





Abstract
Dynamic hyperinflation contributes to exertional breathlessness and reduced exercise tolerance in chronic obstructive pulmonary disease (COPD) patients. This study examined whether oxygen supplementation results in a dose-dependent decrease in hyperinflation associated with functional and symptomatic improvement.
Ten severe COPD patients without clinically significant oxygen (O2) desaturation during exercise, and seven healthy subjects, performed five exercise tests at 75% of maximally tolerated work rate. Inspired oxygen fraction (FI,O2) was varied (0.21, 0.3, 0.5, 0.75 and 1.0) among tests in a randomized order. Ventilation (V'E) was measured, and end-inspiratory (EILV) and end-expiratory (EELV) lung volume changes were assessed from inspiratory capacity manoeuvres.
In the patients, compared to room air, endurance time increased with FI,O2=0.3 (mean±sem 92±20%) and increased further with FI,O2=0.5 (157±30%). At isotime, compared to room air, there were significant reductions in dyspnoea score, EELV, EILV, V'E and respiratory frequency (fR) with FI,O2=0.3. Improved endurance time negatively correlated with change in EELV (r=0.48, p=0.002) and EILV (r=043, p=0.005). The dyspnoea rating decrease correlated with fR decrease. In healthy subjects, smaller V'E and fR decreases were observed at FI,O2=0.5, accompanied by more modestly increased endurance.
Oxygen supplementation during exercise induced dose-dependent improvement in endurance and symptom perception in nonhypoxaemic chronic obstructive pulmonary disease patients, which may be partly related to decreased hyperinflation and slower breathing pattern. This effect is maximized at an inspired oxygen fraction of 0.5.
- chronic obstructive pulmonary disease
- dose-response effect
- dynamic hyperinflation
- endurance
- exercise
- oxygen
A. Somfay is a visiting scientist from the Dept of Pulmonology, Albert Szent-Györgyi Medical University, Szeged-Deszk, Hungary and is partly supported by the Hungarian Soros Foundation (Budapest), the Foundation for Hungarian Pulmonology (Budapest) and the Foundation for Quality Care of Patients with Lung and Heart Diseases (Deszk). J. Porszasz is a visiting scientist from the National Institute of Occupational Hygiene and Health (Budapest). S.M. Lee is a visiting scientist from the Dept of Internal Medicine, Eulji Medical College, Seoul, Korea and is the recipient of a World Health Organization fellowship.
Dyspnoea during exercise is a predominant symptom in most patients with chronic obstructive pulmonary disease (COPD), and thus has a major impact on quality of life. The mechanism of exertional breathlessness in COPD has been linked to expiratory airflow obstruction (measured as forced expiratory volume in one second (FEV1) 1. Recently, it has become evident that while exercise capacity is often poorly predicted by FEV1 2, there is a close correlation between the sensation of dyspnoea and inspiratory muscle load 3. As COPD patients exercise, end-expiratory lung volume (EELV) and end-inspiratory lung volume (EILV) increase in order to prevent dynamic airway closure during expiration and allow higher expiratory flows, thus delaying the onset of mechanical limitation of ventilation 4. This dynamic hyperinflation (DH) exerts a mechanical disadvantage on the respiratory muscles, by pushing the tidal breathing level to a stiffer range of the pressure/volume curve and placing the inspiratory muscles on a less economic part of their length-tension relationship 5. The net effect is a constrained tidal volume (V'T), which encroaches on the inspiratory reserve volume (IRV), thus leading to a greater reliance on tachypnoea to increase ventilation, but this compensatory mechanism soon fails as it causes even further DH. The consequence is an increased elastic work of breathing which contributes to the perceived inspiratory difficulty 6, 7.
