed in the biopsy of presumed hepatic and adrenal metastases although FNA of the latter may be necessary with smaller lesions (figs. 26 and 27⇓⇓).
Conclusion
Lung cancer is a common disease that has a poor prognosis. Survival is inversely proportional to the stage, with early detection and diagnosis being the key to achieving surgical cure. Cross-sectional imaging is now the main radiological means of assessment. Chest radiography is still important, and frequently suggests the first diagnosis, but its relative insensitivity has led to CT scanning being currently evaluated in screening studies.
Currently there is little to choose between CT and MRI in staging the disease although CT is more widely available and less expensive. PET imaging offers heightened sensitivity for both detection of the primary malignancy and disease spread, although it is not 100% accurate and is only available in a few centres. CT scanners are becoming more sophisticated in design and versatility and seem likely to remain the principal imaging modality for this disease in the near future.

a) Diffuse alveolar shadowing in the right lower lobe of a 58‐yr-old male presenting as an unresolving pneumonia. b) Air bronchograms (black arrows) and low attenuation lucencies (open arrow) in apical “consolidation”, later confirmed as bronchoalveolar carcinoma.

A 50‐yr-old female with irregular cavitating squamous cell carcinoma in the right upper lobe (arrows).

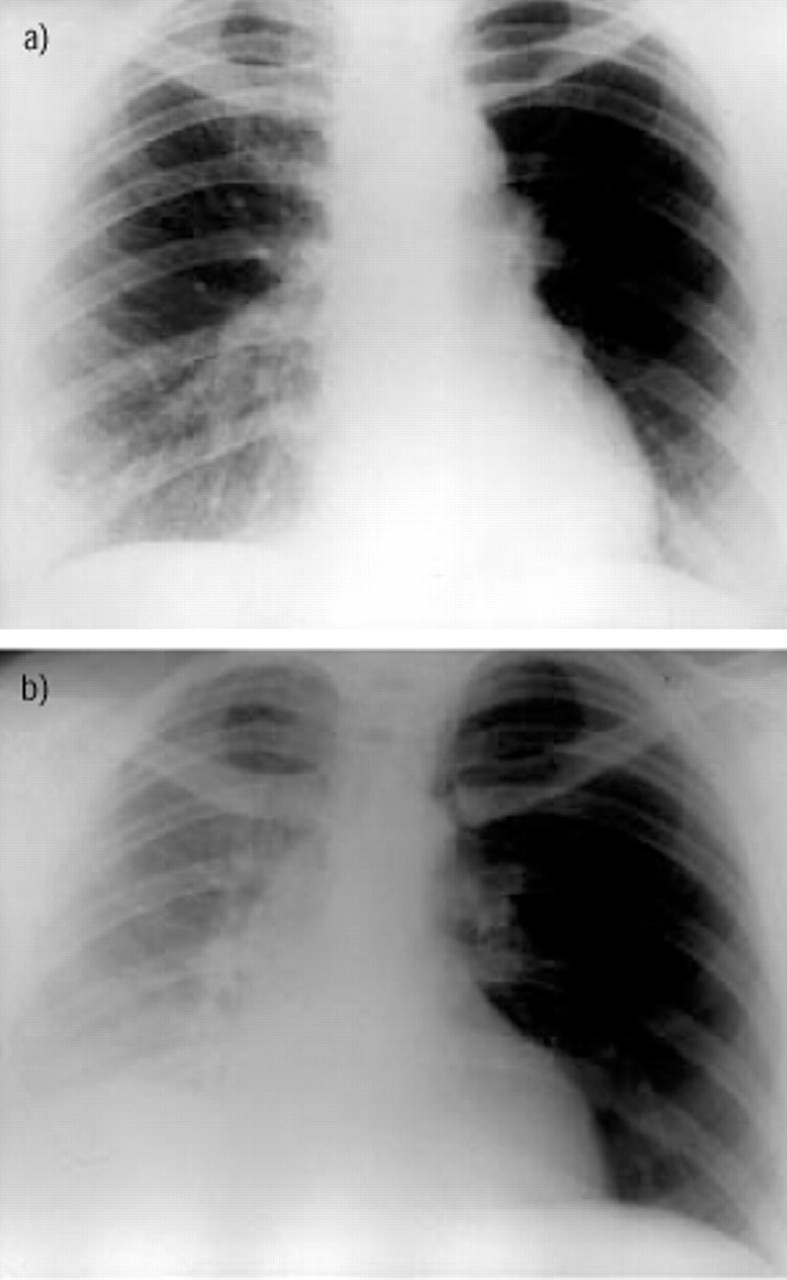
a) A 55‐yr-old dyspnoeic female. Chest radiograph demonstrating widened mediastinum particularly on the right with reduced vascularity of the right lung. b) Contrast enhanced computed tomography showing central mediastinal mass invading the right pulmonary artery. Small cell carcinoma was confirmed on percutaneous biopsy.
a) Inspiratory film with asymmetrical vascularity. b) Expiratory film confirming air trapping due to carcinoid tumour in the left main bronchus.