The beneficial effects of oxygen in the treatment of COPD patients with hypoxaemia have been recognized for decades. The Medical Research Council 8 and Nocturnal Oxygen Therapy Trial 9 studies established clear-cut evidence for the value of oxygen therapy; it is the only proven life-prolonging therapy so far identified for hypoxaemic patients with COPD. Supplemental oxygen also improves exercise tolerance in hypoxaemic COPD patients. In contrast to several observations in hypoxaemic COPD, there are only few studies 10–12 that demonstrate the favorable effect of oxygen supplementation during exercise in COPD patients without clinically significant hypoxaemia. The quantities of oxygen administered in these studies were different and the mechanism by which oxygen improved exercise capacity in this subgroup of COPD patients was not clearly defined. In view of recent understanding of the role of dynamic hyperinflation in exercise tolerance in COPD, it is surprising that supplemental oxygen has not been demonstrated to decrease hyperinflation during exercise 10. Moreover, a recent editorial 13 highlighted reservations regarding the usefulness of supplementary oxygen for indications other than continuous domiciliary care and called for studies to identify patients who could gain particular benefit from this treatment.
In identifying those patients who would potentially benefit from ambulatory oxygen therapy, it was the purpose of the present study to evaluate the correlates of improved exercise tolerance induced by supplemental oxygen in nonhypoxaemic COPD patients. A particular focus was placed on changes in operating lung volumes and breathing pattern. To figure out the optimal quantity of oxygen required during exercise, the dose-dependence of this effect was evaluated by studying a range of fractions of inspired oxygen (FI,O2).
Methods
Subjects
Ten clinically stable patients with severe COPD (FEV1 <40% predicted) who were no more than mildly hypoxaemic (pulse oximeter O2 saturation (Sa,O2) at rest >92% and during exercise >88%) were studied. None of them had qualified previously for ambulatory oxygen therapy. Exclusion criteria included clinically manifest cor pulmonale, severe cardiovascular comorbidity or other disease that might contribute to dyspnoea or exercise limitation. Seven healthy volunteers were also recruited. Participants' characteristics are listed in table 1⇓. The institutional review board approved the protocol and subjects gave written informed consent.
Subject characteristics.
Study design
A randomized, single blinded, controlled study was designed. All subjects had previously been familiarized with exercise testing, breathlessness ratings and inspiratory capacity manoeuvres. Based on a symptom-limited incremental cycle exercise test, performed while the subjects breathed room air, a constant work rate equal to 75% of the highest work rate achieved was selected. During the five subsequent constant work rate tests, subjects breathed compressed air, 30%, 50%, 75% or 100% oxygen, in random order. Subjects were blinded with respect to the oxygen concentration they breathed. The study was designed with three visits separated by 3–5 days. Each study day consisted of two exercise tests with an intervening 1-h recovery period. Subjects avoided caffeine, alcohol or heavy meals before testing.
Pulmonary function testing
Before exercise testing on visit 1, subjects underwent pulmonary function testing (Vmax 229 and Autobox 6200, SensorMedics, Yorba Linda, CA, USA) including spirometry, lung volumes determined by plethysmography and single-breath carbon monoxide diffusing capacity (TL,CO). In the patients, 200 µg albuterol was administered from a metered dose inhaler, 30 min before testing. Trapped air volume (TAV) was calculated as: total lung capacity (TLC, by plethysmograph)-alveolar volume (VA by single breath inert gas dilution).
Exercise testing
A symptom-limited incremental exercise test was conducted with the subject breathing room air on an electronically-braked cycle ergometer (Ergoline-800, SensorMedics). After 3 min of rest and 3 min of unloaded pedaling, work rate was increased continuously (ramp) by 5 or 10 W·min−1 for the patients and 15 or 20 W·min−1 for the healthy subjects. Constant work rate tests to symptom limitation at 75% of the peak work rate in the incremental test were carried out on the same ergometer. Pedalling rate was kept constant at 50–70 rpm. Compressed air and oxygen were blended (air-oxygen blender, SensorMedics) from gas cylinders into a 200-L meteorological balloon to be inspired during exercise. Subjects breathed through a mouthpiece attached to a low resistance, two-way, nonrebreathing valve (deadspace=80 mL) (Hans-Rudolph, Kansas City, MO, USA) whilst wearing a noseclip. Respiratory flows were measured with a calibrated mass flow sensor (SensorMedics). Minute ventilation (V'E) and gas exchange (V'O2 and V'CO2) were measured breath-by-breath with a metabolic cart (Vmax 29c, SensorMedics). Considering the uncertainties of V'O2 determination during high oxygen breathing, metabolic rate was assessed from V'CO2. Equipment was calibrated immediately before each test. Heart rate and oxygen saturation were recorded with continuous electrocardiographic (Cardiosoft, SensorMedics) and pulse oximetric (N-200 pulse oximeter; Nellcor, Hayward, CA, USA) monitoring.
Dynamic hyperinflation was evaluated from inspiratory capacity (IC) measurements. After 10 min adaptation to the mouthpiece and allowing an equilibration of oxygen concentration in the lungs, subjects were asked to perform three IC manoeuvres (“at the end of the next normal expiration, take a deep breath all the way in”), 1 min apart. Verbal encouragement was given to make a maximal effort on top of a maximal inspiration before relaxing. Volume plateau at peak inspiration (fig. 1⇓) and consistent reproducibility (±10%) were required. After collecting three reproducible IC manoeuvres (the mean of the two best was recorded as resting IC), subjects started pedalling and the manoeuvre was repeated at 2-min intervals throughout exercise and at end-exercise. With the assumption that TLC does not change with exercise in patients with chronic airflow limitation 4, changes in IC reflect dynamic shifts in operational lung volumes (EELV=TLC-IC, EILV=EELV+VT). This has been shown previously, to be a reproducible method for evaluating dynamic hyperinflation 6, 14.

a) Flow/volume and b) volume/time curves of a representative resting inspiratory capacity manoeuvre.
The modified Borg scale 15 was used to rate breathlessness at rest, every other minute throughout exercise, and at end-exercise. Maximal voluntary ventilation (MVV) was estimated as FEV1 times 40 16.
Data analysis
For each variable of interest, one way analysis of variance (ANOVA) with repeated measures was performed for values measured at the end of room air exercise and isotime values measured while breathing 30, 50, 75 and 100% oxygen during exercise. When ANOVA detected a significant main effect, post-hoc comparisons were done using the Tukey test. Linear regression analyses were made between selected variables. To find subsets of independent variables that best predicted the change in exercise endurance, Mallows' 17 Cp selection method was used. Significant differences were declared when p<0.05. Results are expressed as mean±sem, unless otherwise indicated.
Results
Demographic data were similar in the two groups (table 1⇑). Pulmonary function was normal in the healthy individuals while severe airway obstruction and moderate hyperinflation were present in the COPD patients. Peak work rate and aerobic capacity were three- and two-fold higher in the healthy subjects, respectively. At termination of incremental exercise, COPD patients were ventilatory-limited and had only mild desaturation (table 1⇑).
Operational lung volumes from rest to end-exercise during the constant work rate test increased significantly in the COPD group on room air (EELV 71.6±1.9 versus 80.9±1.7%TLC, p<0.001; EILV 82.8±1.9 versus 95.7±0.8%TLC, p<0.001). During the same transient in the control group, EELV did not change (54±3.2 versus 51.1±2.5%TLC, nonsignificant (ns)). At the end of room air exercise, compared to healthy subjects, inspiratory reserve was significantly lower in the COPD group (EILV 95.7±0.8 versus 85.4±2%TLC, p<0.001).
The time course of dynamic changes in operational lung volumes while breathing different O2 concentrations throughout constant work rate exercise in a representative patient and a healthy subject are shown in figure 2⇓. In the patient, EELV increased considerably and EILV was close to TLC at the end of normoxic exercise (which lasted only 2 min). Increasing FI,O2 resulted in attenuation of dynamic hyperinflation and dramatically improved exercise endurance time. In the healthy subject, changes in lung volumes while breathing oxygen were similar to those seen while breathing room air.

Time course of changes in lung volumes during exercise with different oxygen (O2) concentrations in a) a patient and b) a healthy subject. Solid symbols represent end-inspiratory lung volume and open symbols represent end-expiratory lung volume. ○: room air; □: 30% O2; ▵: 50% O2; ▿: 75% O2; ⋄: 100% O2. TLC: total lung capacity.