Increased retrocardiac density due to left lower lobe collapse with inferomedial displacement of the hilum.

a) Coronal reformat from multislice computed tomography (CT) demonstrating mediastinal lymph nodes (arrow) and a necrotic tumour mass within the lung. b) Three-dimensional-reconstruction of a lung tumour with pleural tag (arrow) (images courtesy of T. McArthur, Dept. of Radiology, University College Hospitals, London). c) Thin slice reconstruction in the axial plane from spiral CT data permits the correct identification of an inhaled fish bone (arrow), in a different patient, presumed to be a tumour at bronchoscopy.

Necrotic mediastinal lymph nodes with irregular enhancing rims (arrows).

a) Mediastinal mass narrowing left lower lobe bronchus and invading left atrium. b) Distal fluid-filled bronchi (arrows) are seen in the collapsed lower lobe due to the proximal tumour.

Coronal magnetic resonance imaging showing an adenocarcinoma in a young male infiltrating the aortopulmonary window. There is loss of the fat plane against the aorta (arrows) and invasion of the main pulmonary artery (arrowhead).
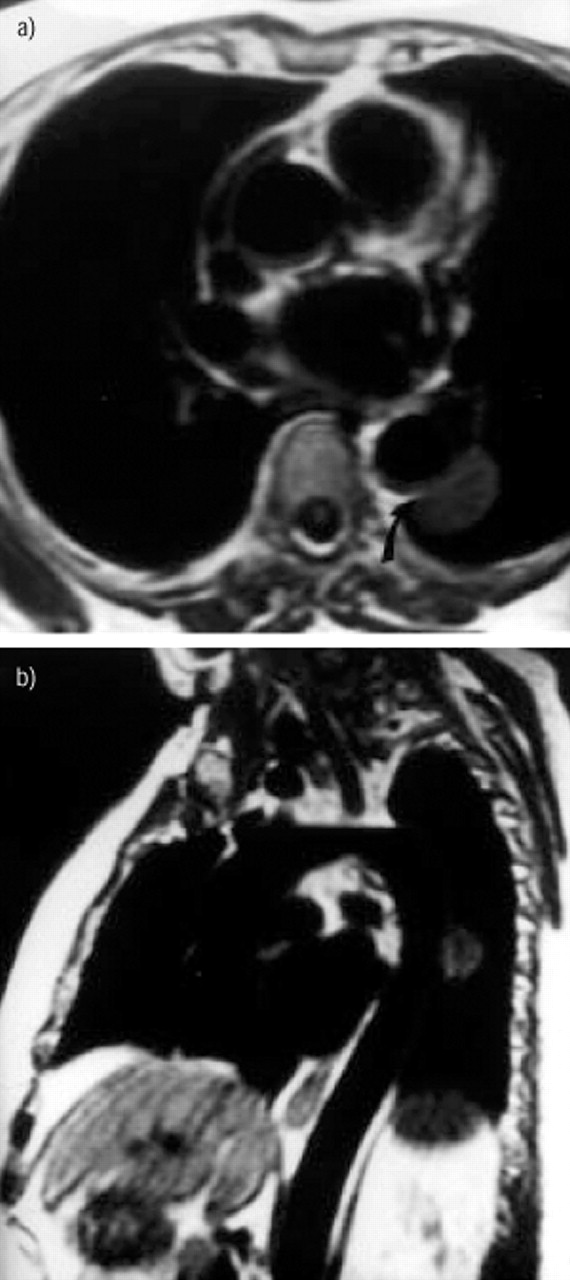
T1‐weighted images demonstrating superior ability of magnetic resonance imaging in demonstrating loss of fat plane (arrow) in a) axial and b) sagittal planes.