Exercise responses while breathing the five different O2 concentrations are summarized in tables 2 and 3⇓⇓. Not shown in tables 2 and 3⇓⇓ are the recorded responses at rest and at end-exercise. No significant differences in any of the physiological variables were observed as a function of FI,O2 either at rest or at end-exercise in either subject group.
Responses to constant work rate exercise with different inspired oxygen fractions in patients with chronic obstructive pulmonary disease.
Responses to constant work rate exercise with different inspired oxygen concentrations in healthy subjects.
In the patients, as compared to room air values, endurance increased while breathing 30% oxygen (92±20%) which increased further with 50% O2 (157±20%). However, further FI,O2 increases did not result in additional exercise endurance increase. Compared to room air values, 30% oxygen significantly increased the isotime IC and IRV with further mild, but nonsignificant increases with 50% O2. Isotime V'E mean inspiratory flow, VT/IC and heart rate decreased while expiratory time increased significantly with 30% O2 breathing and changed no further at higher oxygen concentrations.
In the control group (table 3⇑), IC, IRV and VT/IC did not change significantly with oxygen breathing. Although 30% oxygen did not change responses significantly, an increase in endurance (by an average of 40±14%) and decrease in V'E and inspiratory flow were manifested with 50% oxygen, as compared to 21% O2 values.
The dose-response relationship between the oxygen concentration in the breathed air, and changes in lung volumes during exercise, is demonstrated in figure 3⇓. In the COPD group, 30% O2 significantly decreased both the EELV and EILV, with additional mild decrease with 50% O2. Higher FI,O2 did not cause further decreases in lung volumes. In control subjects, lung volumes did not change significantly with increasing FI,O2.
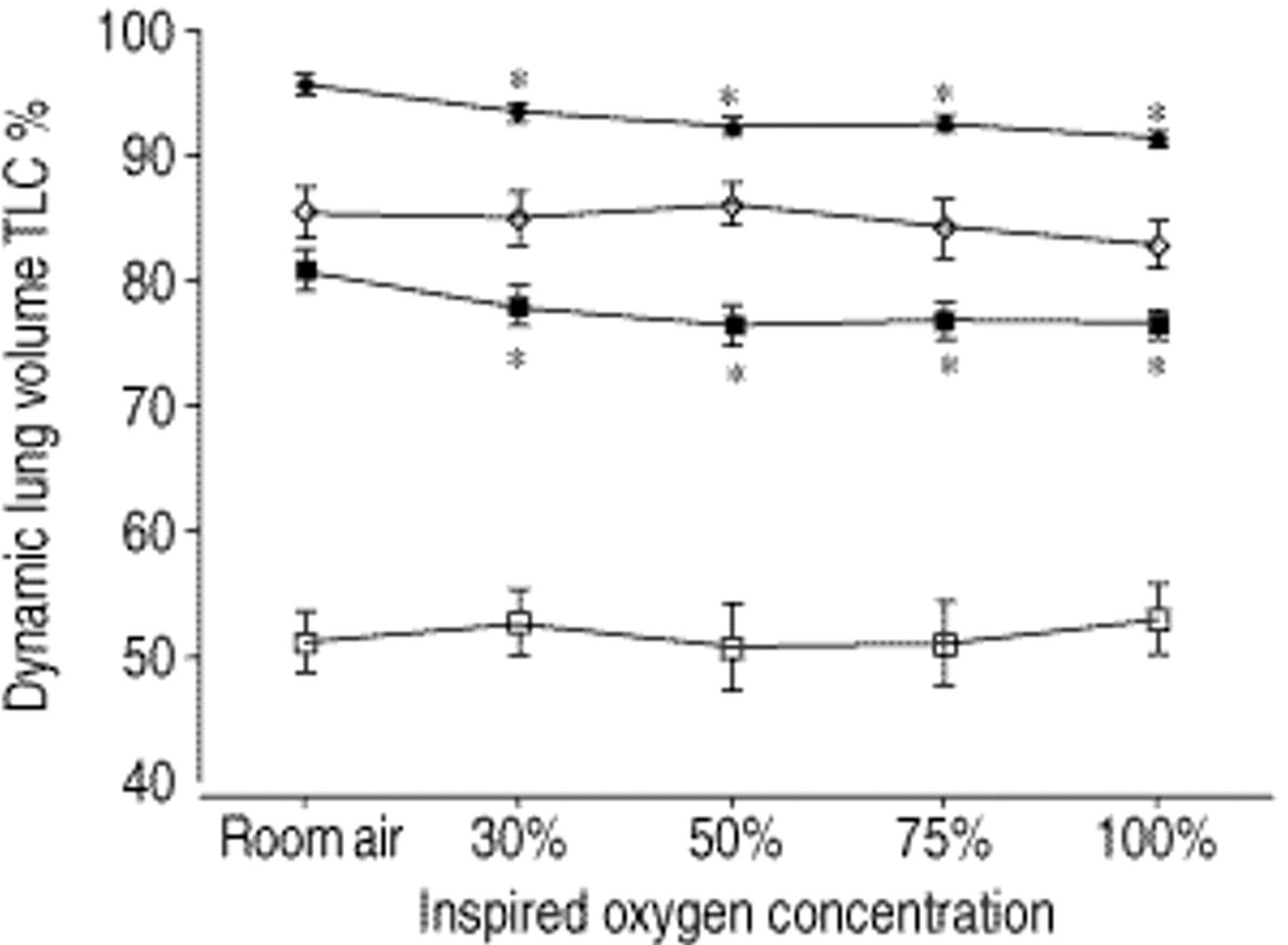
The effect of oxygen on operational lung volumes. All values (mean±sem) are at the time at which the room air test ended (isotime). ▪: end-expiratory lung volume (EELV) in chronic obstructive pulmonary disease patients (COPD); ♦: end-expiratory lung volume (EILV) in patients COPD; ⋄: EILV in healthy subjects; □: EELV in healthy subjects. TLC: total lung capacity. *: p<0.05 versus room air.
As shown in figure 4⇓, V'E. (%MVV), and respiratory rate decreased significantly with 30% O2 breathing in patients with COPD, with additional milder drop in fR with 50% O2. Change in breathing pattern became manifest at 50% O2 in the healthy subjects.

The effect of oxygen on the breathing pattern during exercise. All values (mean±sem) are at the time at which the room air test ended (isotime). V'E/MVV: minute ventilation/maximum voluntary ventilation (closed symbols); fR: respiratory frequency (open symbols); squares represent chronic obstructive pulmonary disease patients; circles represent control, healthy subjects. *: p<0.05 versus room air.
There were significant correlations between the decrease in V'E and the decrease in V'CO2 either in patients (r=0.58, p<0.001) or in healthy subjects (r=0.81, p<0.001). In COPD patients, the percentage increase in endurance time, compared to normoxic exercise time, correlated significantly with the change in EILV (%TLC) at isotime (r=0.43, p=0.005) and the changes in EELV (% TLC) at isotime (r=0.48, p=0.002) (fig. 5⇓). Smaller but significant correlations were found between the changes in operational lung volumes and changes in breathing pattern (change in EELV (% LC) versus change in fR, r=0.36, p=0.023 and change in EILV (%TLC) versus change in V'E (%MVV), r=0.38, p=0.014). The change in dyspnoea rating at isotime significantly correlated with the change in respiratory rate (r=0.35, p=0.028) and heart rate (r=0.33, p=0.036). To find a subset of independent variables that best predict the increased exercise endurance, a two-variable model including the isotime change in dyspnoea rating and IRV resulted in r=0.55 (F=0.0013, Cp=2.9).