Avid uptake of 18F‐2‐deoxy‐d‐glucose in left apical tumour (arrow).

Diffusely calcified, well-defined nodule typical of a hamartoma.

Spiculated mass typical of a carcinoma.

a) Collapse of the left lung with mediastinal shift and a right middle zone nodule (arrow). b) Perihilar low attenuation adenocarcinoma (arrows) with distal enhancing collapsed lung in same patient.

Central mass with Golden “S” sign of proximal tumour (arrows) and distal collapse.

a) Rib erosion (large arrow) due to peripheral tumour (small arrows) suggesting at least T3 disease. b) Corresponding computed tomography showing mass eroding rib and vertebral body (arrows) confirming T4 status and inoperability.

Large central mass (arrows) narrowing left main bronchus and encasing left pulmonary artery, indicating T4 status. A pleural effusion is noted.
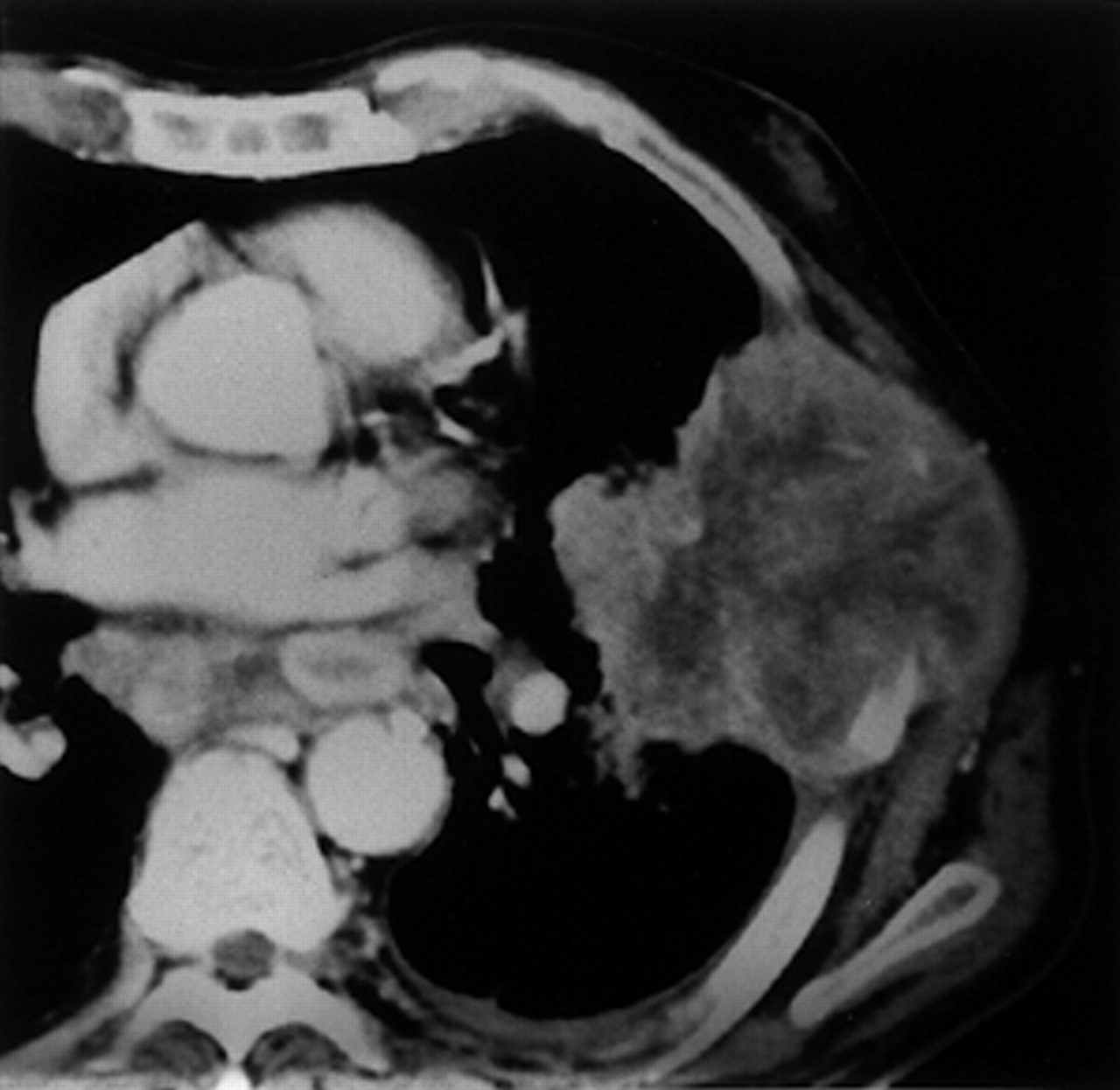
Frank chest wall invasion by large peripheral tumour.