{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
Change in endurance as a function of change in dynamic lung volumes in chronic obstructive pulmonary disease patients. All values are at the time at which the room air test ended (isotime). a) Correlation with end-inspiratory lung volume (EILV) and b) correlation with end-expiratory lung volume (EELV). Inspired oxygen fractions are 0.3 (▪), 0.5 (▴), 0.75 (▾) and 1.0 (♦). Linear regression lines are shown: EILV r=0.432, p=0.005; EELV r=0.48, p=0.002.
In the healthy subjects, there were no significant correlations between the increased endurance and the changes in isotime lung volumes or breathing pattern.
Discussion
Administration of supplemental O2 during high intensity, constant work rate exercise resulted in a dose-dependent increase in exercise endurance in patients with severe airflow limitation but without clinically significant exercise hypoxaemia. In comparison to FI,O2=0.21, average tolerated exercise duration increased by 92% at FI,O2=0.3 and by 157% at FI,O2=0.5 but increased no further at higher FI,O2. Reduced dyspnoea ratings, operational lung volumes and inspiratory flows to identical exercise tasks accompanied this improvement. The changes in breathlessness and dynamic lung volumes (EELV, EILV) were most striking at FI,O2=0.3 compared to room air isotime, though further nonsignificant improvements were detected in the lung volumes at FI,O2=0.5. These results suggest that O2 supplementation during exercise in patients with nonhypoxic COPD, results in beneficial effects on exercise endurance and the sensation of dyspnoea, at least in part, because O2 breathing decreases dynamic hyperinflation.
Since the early observation of Cotes and Gilson 18, it has been confirmed in several studies that O2 supplementation improves the exercise tolerance of COPD patients. Woodcock et al. 12 reported mildly increased exercise tolerance and reduction in breathlessness in “pink puffers” with exercise induced hypoxaemia while breathing O2 at 4 L·min−1 through nasal cannula during incremental treadmill exercise. Dean et al. 11 found that breathing 40% O2 improved exercise endurance by 40%, while O'Donnell et al. 10 documented that breathlessness decreased and endurance improved by 35% when COPD patients without severe hypoxaemia exercised while breathing 60% oxygen. Bye et al. 19 also found increased endurance when high O2 mixtures were breathed. The difference in changes in endurance among studies may relate to differences in study population or to differences in study protocol.
The dose-response relationship between increased FI,O2 and the increased exercise duration and reduced dyspnoea have not been previously defined. Evaluating the effect of different flows of supplemental O2 on exercise performance, Davidson et al. 20 reported cycling endurance time increased by 51%, 88% and 80% with nasal oxygen flow rates of 2, 4 an 6 L·min−1. A wide range of FI,O2 and found that increasing FI,O2 to 0.3 yielded substantial changes in exercise tolerance, the sensation of dyspnoea and the physiological responses to exercise. Increasing FI,O2 to 0.5 produced additional (but smaller) changes; further increases in FI,O2 produced no additional improvements. This plateauing in the dose-response relationship may reflect plateauing in receptor responsiveness (e.g. carotid body chemosensitivity, pulmonary vasodilation) at higher FI,O2. Complete abolition of hypoxic drive requires a Pa,O2 of ∼200 mmHg (26.7 kPa 21), which corresponds to an FI,O2 of 0.35 at sea level. This supports the postulation that the O2 dose plateau effect is, to some extent, related to the extinction of hypoxic ventilatory drive. Alternatively, it may concievably be the result of offsetting effects of high FI,O2: arteriolar vasoconstriction in the exercising muscles (tending to decrease O2 delivery) or cerebral vasoconstriction (tending to increase central chemoreceptor stimulation).
Despite the accumulated evidence about the benefit of O2 supplementation during exercise in COPD, contributing mechanisms to improvements in exercise endurance and breathlessness are not known with certainty. Some of the effects are related to the depression of carotid body output and resultant respiratory drive, as shown by progressive breathholding time prolongation with increasing FI,O2 22 and by the reduction of ventilation for a given work rate during exercise 23. The relationship between exercise ventilation and dyspnoea was not altered by 60% O2 breathing, but the proportional fall in ventilation during hyperoxia was found to be the strongest predictor of reductions in exertional breathlessness 10. Reduction of lactic acid production in the exercising muscles is another mechanism by which O2 supplementation may improve exercise tolerance in COPD 10. There is a consistent relationship between exercise ventilation and blood lactate levels in both healthy subjects 24 and COPD patients 10, 25.
Another possible mechanism through which reduced exercise ventilation and fR improve exercise tolerance and alleviate dyspnoea is the change in dynamic lung volumes. In COPD patients without severe hypoxaemia, O'Donnell et al. 10 found that, during exercise with breathing 60% O2, reduced EELV did not show significant correlation with improved breathlessness. In contrast, while breathing 30% O2 during exercise, the present study showed appreciable changes in operating lung volumes that are probably linked to the improved exercise tolerance. Lower fR and prolonged expiratory time allowed for fuller expiration, facilitating EELV reduction. The reduced ventilatory drive 26, 27 and the bronchodilator effect of O2 28, 29 might have contributed to this change. As VT did not change, inspiratory reserve volume, that was severely restricted during normoxic exercise, increased almost two-fold (table 2⇑). It is postulated that this leads to decreased encroachment on the flat portion of the lung's pressure/volume relationship, thus substantially reducing the work of breathing and, thereby, the sensation of dyspnoea. As a result of reduced ventilation and reduced O2 cost of breathing, more O2 became available for energizing nonrespiratory muscles, thereby contributing to the improved endurance. The correlation between the decrease in V'E and the decrease in V'CO2, both in patients and in healthy subjects, confirms this interpretation. The most striking changes were achieved with FI,O2=0.3 in patients, with some additional improvement with FI,O2=0.5. Increasing FI,O2 above 0.5 did not further improve either endurance, breathlessness or physiological response variables.
Despite demonstrating highly significant correlations, changes in operating lung volumes could “explain” only a modest portion of the variance in exercise tolerance or dyspnoea. This may be related to other (unmeasured) effects of O2 supplementation, e.g. improved respiratory muscle function 19, decreased impedance of the respiratory system 27, decreased pulmonary artery pressure 11 or reduced lactate production 10. Further, it should also be considered that scatter in the measured variables may partly be due to the effort-dependent nature of exercise endurance, the IC manoeuvre and the subjective nature of dyspnoea scoring. These measurement “noise” sources may have degraded the observed correlations.
The responses to O2 during exercise in healthy subjects were different from those of COPD patients. The change in ventilatory response was manifest only at FI,O2 of ≥0.5 with a mean decrease in V'E at isotime of ∼20%. Although these healthy subjects were not ventilatory limited during exercise and a correlation between the decrease in dyspnoea and fR was only found in the COPD group, the suppressed chemoreceptor drive may have contributed to the reduced respiratory sensation. This is in accordance with the observations of Ward and Whipp 30 concerning the relationship between respiratory sensation and peripheral chemoreflex activation during exercise in healthy individuals. Surprisingly, in healthy subjects, detection of a suppressed ventilatory response with exercise while respiring 30% O2 was not measured.
In conclusion, it has been shown that even a modest increase in the inspiratory oxygen fraction to 0.3 during high intensity constant work rate exercise, may induce decreased dynamic hyperinflation and reduced ventilatory drive in patients with severe chronic obstructive pulmonary disease who are not clinically hypoxaemic. The plateauing effect of oxygen at inspiratory oxygen fraction of 0.5 is partly related to decreasing ventilatory drive. The effects of oxygen on dynamic hyperinflation may have contributed to the observed improvement in exercise endurance and breathlessness. The observations provide a mechanistic rationale for the provision of supplemental oxygen to nonhypoxaemic chronic obstructive pulmonary disease patients during ambulation. Practical application of this observation could be the use of supplemental oxygen during rehabilitative endurance exercise training in order to allow elevated exercise intensity and, potentially, an enhanced physiological training effect in the muscles of ambulation.
Acknowledgments
The authors are grateful to L. Woodhouse for her valuable help with statistical analysis.
- Received September 19, 2000.
- Accepted March 13, 2001.
- © ERS Journal Ltd
References