a) Computed tomography scan suggesting infiltration of pleural fat (arrows). b) Lack of movement relative to chest wall (arrows) confirms invasion.

Coronal T1‐weighted magnetic resonance imaging showing subtle Pancoast tumour (open arrow) with extension into the superior sulcus and erosion of the adjacent vertebral body (arrow).

Middle-aged-female with a) right hilar mass (arrow) and b) equivocal precarinal lymph node (arrow). c) Positron emission tomography (PET) scan shows increased uptake in mediastinal nodes (arrows) and small peripheral nodule (open arrow). Biopsy of hilar mass confirmed nonsmall cell lung cancer. (PET images courtesy of J. Bomanji, Institute of Nuclear Medicine, University College London).

Computed tomography scan of enhancing cerebral metastasis with marked oedema and mass effect.

Massive left adrenal (open arrow) and hepatic metastases (arrows). M1 disease, stage IV.
Vertebral body metastasis.

Characteristic septal nodular thickening on high-resolution scans typical of lymphangitis carcinomatosa.

Versatility of transthoracic needle biopsy with needle tip in a) mediastinal mass (note safe approach) and b) peripheral solitary nodule.

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
a) Low attenuation adrenal mass (arrows) with normal right adrenal (open arrow) which at biopsy, b) confirmed metastatic deposits.
Data from low-dose computed tomography screening trials
Tumour, node, metastasis (TNM) classification
Staging classification
Cumulative percentage survival at 5‐yrs post-treatment by clinical stage
Footnotes
-
↵Previous articles in this series: No. 1: Baldacci S, Omenaas E, Oryszcyn MP. Allergy markers in respiratory epidemiology. Eur Respir J 2001; 17: 773–790. No. 2: Antó JM, Vermeire P, Vestbo J, Sunyer J. Epidemiology of chronic obstructive pulmonary disease. Eur Respir J 2001; 17: 982–994. No. 3: Cuvelier A, Muir J‐F. Noninvasive ventilation and obstructive lung diseases. Eur Respir J 2001; 17: 1271–1281. No. 4: Wysocki M, Antonelli M. Noninvasive mechanical ventilation in acute hypoxaemic respiratory failure. Eur Respir J 2001; 18: 209–220. No. 5: Østerlind K. Chemotherapy in small cell lung cancer. Eur Respir J 2001; 18: 1026–1043. No. 6: Jaakkola MS. Environmental tobacco smoke and health in the elderly. Eur Respir J 2002; 19: 172–181.
- Received September 11, 2001.
- Accepted September 11, 2001.
- © ERS Journals Ltd
References









